



1. Background
The pre-participation physical evaluation (PPE) aims to protect the health of athletes while they are practicing sports (1). The PPE assists the health team in decision-making about preventive, treatment, or rehabilitation measures to reduce potential risks from sports practice and return-to-play (2, 3). Thus, early identification of health problems increases the chances of the athlete playing safely - and consequently - for a longer time (3, 4). Among the evaluations that constitute the PPE, musculoskeletal screening is very important since more than 30% of the abnormalities found in an athlete's periodic health evaluation are related to musculoskeletal disorders (2).
However, the execution and interpretation of the results of the physical orthopedic examination (POE) require trained professionals and specialists (4), making its application particularly difficult in sports settings of less developed countries. Therefore, alternative means to detect musculoskeletal problems in athletes, such as questionnaires, represent an accessible and recommended way to evaluate readiness for sports participation (4). In this regard, some sport-related questionnaires have been used to identify injuries and health problems (5), as well as abnormalities in different anatomical sites, which could be risk factors for injuries in athletes (6-8). Overall, these questionnaires are not able to detect, at an early stage, athletes from different modalities who are at risk of developing a musculoskeletal injury due to sports practice.
Recently, Silveira Júnior et al. (9) developed and validated the Sport Readiness Questionnaire Focused on Musculoskeletal Injuries (MIR-Q) with Brazilian experts on sports medicine and orthopedics. The questionnaire enables identification of athletes at risk of future injuries or worsening of pre-existing injuries during training or competition, allowing their referral for specialized medical evaluation. As far as we know, the MIR-Q is the only instrument designed to screen readiness for sports practice focused on the musculoskeletal system, which can be used with athletes from different modalities and during different competitive periods (e.g. training, return to sport) (9). However, although the content of the MIR-Q has been previously validated through the Delphi technique, some psychometric properties of the instrument remain unknown.
2. Objectives
The objective of this study was to analyze the criterion-related validity, reliability (internal consistency and test-retest), and answers to the MIR-Q items. We hypothesized that (1) the MIR-Q has acceptable accuracy for musculoskeletal injury risk screening when compared with the clinical diagnosis of a physician as the reference standard, (2) the questionnaire produces reliable values.
3. Methods
3.1. Participants
Participants included 120 athletes from 12 different sport modalities (track and field (n = 11); soccer (n = 51); judo (n = 2); swimming (n = 1); cycling (n = 20); futsal (n = 10); karate (n = 3); rugby (n = 3); bodybuilding (n = 4); Brazilian jiu-jitsu (n = 12); Mixed Martial Arts (MMA, n = 2); beach volleyball (n = 1)) from the Medal-Project (Multiprofessional Evaluation: Determinants of Athletes Longevity and Performance), a project aimed at evaluating conditions that affect the health and performance of athletes. Eligible athletes included adults (≥ 18years), federated, and who practiced the sport with competitive goals. Parathletes and athletes who missed any stage of data collection were excluded. Athletes were informed of the study goals and procedures and provided written informed consent before participating. A convenience sample was used, i.e., athletes were selected based on availability and accessibility after contacting sports federations/clubs and coaches. The sample size was considered adequate since a minimum sample of 100 participants is sufficient to validate a survey (10).
Participants were 26.5 ± 8.7 years old, with 103 men (85.8%) and 8.9 ± 6.2 years of sport experience. Anthropometrically, the mean values were weight 74.2 ± 13.0 kg, height 173.8 ± 8.3 cm, and body mass index (BMI) 24.5 ± 3.3 kg/m². The study followed the guidelines of the 1975 Declaration of Helsinki and was approved by the Federal University of Mato Grosso do Sul.
3.2. Instruments and Data Collection
Firstly, participants completed the MIR-Q. The MIR-Q is a questionnaire for pre-participation in sport that contains six dichotomous questions (yes/no) covering signs or symptoms that put the athlete at risk of musculoskeletal injury during sports practice. Moreover, questions one to three require further information regarding the place where the athlete presented the sign or symptom described in the item (please see the Appendix in supplementary file). One or more affirmative (yes) questions on the MIR-Q was considered a positive result, suggesting a referral for a specialized medical evaluation (9).
After completing the MIR-Q, participants underwent a POE carried out independently by two orthopedic experts, who were unaware of the athletes' responses to the MIR-Q. The POE consisted of bone inspection, soft tissue palpation, strength and flexibility tests, and other special tests (11). The POE was considered positive when the specialist indicated the necessity of the treatment or complementary exams (e.g., X-ray, ultrasound, or MRI), as this may indicate a finding that puts the athlete at risk for practicing sports (2, 11).
3.3. Analysis of Validation and Reliability
The criterion-related validation was performed based on reports from the MIR-Q and POE. The positive responses to the MIR-Q and the indication from the POE for a medical referral were compared (2). The POE was considered a criterion because it has a good capacity to identify risk factors for injuries and pathological musculoskeletal conditions, proving to be an important component of PPE (2, 4, 11). Internal consistency was obtained with data from the first application of the MIR-Q (10). The MIR-Q test-retest was conducted with a sub-sample of athletes (n = 41), selected for convenience, with an interval of 7 to 14 days between the first and the second applications (10).
3.4. Statistical Analysis
Descriptive data are presented as mean, standard deviation, and percentages. Statistical tests were performed using Microsoft Excel 2010 ® (KR-20 test) and Bioestat 5.3 statistical programs. The data were dichotomized in '0' or ''1'', considering the negative and positive responses, respectively, for the MIR-Q and POE. Considering criterion-related validation, the sensitivity, specificity (10), and accuracy values of the MIR-Q (12) were used, with high values defined as > 0.70 (10, 13). The KR-20 test was used to check the internal consistency of the MIR-Q (14), and the Kappa agreement index was used for the test-retest method (15). Values > 0.70 were considered desirable for internal consistency (10). The test-retest values were classified as: no agreement (less than 0), poor (0.00 - 0.20), weak (0.21 - 0.40), moderate (0.41 - 0.60), strong (0.61 - 0.80), and excellent agreement (0.81 - 1.00) (15).
To analyze the proportion of responses to the MIR-Q, the Goodman test was used for contrasts between and within multinomial distributions (16). For all analyses, only the MIR-Q dichotomous questions were considered. A value of P < 0.05 was considered significant.
4. Results
The MIR-Q survey was associated with good sensitivity and moderate specificity. Sensitivity of the MIR-Q was 84.4% when compared to the medical recommendation for further treatment or evaluation in the POE. Regarding specificity, verified by comparing a negative MIR-Q with a result of no medical recommendation on the POE, remained 42.7%. Overall, the MIR-Q was 58% accurate. The relationship between the MIR-Q and POE is shown in Table 1.
Respective values for internal consistency and test-retest were considered moderate and weak; the MIR-Q internal consistency was 57%. Among 41 athletes that performed the test-retest between the two moments of evaluation (average of 7.3 days), 30 revealed similar reports on the MIR-Q. Even so, its stability was considered weak but significant (K = 0.30; P = 0.0249).
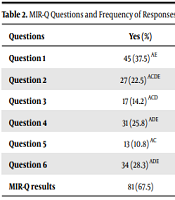
Proportions of MIR-Q reports are presented in Table 2, where it can be observed that eighty-one athletes (67.5%) answered "yes" to at least one of the six questions. In the individual context, question one (1) received more positive answers than questions three (3) and five (5) (P < 0.05). A total of 34 athletes (28.3%) confirmed a decline in performance in the previous six months (question 6), while 13 athletes (10.8%) reported mood swings (question 5) (P < 0.05). Regarding proportions of positive and negative responses, there was a significant difference between negative and positive MIR-Q reports (P < 0.05).
| Questions | Yes (%) | No. (%) |
|---|---|---|
| Question 1 | 45 (37.5) | 75 (62.5) * |
| Question 2 | 27 (22.5) | 93 (77.5) * |
| Question 3 | 17 (14.2) # | 103 (85.8) *# |
| Question 4 | 31 (25.8) | 89 (74.2) * |
| Question 5 | 13 (10.8) #$ | 107 (89.2) *# |
| Question 6 | 34 (28.3) † | 86 (71.7) *† |
| MIR-Q results | 81 (67.5) | 39 (32.5) |
Regarding the musculoskeletal evaluation, forty-five (37.5%) athletes had a positive POE. Computerized magnetic resonance imaging was the most commonly requested image exam (18 exams; 56.2%), followed by X-ray (10 exams; 31.3%), and ultrasonography (4 exams; 12.5%). A physiotherapy intervention was the most commonly indicated medical treatment (9 athletes; 69.2%) followed by muscular strengthening (4 athletes; 30.8%).
5. Discussion
In this study, the MIR-Q results demonstrated low reliability but acceptable values of validity. The sensitivity of the MIR-Q was considered high (84.4%), demonstrating its capacity to identify athletes that require specialized medical evaluation, therefore favoring timely treatment (4). In conditions where the presence of sports physicians is not accessible, the MIR-Q can be used to screen the majority of the athletes with a higher risk of musculoskeletal injuries while practicing sports, ensuring safer participation (9).
The MIR-Q specificity was considered moderate and equivalent to that observed by Smiths et al. (13). The authors found moderate values of specificity (54%) when comparing the questionnaire against a medical diagnosis of muscle-tendon injuries in novice runners. It is important to highlight that in the context of sports participation, a questionnaire with low specificity does not harm health but can be costly since it may lead to athletes being referred for unnecessary specialized medical evaluations. Additionally, overdiagnoses are likely to occur in these cases. Thus, despite their moderate specificity, questionnaires are still useful for screening athletes for adequate care (17). Regarding accuracy, the MIR-Q was moderately accurate to identify athletes requiring medical advice or specialized medical assistance (5). To maximize the accuracy of the MIR-Q, a better explanation of each question should be considered in future studies to increase athletes' understanding (13).
Concerning reliability parameters, the internal consistency of the MIR-Q was below the ideal values (10) and was lower compared to other questionnaires with similar constructions (6-8). Two main reasons may have weakened the internal consistency of the MIR-Q. First, the short size of the MIR-Q, as the relationship between the items on a questionnaire can be amplified by the addition of questions, i.e., extensive questionnaires tend to have greater internal consistency (10, 17). Second, the different aspects of the construct measured by the MIR-Q, i.e., injury risk, can be attributed to several factors such as overtraining, body alignment, and pain symptoms. Overall, questionnaires asking athletes about specific injury types can identify a greater number of problems in that location than when generalized questions are used (5) and, therefore, could have greater internal consistency compared to generalized questionnaires such as used on the MIR-Q. Despite these limitations, one of the greatest advantages of short questionnaires is that they are less time-consuming to participants, clinicians, and researchers, improving their feasibility in sports scenarios and epidemiological studies (6).
Concerning the temporal stability, the MIR-Q obtained low but significant Kappa values (P < 0.05). The interval between the first and second applications (7 - 14 days) may explain, in part, the low agreement (10). Lohrer et al. (7) obtained high test values of the Functional Assessment Scale for Acute Hamstring Injuries (ICC 0.98; P < 0.0001); however, the interval between applications was 2 - 3 days. The instability of the evaluated construct in the MIR-Q may also have contributed to the different responses at both moments and, consequently, to the low repeatability since musculoskeletal injuries are common in athletes and may have occurred during the interval between the applications (6, 17).
A careful and individualized look at the questions on the MIR-Q, which had the highest frequency of positive answers (questions one and six), allows us to understand their direct relation with the risk of sport participation. Question one refers to the pain experienced by athletes during sports participation that can affect their performance (9). Pain is classified as a health problem and deserves great attention by medical staff since it is a premonitory symptom of injury (18, 19). In addition, athletes with a pain complaint are twice as likely to be injured during a competition (20). Thus, the high number of positive responses to question 1 signals the importance of this item in the context of pre-participation screening, highlighting the need for constant monitoring (9). Another question with many positive answers was question six. The ability of athletes to perceive decrements in performance can be a sign of overtraining syndrome (21), which exposes them to the risk of illness (22) and injury (18). In clinical practice, the decrease in sports performance should be monitored, and adjustments made to the training plan, such as the adequacy of workloads, to protect the athletes against injuries caused by possible insufficient recovery (18, 21).
Our study has limitations that deserve to be highlighted. The sample had a small number of women and did not include adolescent athletes - which hinders the transfer of the findings to this population. In addition, further studies should investigate other psychometric properties of the MIR-Q, such as predictive validity. However, the MIR-Q demonstrated acceptable values of reliability and validity, enabling its use, particularly, in places without specialized medical assistance.
5.1. Conclusions
The MIR-Q demonstrated acceptable values of reliability and validity. Its use is justified in sports scenarios where the presence of specialized physicians is not a reality.
