





1. Background
2. Objectives
3. Methods
3.1. Animal Study
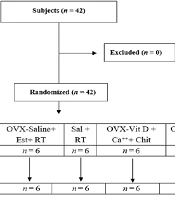
3.1.1. Experimental Groups and Treatments
3.1.2. Ovariectomy Procedure
3.1.3. Route and Time of Administration of Drugs
3.1.4. Euthanasia
3.2. Biochemical Analysis
3.3. Micro-Computed Tomography (CT) Testing
3.4. Histologic Evaluations
3.5. Quantitative Real Time-Polymerase Chain Reaction Analysis
| Gene | Primer Sequence | Size (bp) | Genebank Code | Annealing Temperature (˚C) |
|---|---|---|---|---|
| Ocn | F: GAGGGCAGTAAGGTGGTGAA | 135 | NM_013414.1 | 60 |
| R: GTCCGCTAGCTCGTCACAAT | ||||
| Alp | F: GCACAACATCAAGGACATCG | 195 | NM_013059.1 | 60 |
| R: TCAGTGCGGTTCCAGACATA | ||||
| Col1a1 | F: GAATATGTATCACCAGACGCAG | 186 | NM_053304.1 | 60 |
| R: AGCAAAGTTTCCTCCAAGAC | ||||
| GAPDH | F: GACTTCAACAGCAACTCCCAC | 652 | NM_017008.4 | 60 |
| R: TCCACCACCCTGTTGCTGTA | 1306 |
Abbreviations: Alp, alkaline phosphatase; Col1a1, collagen type 1 a1; GAPDH, host keeping gene; Ocn, osteocalcin.
3.6. Biomechanical Evaluation
3.7. Statistical Analysis
4. Results
4.1. The Micro-CT Scan’s Results
; C, OVX-RI (risedronate treated ovariectomized rat); D, OVX-AL (alendronate treated ovariectomized rat); E, OVX-ZA (zoledronic acid treated ovariectomized rat), BMD: bone mineral density, BV/TV: bone volume/total volume, Ct/Th: cortical bone thickness, Tb.Th: trabecular bone thickness, *,**: indicates treatment group versus un-treatment OVX group, **P < 0.01, *P < 0.05.")
Micro CT analysis of different experimental groups 8 weeks after treatment, A, sham; B, OVX (PBS treated ovariectomized rat); C, OVX-RI (risedronate treated ovariectomized rat); D, OVX-AL (alendronate treated ovariectomized rat); E, OVX-ZA (zoledronic acid treated ovariectomized rat), BMD: bone mineral density, BV/TV: bone volume/total volume, Ct/Th: cortical bone thickness, Tb.Th: trabecular bone thickness, *,**: indicates treatment group versus un-treatment OVX group, **P < 0.01, *P < 0.05.
4.2. Blood and Serum Biochemical Parameters
| Factors | Sham | OVX | OVX-AL | OVX-RI | OVX-ZA |
|---|---|---|---|---|---|
| HCT, % | 48 ± 3 | 45 ± 2 | 44 ± 6 | 45 ± 8 | 45 ± 7 |
| TP, g/dL | 7.1 ± 0.2 | 6.8 ± 0.3 | 7.0 ± 0.5 | 6.7 ± 0.2 | 7.2 ± 0.8 |
| Ca, mg/dL | 9.4 ± 1.4 | 6.1 ± 1.3b | 8.7 ± 1.4 | 9.0 ± 1.8 | 9.2 ± 0.3 |
| P, mg/dL | 7.2 ± 0.3 | 6.6 ± 0.5 | 6.8 ± 0.4 | 6.8 ± 1.1 | 7.1 ± 0.4 |
| ALP, IU/L | 65.8 ± 3.8 | 135.5 ± 14.4c | 98.7 ± 9.6 | 82.3 ± 6.1 | 91.2 ± 5.2 |
| CTX, ng/mL | 34.5 ± 2.4 | 53.1 ± 4.7b | 38.1 ± 1.8 | 40.5 ± 3.5 | 36.3 ± 2.2 |
Abbreviations: OVX-AL, alendronate treated ovariectomized rat; OVX, PBS treated ovariectomized rat; OVX-RI, risedronate treated ovariectomized rat; OVX-ZA, zoledronic acid treated ovariectomized rat.
a Values are expressed as mean ± SD (n = 6), evaluated by Tukey's multiple comparison tests.
b P < 0.05 (treatments versus sham group).
c P < 0.01 (treatments versus sham group).
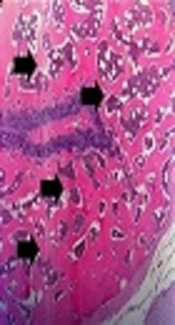
4.3. Histologic Findings

Histopathology section of vertebra, femur, and hip from different experimental groups after 8 weeks post-treatment. Asteroids: loss of interconnectivity, Arrows: trabeculae. OVX: PBS treated ovariectomized rat, OVX-RI: risedronate treated ovariectomized rat, OVX-AL: alendronate treated ovariectomized rat, OVX-ZA: zoledronic acid treated ovariectomized rat.
4.4. Q-RT PCR Analysis
 of hip, femoral head, and vertebra 8 weeks post-treatment; B, Effects of different treatments on mRNA expression of osteocalcin (OCN), alkaline phosphatase (ALP), and collagen type 1 (Col1) at 8 weeks post-treatment (vertebral bone). OVX: PBS treated ovariectomized rat, OVX-RI: risedronate treated ovariectomized rat, OVX-AL: alendronate treated ovariectomized rat, OVX-ZA: zoledronic acid treated ovariectomized rat, *,**: indicates treatment group versus un-treatment OVX group ,**P < 0.01, *P < 0.05.")
A, Histomorphometric analysis of all groups including trabecular bone (%) of hip, femoral head, and vertebra 8 weeks post-treatment; B, Effects of different treatments on mRNA expression of osteocalcin (OCN), alkaline phosphatase (ALP), and collagen type 1 (Col1) at 8 weeks post-treatment (vertebral bone). OVX: PBS treated ovariectomized rat, OVX-RI: risedronate treated ovariectomized rat, OVX-AL: alendronate treated ovariectomized rat, OVX-ZA: zoledronic acid treated ovariectomized rat, *,**: indicates treatment group versus un-treatment OVX group ,**P < 0.01, *P < 0.05.
4.5. Biomechanical Performance
| Value | Sham (1) | OVX (2) | OVX-AL (3) | OVX-RI (4) | OVX-ZA (5) |
|---|---|---|---|---|---|
| Femur | |||||
| Ultimate load, Nb | 44.1 ± 4.2 | 36.2 ± 6.5 | 40.2 ± 4.2 | 41.7 ± 5.7 | 43.2 ± 3.5 |
| Stiffness, N/mmc | 89.3 ± 6.4 | 78.5 ± 3.7 | 84.1 ± 5.1 | 86.9 ± 4.1 | 88.2 ± 2.2 |
| Vertebra | |||||
| Ultimate load, Nd | 125.4 ± 6.6 | 107.1 ± 4.5 | 117.8 ± 5.2 | 120.7 ± 3.2 | 123.6 ± 5.1 |
| Stiffness, N/mme | 1439.4 ± 28.5 | 1371.5 ± 33.7 | 1419.1 ± 24.3 | 1402.5 ± 34.9 | 1430.4 ± 25.2 |
Abbreviations: OVX-AL, alendronate treated ovariectomized rat; OVX, PBS treated ovariectomized rat; OVX-RI, risedronate treated ovariectomized rat; OVX-ZA, zoledronic acid treated ovariectomized rat.
a Values are expressed as median ± SD.
b P < 0.05 (2 vs. 1, 3, 4 and 5).
c P < 0.05 (2 vs. 1, 3, 4 and 5).
d P < 0.05 (2 vs. 1, 4 and 5).
e P < 0.05 (2 vs. 1, 5), (4 vs. 1, 5).