








1. Background
Since 2019, the spread of COVID-19 with new manifestations in children and adults has caused significant concern worldwide. Among the strains created by this virus, signs and symptoms of the alpha, beta, delta, and omicron strains were more noticeable in Iranian children. The omicron strain of the SARS-CoV-2 virus was reported almost two years after the start of the pandemic, when the number of delta strain infections was decreasing, causing more concern for parents due to its high prevalence in children. Among the types of corona strains, the alpha B.1.1.7 strain was first identified in England in November 2020. This strain was more transmissible, with a higher lethality than the original virus. The beta strain B.1.351 was identified in South Africa at the end of 2020 and was released to other countries. This strain had a transmission rate 50% higher than the original strain and a higher probability of hospital mortality. The delta strain is B.1.617.2, first identified in India at the end of 2020 and was the dominant strain until omicron. This strain was seen to be twice as infectious as compared to the previous strains. The omicron BA.1 strain was first seen in Botswana, South Africa, at the end of November 2021. By December of that year, the number of cases had dramatically increased, with BA.5 accounting for more than 50% of cases in the United States and BA.4 accounting for 17% of cases (1). According to World Health Organization (WHO) statistics, omicron caused five to six times more infections in children than in previous waves of COVID-19 due to its increased affinity to host cell receptors and ability to escape the immune system caused by previous infection or vaccination (2). The omicron strain is more capable of penetrating the immune system of previously infected people than the alpha, beta, and delta strains, and both vaccinated and previously infected people are at risk (3). The most common manifestations of the new strain are fever, cough, shortness of breath, seizures, vomiting, and diarrhea (4). In an article by Christophers et al., fever was the most common symptom among all strains, followed by cough, diarrhea, and vomiting. Among the less common symptoms were headache, seizures, skin manifestations, rash, and Kawasaki-like symptoms (5). Hospitalized patients were often confined to the emergency department, and a few cases required oxygen therapy and mechanical ventilation, with mortality statistics reported to a limited extent (4). However, Butt et al. (6) showed that serious complications of the disease may occur in children, especially those with underlying diseases and chronic conditions. Rarely, hyperinflammatory syndrome with multisystem involvement multisystem inflammatory syndrome in children (MIS-C) has been reported, associated with high hospitalization rates and the need for increased support. In addition to the clinical symptoms of the coronavirus strains, specific laboratory manifestations have been identified for each strain. The most practical laboratory tests reported in COVID-19 include white blood cell count, platelet count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), creatinine, urea, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) (5). It is crucial to understand the clinical and laboratory symptoms of each strain for vaccine prevention and treatment. Multiple vaccines for SARS-CoV-2 have been provided for use in children aged five years and older and have been effective in preventing infection, hospitalization in the pediatric intensive care unit, need for mechanical ventilation, and death (6). In a study by Vitiello et al., it was reported that two doses of the vaccine offer little or no protection against omicron, while booster doses provide significant protection against mild disease and possibly higher levels of protection against severe disease (7). To minimize the disease burden in children, it is necessary to observe hygiene, vaccination, isolation, and preventive actions such as wearing masks, practicing hand hygiene, cleaning, and ventilating indoor spaces (2).
2. Objectives
The study focused more on the clinical manifestations and symptoms, such as fever, abdominal pain, seizure/febrile convulsion, pneumonia, gastroenteritis, cough, urinary tract infection, a MIS-C, skin presentation, croup, and hyperglycemia. Understanding common symptoms in the alpha, beta, delta, and omicron strains is a step toward predicting subsequent symptoms and the severity of the disease in children, enabling prompt treatment.
3. Methods
This cross-sectional study compares clinical manifestations of different COVID-19 strains (alpha, beta, delta, and omicron) based on their prevalence peaks. The study assumed peak time to be equal to the highest rate of each strain, corresponding to the WHO peak of variants of concerns (VOCs). Patients were included if they were referred to the emergency department of Mofid Children's Hospital in Tehran during the peak of the alpha strain in November 2020, the beta strain in April 2021, the delta strain in August 2021, and the omicron strain in February 2022, and had positive nasopharyngeal PCR. Peak strains were obtained based on the WHO statistics, and the nasopharyngeal PCR test was performed by expert laboratory personnel. Patients with mild disease, outpatient treatment, immunodeficiency, and underlying disease were excluded from the study. Hyperglycemia was defined as blood glucose levels greater than 125 mg/dL while fasting and greater than 180 mg/dL 2 hours postprandial (8). Recording of the patients' clinical manifestation and laboratory findings was done confidentially and with their permission.
We selected variables that were most likely to differ among COVID-19 strains, and after collecting data, the information was analyzed using SPSS software. The relationship between quantitative and qualitative variables with the type of COVID-19 strain was assessed through the chi-square test. We also used multivariate regression tests in this study. Various national VOC peaks were considered as dependent variables, and the lab tests were selected as the independent variables. However, the resulting model was insignificant for each type of COVID-19 (P-value > 0.05). Therefore, only the P-values in the coefficient table were reported (see Table 1 for details). ANOVA and Wilcoxon's tests were used to measure differences in all types of COVID-19 strains together and separately between two strains, respectively. We considered a significant difference with a P-value of less than 5%.
| Laboratory Test | Coronavirus Type | Confidence Interval 95 % | ||||
|---|---|---|---|---|---|---|
| Delta | Omicron | Alpha | Beta | Lower Bound | Upper Bound | |
| WBC | < 0.001 | 0.221 | 0.013 | 0.541 | 0.000 | 0.000 |
| Lymphocyte percentage | < 0.001 | < 0.001 | 0.002 | 0.009 | -0.019 | -0.011 |
| CRP | < 0.001 | 0.001 | 0.034 | 0.636 | -0.001 | -0.142 |
| ESR | < 0.001 | 0.01 | 0.017 | 0.428 | -0.013 | -0.003 |
The Relationship Between Laboratory Investigations and SARS-CoV-2 Strains in Children Referred to the Pediatric Emergency Department a
4. Results
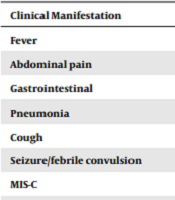
In this study, we compared the clinical and laboratory manifestations of four strains of COVID-19: Alpha, beta, delta, and omicron. A total of 649 patients were included in the survey, with 58.1% being male. The mean age of the included patients was 2.01 ± 3.0 years, ranging from 0.08 to 14 years. The distribution of the number of patients suffering from each of the four COVID-19 strains was not statistically significant. The most frequent clinical manifestation was fever, while skin presentation was the least frequent. Table 2 shows the frequency and percentage of each clinical manifestation.
| Clinical Manifestation | Frequency (%) |
|---|---|
| Fever | 196 (30.2) |
| Abdominal pain | 28 (4.3) |
| Gastrointestinal | 136 (21) |
| Pneumonia | 30 (4.6) |
| Cough | 83 (12.8) |
| Seizure/febrile convulsion | 78 (12) |
| MIS-C | 22 (3.4) |
| Skin presentations | 12 (2) |
| Croup | 30 (4.8) |
| Hyperglycemia | 20 (3.1) |
Frequency of Clinical Manifestations of COVID-19 During National Peaks of Alpha, Beta, Delta, and Omicron in Children Referred to the Pediatric Emergency Department
Table 2 illustrates the frequency of clinical manifestations of patients suffering from all four kinds of COVID-19.
The white blood cell counts (WBC) ranged from 1200 to 24700 with a mean of 8423.9 ± 5427.3. The mean values of CRP and ESR were 30.14 ± 20.07 and 38 ± 22.6, respectively. Mildly elevated CRP levels were observed in more than half of the patients, while ESR levels were significantly increased in all patients. Further details of the laboratory investigations are presented in Table 3.
| Laboratory Investigation | Percentage |
|---|---|
| Low WBC (< 4000/mm3) | 40.8 |
| Normal levels of WBC (4000 - 10000/mm3) | 44 |
| Elevated levels of WBC (> 10000/mm3) | 14.3 |
| Normal CRP (< 10 mg/L) | 8.9 |
| Mildly elevated CRP (10 - 40 mg/L) | 60.7 |
| Moderately elevated CRP (40 - 70 mg/L) | 25.9 |
| Severely elevated CRP (> 70 mg/L) | 4.5 |
| Normal levels of ESR (< 6 mm/hr) | 3.1 |
| Elevated levels of ESR (> 6 mm/hr) | 96.9 |
Frequency of Laboratory Findings in Children with Alpha, Beta, Delta, and Omicron COVID-19 Strains Referred to the Pediatric Emergency Department
Table 3 demonstrates the results of laboratory investigations.
No significant relationship was found between COVID-19 virus type, age, and gender. We performed a chi-square test to assess the correlation between clinical manifestations, laboratory studies, and the four types of coronavirus, including delta, omicron, alpha, and beta. The results indicated that gastroenteritis, urinary tract infection, and croup had a significantly positive correlation with delta, beta, and omicron subtypes (P-value < 0.003, < 0.001, and < 0.001, respectively). Cough was more frequent in patients infected with alpha and beta subtypes. Fever, croup, cough, and gastroenteritis were negatively related to beta, delta, omicron, and alpha subtypes (P-value < 0.001 and 0.001, respectively). Hyperglycemia was more commonly observed in patients infected with Beta subtypes. The P-values of the chi-square test are shown in Table 4.
| Clinical Manifestation | Delta | Omicron | Alpha | Beta |
|---|---|---|---|---|
| Fever | 0.1 | 0.093 | 0.095 | < 0.001 |
| Abdominal pain | 0.402 | 0.575 | 0.864 | 0.83 |
| Gasteroenteritis | 0.003 | 0.343 | 0.014 | 0.13 |
| Pneumonia | 0.770 | 0.134 | 0.788 | 0.098 |
| Cough | 0.096 | < 0.001 | < 0.001 | 0.007 |
| Seizure/febrile convulsion | 0.358 | 0.315 | 0.559 | 0.564 |
| MIS-C | 0.718 | 0.93 | 0.667 | 0.056 |
| Skin presentation | 0.718 | 0.587 | 0.309 | 0.974 |
| Croup | 0.001 | < 0.001 | 0.044 | 0.949 |
| Hyperglycemia | 0.141 | 0.142 | 0.513 | 0.007 |
Significance of Clinical Symptoms During Alpha, Beta, Delta, and Omicron Peaks in Children Referred to the Pediatric Emergency Department
Table 4 shows the resulting P-value after conducting the chi-square test.
A multivariate regression test was performed to investigate the relationship between laboratory tests and SARS-CoV-2 strains. The WBC count was significantly elevated in patients infected with the delta strain. The percentage of lymphocytes was increased in patients with delta, omicron, and alpha strains. C-reactive protein and ESR levels were significantly increased in patients with delta infection. In patients with omicron infection, CRP levels were significantly elevated. Details of the multivariate regression test are presented in Table 1.
An ANOVA regression test was performed to compare the means of variables across the different SARS-CoV-2 strains. The mean age of patients was significantly higher in those infected with the beta subtype. Patients with the beta subtype experienced fever less frequently than those infected with the other three subtypes, as shown by the chi-square test. Gastroenteritis was significantly more common in patients with the delta subtype. Cough was more common among patients infected with the alpha subtype, and the croup rate was significantly higher than the other subtypes. The chi-square test shows that more patients with the beta subtype manifested hyperglycemia. The details of the ANOVA test are listed in Table 5.
| Clinical Manifestation | P-Value |
|---|---|
| Fever | < 0.001 |
| Abdominal pain | 0.865 |
| Gasteroenteritis | < 0.001 |
| Pneumonia | 0.262 |
| Cough | < 0.001 |
| Seizure/febrile convulsion | 0.614 |
| MIS-C | 0.169 |
| Skin presentation | 0.738 |
| Croup | < 0.001 |
| Hyperglycemia | 0.036 |
P-Values Resulting from ANOVA Regression Test Comparing Averages of Variables Among Patients with Alpha-Peak, Beta-Peak, Delta-Peak, and Omicron-Peak
Table 5 summarizes the resulting P-value of the ANOVA test.
Among the assessed laboratory investigations, the percentage of lymphocytes was higher in patients who suffered from omicron and delta subtypes (P-value < 0.001). C-reactive protein and ESR levels were significantly higher in patients with the delta subtype (P-value < 0.001 and < 0.001, respectively).
5. Discussion
The predominant variant of COVID-19 in Iran was the alpha strain in November 2020, which was replaced by the beta strain in April 2021. In August 2022, the delta strain became prevalent, followed by the omicron strain in February 2022. The prevalence of the gamma strain in Iranian children was insignificant, as shown by the curve of COVID-19 strain peaks presented by the WHO. This study examined the clinical and laboratory symptoms of different COVID-19 strains in children. However, the effect of the vaccine could not be assessed, as the investigation was limited to hospitalized patients, and those with mild disease and outpatients were not included. With the global spread of the COVID-19 pandemic, symptoms such as fever, cough, myalgia, and fatigue, along with laboratory findings of leukocyte count abnormalities and chest radiography evidence, have been reported as non-specific symptoms in various strains. Previous studies have shown that fever is commonly present but cannot be considered the main symptom. The present study confirms these findings. Fever remains the most common symptom across all types of COVID-19 strains, although our results indicate that children with the Beta subtype experience less fever. Other manifestations, such as diarrhea, vomiting, abdominal pain, and dizziness, were less common, but as our study shows, they may sometimes be the only symptoms (9). The symptoms are often mild and improve within two weeks (10). In comparison to adults, children have a lower presence of comorbidities such as diabetes, vascular disease, and hypertension, and the risk of contracting the disease in children has been reported to be through close contact with infected people or travel to endemic areas (11). However, due to the absence of these factors in children, the severity of the disease is expected to be lower in them. Recent studies have shown that in children, the most common consequence of COVID-19 is a period without symptoms or mild symptoms. Additionally, at the time of infection in children, compared to adults, they have stronger and more stable antibodies in their bodies for up to 17 months after infection. It was found that after infection, compared to adults, antibody binding to alpha, beta, and delta strains is stronger in children, but neutralization is similar (12). Multisystem inflammatory syndrome in children is a severe disease that has been reported in immunocompromised individuals. In this study, MIS-C accounted for 3.4% of all COVID-19 strains, higher than the percentage of urinary tract infections, skin manifestations, and hyperglycemia. Among the laboratory symptoms, decreased or normal lymphocyte count, as well as normal or high levels of CRP, procalcitonin, liver and muscle enzymes, myoglobin, and D-dimer, were reported as manifestations of COVID-19. Decreased lymphocyte count and high CPK, procalcitonin, and D-dimer levels were found to be differentiating factors between severe and mild cases (11). In this study, only WBC, lymphocyte count, ESR, and CRP were evaluated among the mentioned items, as other diagnostic tests were not performed for all hospitalized patients except in cases of suspected severe disease and MIS-C. The increase in lymphocytes in hospitalized patients with the alpha, delta, and omicron strains compared to other strains is interesting. Previous studies have shown that lymphopenia is a serious factor in the severity of the disease and mortality (13). With less lymphopenia in patients with omicron, the severity of the disease was also less in this strain. In this study, most patients had mildly elevated CRP, high ESR, and normal WBC (leukocytosis was often reported in the delta strain). Regarding age, studies have shown that children under one year old with underlying diseases are more at risk of serious COVID-19, while people under 18 are less likely to be affected by this disease. It can be concluded that the maturity and function of ACE2 as a coronavirus receptor is less in children than in adults. Additionally, immunity to other viruses protects the body against coronavirus (9). In a study, the BCG vaccine was considered important in strengthening the immune system for memory cells (14, 15). Increasing age is independently related to the severity of COVID-19 disease (16). In our study, with an average age of two years, there was no correlation between age and gender in different strains. However, overall, the beta subgroup had a higher average age, and there was no increase in age-related disease severity among the strains. In the United States, omicron was significantly milder but more pathogenic. On the other hand, the number of outpatient visits was reported to be higher, and hospitalization cases also increased (10). According to the WHO statistics in Iran, the omicron strain was responsible for the second-highest number of infections after delta. One limitation of our study was the lack of a separate subgroup for vaccinated or previously infected patients, which would have allowed us to evaluate the effect of antibodies and vaccines on patients. As we did not have access to laboratory kits for PCR-based determination of COVID-19 strains, we used WHO statistics to identify the strains based on disease prevalence, which is another limitation. It was also impossible to determine whether leukocytosis or elevated CRP levels were strain-specific or disease-specific, although negative cultures provided some assistance. After vaccination was administered to adolescents, the age of those infected during the Delta and Omicron periods changed to a younger population (16).
5.1. Conclusions
The clinical symptoms of COVID-19 in children vary depending on the strain of the virus, corresponding to the WHO peak of VOCs. This variability can help diagnose the disease.
