

1. Background
Lactation is widely recognized as an effective strategy for promoting good health and preventing diseases, particularly infections, making it highly recommended, especially in developing and less-developed countries (1). However, many women face challenges when it comes to breastfeeding, even under normal circumstances, without the added stress of natural disasters. These challenges were further exacerbated during the initial phase of the COVID-19 pandemic, as sufficient information was not readily available (2). Subsequently, the World Health Organization declared breastfeeding by mothers with COVID-19 safe during the pandemic and encouraged its continuation (3).
Once the vaccine became available, it was recommended for all individuals, including lactating women (4). Despite these recommendations, the coverage of COVID-19 vaccination among lactating mothers was insufficient (5). According to reports from the World Health Organization, as of February 18, 2023, approximately 155 million vaccine doses had been administered in Iran, with 65 million individuals receiving their first dose and 42,976,431 individuals receiving their third dose. However, there is currently no available data regarding the proportion of vaccinated lactating women (6). The reasons for differences in vaccine uptake or refusal vary. The lack of advice from authorities has been documented as one of the main reasons why breastfeeding women refrain from vaccination (7). Fear of safety concerns and associated risks while breastfeeding is another significant factor contributing to low vaccine compliance (8). One study found that fear of contracting COVID-19 can actually lead to a positive attitude towards vaccination and increase the likelihood of receiving the vaccine (9). Additionally, breastfeeding women may be more likely to get vaccinated due to increased perceived threats compared to pregnant women (10). However, a study conducted in Singapore revealed that 62.3% of lactating women were undecided about vaccination, while 20.8% were reluctant (11).
Various factors can influence vaccine compliance or hesitancy. Several studies have shown that receiving other vaccines, such as the influenza vaccine, before or during lactation can play a role in determining COVID-19 vaccination during this period (12-17). A history of previous lactation can also impact an individual’s decision to comply with or refrain from vaccination (18, 19). Furthermore, the viewpoints of family and friends on vaccination can be influential (20). The number of children and lack of health insurance have also been identified as factors influencing vaccine uptake (21, 22).
Breastfeeding self-efficacy appears to be a crucial factor in determining whether an individual chooses to receive a vaccination or is hesitant about it. Emotional and psychological factors have a significant impact on breastfeeding self-efficacy (23), and this relationship is evident in our society, as well as in other countries (20, 24). Given the varying reasons why mothers either choose to get vaccinated or hesitate, it is essential to compare the compliance and hesitancy rates among breastfeeding women.
2. Objectives
The main objective of this study was to compare two groups of breastfeeding women-those who received the COVID-19 vaccine and those who refused vaccines-in terms of their demographic factors, fear of COVID-19, and breastfeeding self-efficacy.
3. Methods
3.1. Study and Design
This is a comparative cross-sectional study. The sampling was conducted from February to April 2022 to compare factors that may be associated with receiving COVID-19 vaccination in lactating women.
A multi-stage random sampling was employed in this study. The northwest and western regions of Tehran are covered by comprehensive health centers affiliated with the Iran University of Medical Sciences. These regions are situated within the seven municipal districts of Tehran, including 9, 18, 21, 22, 2, 5, and 6. Overall, 18 centers are in the northwest, and 18 centers are in the west. Thus, a total of 36 centers were identified as clusters. First, using a simple random, 18 centers or clusters were selected for inclusion in the study. Twenty-five individuals from each center were entered into the study. The individuals were the same in terms of social and economic status in the clusters. Subsequently, a comprehensive list of breastfeeding women was extracted. Then, they were invited to centers for infant and mothers’ postnatal care. They were visited, and if they were eligible, they filled out a consent form, followed by the scales of study. Vaccinated breastfeeding women comprised one group, and unvaccinated breastfeeding women were placed in the other group.
3.2. Participants
The study included a total of 450 participants who were divided into two groups: One group who received the COVID-19 vaccine (n = 225) and the other group who did not receive the vaccine (n = 225). The inclusion criteria were as follows: Being 18 - 49 years old, having an infant under six months of age, having a healthy newborn, having a single pregnancy, and having no contraindications to breastfeeding. All of this information is obtained in an electronic integrated system. Mothers’, their husbands’, and babies’ ages were based on their ID cards. Infants’ health status was based on their vaccination and growth cards filled out by care providers. In both groups, information related to receiving the COVID-19 vaccine was gathered from electronic records or mothers’ vaccination cards if they had received two doses of the COVID-19 vaccine during the third trimester of pregnancy or lactating.
3.3. Sample Size
The sample size necessary for comparing COVID-19 vaccination in lactating women was determined by considering demographic variables, breastfeeding, and fear of COVID-19. With due attention to the questions related to breastfeeding, a self-efficacy score was used, with a standard deviation of 7.6, taken from Moafi et al. (25) to ensure a precision of two in a 95% confidence interval and 80% test power. The sample size was calculated based on two equal groups of women, resulting in a sample size of 225 participants for each group.
3.4. Study Variables
Outcome/Dependent variable: The outcome variable of the study was receiving the COVID-19 vaccine and not receiving the COVID-19 vaccine. Independent variables were demographic factors, breastfeeding self-efficacy, and fear of COVID-19. The scales used for this study consisted of the following:
3.4.1. Demographic Data
The demographic data checklist included 13 questions regarding the mother’s age, infant’s age, number of children, education level of the mother and her husband, occupation, economic household levels, type of delivery, type of newborn nutrition, history of COVID-19 infection diagnosed by a physician or laboratory, breastfeeding self-efficacy, and fear of COVID-19.
3.4.2. Dennis’ Breastfeeding Self-efficacy Scale (Short Form)
Dennis’ Breastfeeding Self-Efficacy Scale assesses the confidence of mothers in breastfeeding their infants. This scale was revised in 2003 by Dennis and condensed to 14 questions. Scoring is conducted on a five-point Likert scale, ranging from “not at all confident” (score 1) to “completely confident” (score 5). The total scores range from 14 to 70, with higher scores indicating greater levels of self-efficacy. The reliability of this instrument was confirmed by Dennis, yielding a Cronbach’s alpha of 0.9725 (26). The Persian version of the scale has been translated, and its reliability was confirmed with a Cronbach’s alpha of 0.9126 (27). In this study, reliability was calculated as internal consistency among 30 breastfeeding women, giving Cronbach’s alpha of 0.90. Ten experts also assessed content validity.
3.4.3. COVID-19 Fear Questionnaire
The COVID-19 Fear Questionnaire, developed by Ahorsu et al. in 2020, consists of seven questions and utilizes a five-point Likert scale ranging from “strongly disagree” (score 1) to “strongly agree” (score 5). The total score ranges from 5 to 35, with higher scores indicating a greater intensity of fear. Ahorsu et al. confirmed the reliability of this Persian questionnaire by calculating a Cronbach coefficient of 0.82 (28). Internal consistency was measured among 30 breastfeeding women, giving Cronbach’s alpha of 0.84.
3.5. Ethics Approval
The study received approval from the Ethics Committee of Iran University of Medical Sciences, Tehran, Iran, under the ethics code IR.IUMS.REC.1400.971. Before data collection, a sampling license was obtained from the Iran University of Medical Sciences. All participants were provided with a written informed consent form to sign. The participants were assured that their information would be kept confidential, and all necessary research permissions were obtained. Lactating women completed demographic information, breastfeeding self-efficacy, and COVID-19 fear forms.
3.6. Statistical Analysis
The collected data was analyzed using SPSS version 16. Descriptive statistics, such as the mean, standard deviation, frequency, and percentage, were used to report numerical indices. In inferential statistics, variables related to socioeconomic characteristics and health status are compared. Categorized qualitative variables were analyzed in two groups using the Chi-square test, while independent t-tests were used for quantitative variables. Moreover, in order to assess confounding factors such as socioeconomic variables, fear, and health conditions, the Logistic Regression test was used to determine the factors affecting vaccination status among lactating women. The dependent variable was whether the women were vaccinated or unvaccinated, while the independent variables included fear of COVID-19, breastfeeding self-efficacy, demographic characteristics, and health status. The variables with a significance level less than 0.2 were included in the model. The statistical tests were performed at the 95% confidence interval. In the world, P-value < 0.05 was considered significant.
4. Results
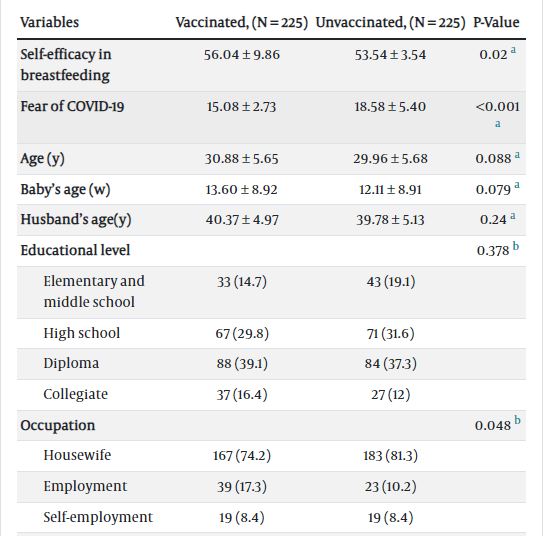
In total, 450 breastfeeding women were eligible to participate in this study. Based on whether to get the vaccine or not, 225 women were in the vaccinated group and 225 women in the unvaccinated group. This study aimed to compare the received COVID-19 vaccine among breastfeeding women, controlling for variables such as COVID-19 fear, breastfeeding self-efficacy, and demographic characteristics. The findings revealed an average age of 30.88 ± 5.65 years in the vaccinated group and 29.96 ± 5.6 years in the unvaccinated group. Besides, 74.2% of the vaccinated and 81.3% of the unvaccinated women were housewives. Approximately 48% of the vaccinated women and 50.7% of the unvaccinated women had one child. The majority of women had diploma degrees or above. Cesarean section was the most common childbirth method, with 69.3% of the vaccinated women and 62.2% of the unvaccinated women opting for it. The baby’s age was 13.60 ± 8.92 weeks in the vaccinated women and 12.11 ± 8.91 weeks in the unvaccinated women. The mean husband’s age was 40.37 ± 4.97 in the vaccinated and 39.78 ± 5.13 in the unvaccinated women. There were no differences in mothers’ age, educational level, baby’s age, childbirth type, husbands’ occupation, and husband’s age between the two groups. Among vaccinated individuals, 47.6% of husbands held academic degrees, while for unvaccinated individuals, the percentage was 37.8%. The mean score of breastfeeding self-efficacy was 56.04 ± 9.86 in the vaccinated group, whereas it was 53.54 ± 3.54 in the unvaccinated group. The mean score of COVID-19 fear was 15.08 ± 2.73 in the vaccinated group and 18.58 ± 5.40 in the unvaccinated group. Concerning the type of baby feeding, 60.9% of the vaccinated individuals and 68.9% of the unvaccinated individuals used exclusive breastfeeding. There was a significant difference in husbands’ education levels between the two groups (P = 0.03). Through independent sample t-test analysis, it was determined that vaccinated women exhibited significantly higher levels of breastfeeding self-efficacy than unvaccinated women (P = 0.02). The vaccinated group displayed significantly lower levels of COVID-19 fear than the unvaccinated group (P < 0.001). There was a significant difference in child number and type of baby feeding between the two groups (P = 0.04). Data are shown in Table 1.
| Variables | Vaccinated, (N = 225) | Unvaccinated, (N = 225) | P-Value |
|---|---|---|---|
| Self-efficacy in breastfeeding | 56.04 ± 9.86 | 53.54 ± 3.54 | 0.02 a |
| Fear of COVID-19 | 15.08 ± 2.73 | 18.58 ± 5.40 | <0.001 a |
| Age (y) | 30.88 ± 5.65 | 29.96 ± 5.68 | 0.088 a |
| Baby’s age (w) | 13.60 ± 8.92 | 12.11 ± 8.91 | 0.079 a |
| Husband’s age(y) | 40.37 ± 4.97 | 39.78 ± 5.13 | 0.24 a |
| Educational level | 0.378 b | ||
| Elementary and middle school | 33 (14.7) | 43 (19.1) | |
| High school | 67 (29.8) | 71 (31.6) | |
| Diploma | 88 (39.1) | 84 (37.3) | |
| Collegiate | 37 (16.4) | 27 (12) | |
| Occupation | 0.048 b | ||
| Housewife | 167 (74.2) | 183 (81.3) | |
| Employment | 39 (17.3) | 23 (10.2) | |
| Self-employment | 19 (8.4) | 19 (8.4) | |
| Husband’s Educational level | 0.03 b | ||
| Elementary school | 20 (8.8) | 26 (11.5) | |
| High school | 21 (9.3) | 30 (13.3) | |
| Diploma | 77 (34.2) | 84 (37.3) | |
| Collegiate | 107 (47.5) | 85 (37.8) | |
| Husband’s Occupation | 0.57 b | ||
| Employment | 72 (32) | 64 (28.4) | |
| Self-employment | 141 (62.7) | 145 (64.4) | |
| Unemployed | 12 (5.3) | 16 (7.1) | |
| Child number | 0.04 b | ||
| One | 108 (48) | 114 (50.7) | |
| Two | 86 (38.2) | 92 (40.9) | |
| Three | 26 (11.6) | 15 (6.7) | |
| Four or more | 5 (2.2) | 4 (1.8) | |
| Household economic level | 0.17 b | ||
| Undesirable | 9 (4) | 16 (7.1) | |
| Relatively favorable | 156 (69.3) | 140 (62.2) | |
| Favorable | 60 (26.7) | 69 (30.7) | |
| Childbirth type | 0.76 a | ||
| Cesarean section | 152 (67.6) | 155 (68.9) | |
| Vaginal | 73 (32.4) | 70 (31.1) | |
| Type of baby feeding | 0.04 b | ||
| Exclusive breastfeeding | 137 (60.9) | 157 (69.8) | |
| Breastfeeding and formula | 72 (32) | 59 (26.2) | |
| Breastfeeding and family diet | 16 (7.1) | 9 (4) | |
| History of COVID-19 | 0.20 b | ||
| Yes (during pregnancy) | 39 (17.3) | 32 (14.2) | |
| Yes (during breastfeeding) | 30 (13.3) | 22 (9.8) | |
| Yes (before pregnancy) | 31 (13.8) | 24 (10.7) | |
| No | 125 (55.6) | 147 (65.3) |
Demographic Characteristics of Vaccinated and Unvaccinated Lactating Women
The final analysis was performed on the data of 450 individuals. The variables that had a significance level of lower than 0.2 were entered into the model. Logistic regression showed that individuals’ age, baby’s age, woman’s occupation, husband’s education level, type of baby feeding, child number, fear of COVID-19, and breastfeeding self-efficacy were independent variables for predicting received COVID-19 vaccination. Receiving or not receiving vaccination was a dependent variable. The odd ratio was the proportion receiving the vaccine was assigned a cod of 1, and to not receive the vaccine were assigned a code of 0. The study findings indicated that husbands with a higher level of education (OR = 0.44 95% CI: 0.19-0.76, P = 0.04), a greater number of children (OR = 0.56, CI: 0.31-0.89, P = 0.04), and a lower level of fear regarding COVID-19 (OR = 0.90, CI: 0.87-0.94, P<0.001) had higher odds of receiving vaccine than others. In other words, the odd of receiving a vaccine were 56% higher in breastfeeding women whose husbands held academic degrees than in others. The odds of receiving the vaccine were 44% higher in women who had 4 children and above than others, and the odds of receiving the vaccine were higher in women who had a 10% lower level of fear regarding COVID-19. So, the type of baby feeding, women’s education level, women’s and their husbands’ occupation, and breastfeeding self-efficacy did not predict receiving vaccination. Data are shown in Table 2.
| Variables | B | Sig. | OR | Unadjusted Odds (95% CI) | Adjusted Odds (95% CI) |
|---|---|---|---|---|---|
| Women’s age (y) | 0.007 | 0.76 | 1.007 | 1.98 (.951-2.003) | 1.007 (.965-1.050) |
| Baby’s age (w) | 0.010 | 0.65 | 2.20 | 1.43 (.854-1.53) | 1.006 (.982-1.030) |
| Fear of COVID-19 a | - 0.97 | 0.000 | 0.908 | 0.991 (.853-.957) | 902 b (.872-.945) |
| Breastfeeding self-efficacy | 0.020 | 0.126 | 1.021 | 1.51 (.984-1.73) | 1.021 (.994-1.048) |
| Occupation | |||||
| Housewife | Reference category | ||||
| Employment | 0.20 | 0.58 | 1.22 | 1.94 (0.678 - 2.96) | 1.22 (0.594 - 2.51) |
| Self-employment | 0.66 | 0.15 | 1.94 | 1.44 (0.567 - 1.26) | 1.03 (0.599 - 1.98) |
| Husband’s education level a | |||||
| Elementary school | Reference category | ||||
| High school | - 0.61 | 0.08 | 0.540 | 0.632 (0.265 - 754) | 0.540 (0.271 - 1.079) |
| Diploma | - 0.54 | 0.11 | 0.580 | 0.704 (0.302 - 732) | 0.580 (0.293 - 1.150) |
| Collegiate | - 0.82 | 0.40 | 0.438 | 0.499 (0.254 - 0.897) | 0.438 b (0.196 - 0.677) |
| Type of baby feeding | |||||
| Exclusive breastfeeding | Reference category | ||||
| Bottle milk | - 0.37 | 0.42 | 0.686 | 0.806 (0.353 - 1.543) | 0.686 (0.265 - 1.773) |
| Breastfeeding and family diet | 0.12 | 0.81 | 1.130 | 2.004 (0.423 - .3.016) | 1.130 (0.410 - 3.112) |
| Child number a | |||||
| One | Reference category | ||||
| Two | 0.19 | 0.56 | 1.21 | 0.988 (0.908 - 1.967) | 1.21 (0.624 - 2.38) |
| Three | 0.07 | 0.89 | 1.042 | 1.34 (1.12 - 1.45) | 1.042 (1.035 - 1.167) |
| Four | - 0.57 | 0.04 | 0.563 | 0.584 (0.399 - 0.998) | 0.563 b (0.318 - 0.897) |
Results of Logistic Regression Analysis: Unadjusted and Adjusted Odds Ratios of Breastfeeding Women (N = 450)
5. Discussion
The present study aimed to compare demographic characteristics, fear of COVID-19, and self-efficacy in breastfeeding between two groups of lactating women based on their acceptance or refusal of COVID-19 vaccination. The results showed no differences between breastfeeding women’s age, childbirth type, history of COVID-19 infection, household economic level, education level, and husbands’ occupation between the two groups. However, a study indicated that young pregnant women were less likely to receive the COVID-19 vaccine (29, 30). Furthermore, a systematic review demonstrated that older pregnant women reported less anxiety than younger ones. Younger women refused to get the vaccine (31). This finding is reasonable because it is recognized that pregnancy in older mothers is a risk factor for unfavorable outcomes, and there are complications for the mother and baby (32). Additionally, older age was associated with higher COVID-19 mortality (33). In the present study, the number was significantly different between the two groups. Interestingly, the present study found that lactating women with more children were more likely to be vaccinated, which aligns with the results of a study suggesting that parents with school-aged children were more worried about the transmission of the infection to their families (34).
In the current study, the education level of lactating women was not different between the two groups. However, another study indicated that women with lower education levels were more hesitant to receive the vaccine (35). Nonetheless, in our study, breastfeeding women’s husbands’ education levels were significantly different between the two groups. Women whose husbands held academic degrees were more motivated to receive the COVID-19 vaccine. Education level probably has a relationship to economic status; in this regard, a study demonstrated that pregnant women from poor socioeconomic backgrounds were less likely to receive a vaccine (36). Moreover, women with lower socioeconomic tended to be more afraid of the disease and to receive the COVID-19 vaccine (37). Moreover, research indicates that pregnant women with lower education levels, unemployment, and unfavorable socioeconomic conditions have reported increased levels of fear and concern during the pandemic (38). in this study, the history of COVID-19 infection was not different between the two groups. This finding is consistent with another study that showed no association between a history of COVID-19 infection and vaccine uptake (39).
The present study showed that women who had higher levels of fear of COVID-19 infection were less interested in receiving the vaccine, whereas lactating women who had received the vaccine exhibited less fear of the disease. In this regard, a previous study interestingly found that fear of COVID-19 during pregnancy was a predictor of COVID-19 vaccination uptake, while fears about the safety and side effects of COVID-19 vaccines were reasons for declining vaccination (40). In this respect, a study also showed that pregnant women who trusted in COVID-19 vaccines and the effectiveness of the vaccine for the mother and fetus received the vaccine while worrying about the safety of COVID-19 vaccines, concerned about side effects of vaccines for mothers and their fetus, and diagnosis of COVID-19 infection during pregnancy were reasons for decreasing vaccination (17). Additionally, a study conducted on the general population demonstrated that fear of COVID-19 was a very stable predictor for vaccination willingness, but researchers concluded that there are several probable approaches to decrease vaccination desire. One of them could be the use of threatening messages by social media. They found that the perceived ability of a person to deal with a threat could avoid a threat, especially when this ability is high; sometimes fear can help motivate getting vaccinated; otherwise, it can result in defensive responses (41). Another approach identified as the strong predictor for vaccine acceptance is confidence in public health science and health agencies, compliance with protocols on the condition that they were not changed frequently, and attitudes toward other routinely administered vaccines (41). Therefore, it is evident that COVID-19 vaccine acceptance and its predictors among women vary across different countries and regions worldwide (15).
In the present study, it was found that breastfeeding self-efficacy was higher in women who received the COVID-19 vaccine than in those who refused vaccination. However, there was no significant difference in breastfeeding self-efficacy between vaccinated and unvaccinated women. Therefore, we concluded that breastfeeding self-efficacy is not a predictor of COVID-19 vaccine acceptance. Other studies have also shown that women who have the confidence and capability to breastfeed are more likely to breastfeed frequently and exclusively (32, 33). This finding is consistent with the fact that even during the COVID-19 pandemic, women continued to breastfeed their infants. Overall, the results highlight the importance of supporting women in their breastfeeding journey, regardless of the pandemic situation. Women who feel confident and capable of breastfeeding are more likely to succeed, both in the pre-pandemic period and during the pandemic (42).
Other things that may influence the decision to receive the vaccine are social media (43, 44), confidence in the policymakers (45), and trust in the pharmaceutical industry, experts, and healthcare providers (46). These have all shown significant associations with vaccine uptake in the general population in other studies.
5.1. Limitations
There are some limitations to this study. Lactating women may have given birth in different types of hospitals, such as teaching, private, and charitable hospitals. The emphasis and education level on receiving the vaccine may have varied in the postpartum period. This could affect breastfeeding women’s decisions. In a study, women were asked whether they would choose to be vaccinated if scientific results showed that the vaccination is safe for breastfeeding women (47). So, future research should investigate the impact of hospital staff on promoting vaccination among women who have given birth in various hospital settings.
The findings of this study suggest the importance of emphasizing the benefits of strategies for preventing contagious infections, such as the COVID-19 vaccine and discussing the potential risks during breastfeeding. So, the health providers should respond to them. Breastfeeding women preferred to contact people for questions regarding the COVID-19 vaccination, such as talking to a gynecologist, a virologist, and a midwife (16). Additionally, this study highlights the role of husbands in increasing breastfeeding women’s knowledge about the safety and benefits of the COVID-19 vaccine. That is better when education is provided for breastfeeding women and their spouses. Future interventions would help the family with this issue.
5.2. Conclusions
In conclusion, the results of this study found that lactating women, both vaccinated and unvaccinated, were not different in age, education level, childbirth type, husbands’ occupation, economic household level, and history of COVID-19 infection. In contrast, there were significant differences in child numbers, occupation, husbands’ education level, type of baby feeding, fear of COVID-19, and self-efficacy. Finally, child numbers, husbands’ education level, and fear of COVID-19 predicted COVID-19 vaccination uptake. Breastfeeding women who had a lower fear of COVID-19 were more likely to get vaccinated. Additionally, the study found that lower education levels of husbands and a low number of children in families were associated with lower vaccination rates among lactating women. Vaccination is an increasingly critical aspect influencing the health and well-being of communities globally. When addressing the topic of unvaccinated breastfeeding women, it is imperative to adopt a comprehensive outlook, taking into account various factors. Deciding on receiving vaccines should involve consultation with healthcare providers, who can evaluate the risks and benefits based on the woman’s health condition, the well-being of her baby, and the prevalence of vaccine-preventable diseases within the community. It is suggested that the views of health providers who engage with pregnant and breastfeeding women about the causes of not receiving the COVID-19 vaccine be evaluated.
Vaccination also can contribute to community immunity, commonly known as herd immunity, which includes breastfeeding women. Health authorities are urging society to take the necessary steps to receive vaccine doses. Social media could have a key role in giving information to the community, especially breastfeeding women. A thorough understanding of the significance, safety, and effectiveness of vaccines is of utmost importance. So, the decision makers’ experiences could help future programs during such pandemics by integrating information about coping strategies related to refusing breastfeeding women. Ultimately, the choice to vaccinate is a personal one and should be based on a comprehensive comprehension of available information. To increase vaccination rates among lactating women, they should actively engage in prevention programs with trusted healthcare providers, considering their health, the well-being of their baby, and the broader impact on public health. It is crucial to develop education programs that focus on pregnancy care and preparation classes for childbirth. These programs should encourage the active participation of both women and their husbands, as they play a significant role in the decision-making process. Also, to enhance the outcomes associated with the rising vaccination rate, it is suggested to investigate the perspectives of husbands of breastfeeding women regarding COVID-19 vaccination through qualitative interventions.
