1. Background
Prostate cancer is the most common cancer in men and usually occurs in men over 50 years of age (1). Men have a 10% risk of developing this cancer and about 3% of cases are fatal (2). The primary symptoms are frequent urination, intermittent and poor urine flow, urinary incontinence, blood in the urine (hematuria), semen excretion with pain, and persistent pain in the lower back. Digital rectal examination (DRE), biopsy, and measuring prostate-specific antigen (PSA) in the blood are methods to diagnose prostate cancer at the moment (3).
PSA is a glycoprotein produced both in cancerous and healthy epithelial cells that helps break down collagen in the semen and makes it clot. In prostate disease, over 4 ng/mL (recognized as normal) PSA leaks into the bloodstream. PSA test for diagnosis of prostate cancer has shown low sensitivity and specificity. For prostatitis and benign prostatic hyperplasia (BPH), the level of PSA may increase but, even with prostate cancer, it may be normal (1, 4).
A DRE shows changes in the shape and size of the prostate but is not sensitive. If the results of PSA and DRE are not normal, prostate cancer is generally confirmed by biopsy. It is the gold standard for the detection of prostate cancer, but it is highly invasive, costly, and painful. One of the most effective factors in increasing patient longevity to improve treatment and reduce the financial and mental costs to the patient is the quick and early diagnosis of cancer. Researchers are looking for such a method and have identified numerous biomarkers for detecting and tracking cancer. One of the most important biomarkers is microRNA (miRNA) (5, 6).
MicroRNA is a small, non-coding single-stranded RNA with a length of 21 to 23 nucleotides that are involved in the regulation of post-transcriptional expression of about 60% of human genes. They also regulate processes such as the proliferation, apoptosis, evolution, and differentiation of cancers and increase and decrease gene expression. This means that they can be used as biomarkers in the prognosis and diagnosis of diseases, including cancer, in the blood, urine, and tissue. They are found in plants, animals, and viruses, but they do not exist in bacteria. MicroRNAs can directly regulate oncogenes and tumor suppressor genes, so they can play an oncogenic or tumor suppressor role depending on the function of their target mRNAs (7, 8).
Early evidence of the association between miRNA and cancer was presented by Calin in 2002. He showed that, in many patients with chronic lymphocytic leukemia (CLL), a piece of the genome had been removed, including the miR-15a and miR-16 gene clusters (9). The profile of the microRNAs (miRNAs) involved in prostate cancer was published in 2007 (10).
One type of miRNAs that plays a role in prostate cancer is miR-21. This miRNA can inhibit the expression of PTEN (tumor suppressor gene) and increase the aggressive proliferation of cancer cells (11). This miRNA is classified as an oncomir. The most important target mRNAs are PDCD4, TPM1, TIMP3, MARCK, and PTEN (12, 13). It plays an important role in bone metastasis in the advanced stages of prostate cancer and it is located on chromosome 17 (14, 15). Another type of miRNA that plays a role in prostate cancer is miR-214. The miR-214 is one of the most important miRNAs that plays a role in cancers, especially prostate cancer, and the most important target mRNAs are EZH2 and CTNNB1 (12). It is located on chromosome 1 (15).
2. Objectives
In this study, the expression of miR-21 and miR-214 in urine samples of patients with prostate cancer (metastatic and non-metastatic) and healthy subjects, receiver operating characteristic (ROC) curve analysis for each miRNA, and comparison of them with the results of the PSA test were investigated.
3. Methods
3.1. Collection of Urine Samples
Urine samples (15 mL) were collected from suspected prostate cancer patients, who were referred to Hashemi-Nejad Hospital in Tehran, Iran for biopsies from April 2017 to March 2018. The urine samples were transferred to the Molecular Genetics Laboratory of the Cancer Institute of Imam Khomeini Hospital (Tehran, Iran) and stored at 4°C for up to 3 hours and, then, were centrifuged at 3500 rpm for 5 min at 4°C. Urine samples were stored at -80°C. Based on the pathology report, 70 urine samples were diagnosed with prostate cancer (32 metastatic and 38 non-metastatic); 30 urine samples were from healthy participants who had received negative biopsy reports.
All participants have been informed and completed a consent form and a questionnaire before enrollment. All patients’ information was kept confidential.
This study was approved by the Ethics Committee of Islamic Azad Tehran Medical Sciences University, Pharmacy and Pharmaceutical Branches Faculty (IR.IAU.PS.REC.1397.112).
3.2. Inclusion and Exclusion Criteria
3.2.1. Inclusion Criteria
Patients diagnosed with prostate cancer (according to pathology reports), who had no other related diseases were included.
3.2.2. Exclusion Criteria
Patients who were sampled after a biopsy, patients who received any treatment such as chemotherapy, radiotherapy, and patients with related diseases such as bladder and kidney diseases were excluded.
3.3. RNA Extraction from the Urine
RNA was extracted by using 500 μL of Trizol (Invitrogen; USA) in 2 mL of urine samples according to manufacturer's protocol such as Yang and Wang studies (16, 17). A NanoDrop 2000 spectrophotometer (Thermo Scientific; USA) was used to detect the concentration and purity of extracted RNA (ng/μL). RNA with OD260/OD280 ratio between 2 and 2.2 was taken. The extracted RNA was stored at -80°C until cDNA synthesis.
3.4. cDNA Synthesis
RNA was converted to cDNA by using a Pars Genome MiR-Amp kit (Iran) according to the manufacturer's protocol. The cDNA was stored at -20°C until a quantitative reverse transcription-polymerase chain reaction (qRT-PCR) was performed.
3.5. qRT-PCR
The expression level of miR-21 and miR-214 were measured for 70 prostate cancer patients (32 metastatic and 38 non-metastatic) and 30 healthy subjects by using a real-time PCR system (Bioneer; South Korea). Urine samples were normalized to internal standard control U6snRNA. This method was chosen for its precision, high sensitivity, and low cost. The forward and reverse primer sequences for miR-21, miR-214, and internal reference (U6SnRNA) were designed (Table 1).
Table 1.
Primer Sequences of miR-21, miR-214, and U6SnRNA
| MicroRNA | Forward | Reverse |
|---|---|---|
| miR-21 | 5′-GTGCAGGGTCCGAGGT-3′ | 5′-GCCGCTAGCTTATCAGACTGATGT-3′ |
| miR-214 | 5′-GCGGCACAGCAGGCACAGACA-3′ | 5′-TGCAGGGTCCGAGGT-3′ |
| U6SnRNA | 5′-CTCGCTTCGGCAGCACA-3′ | 5′-AACGCTTCACGAATTTGCGT -3′ |
Real-time PCR reaction system (14 μL): SYBR Green Master Mix (Takara; Japan) 7 μL, specific primers (10 pmol) 1 μL, cDNA diluted 1 to 4, 3 μL and distilled water 3 μL. Real-time PCR conditions: Polymerase activation at 95°C for 12 minutes, denaturation at 95°C for 15 seconds, annealing 60°C for 30 seconds, and extension at 72°C for 15 seconds for 42 cycles. The experiment was repeated 3 times for each sample. For each miRNA and U6snRNA, no template control (NTC) was provided, which lacked a template (cDNA) for reproduction. PCR performance was calculated by using the standard curve and serial dilutions of 107%. Finally, 2% agarose gel electrophoresis was used to ensure the reproduction and specificity of the components.
3.6. Statistical Analysis
The 2-∆∆Ct method was used for pre-processing and fold-change calculations. Analysis of data from real-time PCR was performed by using REST 2009 software. All statistical calculations and charts were performed by using SPSS 22 and P < 0.05 was considered significant. The sensitivity and specificity of each miRNAs were calculated by using Medcalc18.2.1 software. The ROC curve was plotted and the area under the curve (AUC) was calculated. All the box plots represent miRNA levels relative to U6snRNA and they are plotted by using formula 2−∆Ct in Medcalc18.2.1 software.
4. Results
The clinical and pathological data of the patients with prostate cancer and healthy subjects with negative biopsy reports are based on the pathology results (Table 2). miR-21 and miR-214 showed significant changes in the expression of prostate cancer patients compared to the healthy subjects.
Table 2.
Clinical and Pathological Characteristics of Patients with Prostate Cancer and Healthy Subjects a
| Variables | Patients with Prostate Cancer | Metastatic Group | Non-metastatic Group | Healthy Subjects |
|---|---|---|---|---|
| Number | 70 | 32 | 38 | 30 |
| Age (y), mean ± SEM | 69.83 ± 1.03 | 70.62 ± 1.68 | 69.16 ± 1.29 | 65.97 ± 1.32 |
| Range | 45 - 87 | 45 - 87 | 48 - 86 | 52 - 84 |
| Serum PSA (ng/mL), mean ± SEM | 18.03 ± 3.77 | 31.39 ± 7.64 | 6.77 ± 0.51 | 7.08 ± 0.53 |
| Range | 1 - 170.6 | 4.7 - 170.6 | 1 - 21 | 2 - 13.2 |
| Gleason score mode | 7 | 8 | 7 | - |
| Range | 6 - 10 | 7 - 10 | 6 - 7 | |
| Grade mode | 2 | 4 | 2 | - |
| Range | 1 - 5 | 3 - 5 | 1 - 2 |
Abbreviations: SEM, standard error of the mean; PSA, prostate specific antigen.
a A Gleason score < 7 is considered a low grade; a Gleason score of 7 is considered intermediate grade; and a Gleason score > 7 is considered a high grade.
4.1. Expression of miR-21 in the Urine Samples of People with Prostate Cancer
The miR-21 significantly increased (P = 0.003) in the prostate cancer group compared with the control group with a fold change of 3.493. The expression of miR-21 in the metastatic and non-metastatic prostate cancer subgroups was examined and was significantly different. The metastatic subgroup showed a significant increase in expression (P = 0.042) compared to the non-metastatic subgroup (P = 0.036). The rate of expression (fold change) miR-21 was 3.911 in the metastatic subgroup and 3.176 in the non-metastatic subgroup (Figure 1).
 in the prostate cancer group compared with the control group (fold change = 3.493); B, the metastatic subgroup showed a significant increase in expression more than the non-metastatic subgroup (P = 0.042 and fold change = 3.911); C, the non-metastatic subgroup showed a significant increase in expression and less expression than the metastatic subgroup (P = 0.036 and fold change = 3.176).")
Figure 1.
Expression of miR-21 in A, prostate cancer; B, metastatic subgroup; and C, non-metastatic subgroup. A, the miR-21 significantly increased (P = 0.003) in the prostate cancer group compared with the control group (fold change = 3.493); B, the metastatic subgroup showed a significant increase in expression more than the non-metastatic subgroup (P = 0.042 and fold change = 3.911); C, the non-metastatic subgroup showed a significant increase in expression and less expression than the metastatic subgroup (P = 0.036 and fold change = 3.176).
4.2. Expression of miR-214 in the Urine Samples of People with Prostate Cancer
The miR-214 showed a significant decrease in expression (P = 0.000) in patients with prostate cancer with a fold change of 0.008. Expression of miR-214 in the metastatic and non-metastatic prostate cancer subgroups was investigated. In the metastatic subgroup, the expression level (fold change) was 0.007 and, in the non-metastatic subgroup, the expression level was 0.011. The metastatic subgroup showed a significant decrease in expression (P = 0.000) compared to the non-metastatic subgroup (P = 0.000) (Figure 2).
 in the prostate cancer group compared with the control group (fold change = 0.008); B, the metastatic subgroup showed a significant decrease in expression more than the non-metastatic subgroup (P = 0.000 and fold change = 0.007); C, the non-metastatic subgroup showed a significant decrease in expression and more expression than the metastatic subgroup (P = 0.000 and fold change = 0.011).")
Figure 2.
Expression of miR-214 in A, prostate cancer; B, metastatic subgroup; and C, non-metastatic subgroup. A, the miR-214 significantly decreased (P = 0.000) in the prostate cancer group compared with the control group (fold change = 0.008); B, the metastatic subgroup showed a significant decrease in expression more than the non-metastatic subgroup (P = 0.000 and fold change = 0.007); C, the non-metastatic subgroup showed a significant decrease in expression and more expression than the metastatic subgroup (P = 0.000 and fold change = 0.011).
The expression of miR-214 and miR-21 in the prostate cancer and control groups were calculated separately by using the formula 2-∆Ct and is plotted in Figure 3.

Figure 3.
Box plot of miR-21 and miR-214 in urine samples. A, box plot of 70 urine samples from patients with prostate cancer that shows increased expression of miR-21 over samples of 30 from healthy subjects; B, miR-214 shows decreased expression in the prostate cancer group compared with the control group.
4.3. ROC Curve Analysis of miR-21, miR-214, and PSA
The ROC curve was used to determine the specificity and sensitivity of miRNA for the identification of prostate cancer. This statistical analysis shows the efficacy of miRNA as a diagnostic biomarker. The specificity index provides the ability to diagnose a cancer sample from non-cancerous samples. The sensitivity index confirms its ability to diagnose the disease for the patient. The AUC indicates the biomarker's prediction power.
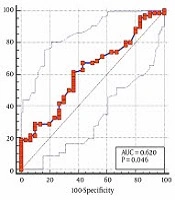
In ROC curve analysis, miR-21 showed 100% specificity, 64.29% sensitivity and AUC = 0.643 and miR-214 showed 100% specificity, 84.29% sensitivity, and AUC = 0.843. The combined panels of miR-21 and miR-214 had 100% specificity, 72.14% sensitivity, and AUC = 0.721. PSA showed 63.33% specificity, 61.43% sensitivity, and AUC = 0.620. Compared to miRNA, PSA shows less specificity and sensitivity (Figure 4 and Table 3).

Figure 4.
ROC curve analysis. A, the ROC curve analysis of miR-21; B, the ROC curve analysis of miR-214; C, the ROC curve analysis of miR-21 + miR-214; D, the ROC curve analysis of PSA.
Table 3.
Data of ROC Curve Analysis b
| Variables | miR-21 | miR-214 | miR-21 and miR-214 | PSA |
|---|---|---|---|---|
| Specificity (%) | 100 | 100 | 100 | 63.33 |
| Sensitivity (%) | 64.29 | 84.29 | 72.14 | 61.43 |
| AUC | 0.643 | 0.843 | 0.721 | 0.620 |
| P-value | 0.0133 | 0.0001 | 0.0001 | 0.0464 |
| 95% CI | 0.541 - 0.736 | 0.756 - 0.908 | 0.654 - 0.782 | 0.517 - 0.715 |
| SE | 0.0577 | 0.0438 | 0.0380 | 0.0600 |
Abbreviations: PSA, Prostate Specific Antigen; AUC, Area under the Curve; CI, confidence interval; SE, standard error.
b P-value < 0.05 is significant.
5. Discussion
Changes in lifestyle and eating habits, alcohol and tobacco use, electromagnetic radiation, and environmental pollution have increased the incidence of cancer year by year. Most diagnostic methods are invasive or do not have high specificity and sensitivity.
In recent years, many diagnostic biomarkers in the biological samples of patients have been introduced for the diagnosis of cancer. These biomarkers are often proteins or nucleic acid, but they have low specificity and sensitivity. MicroRNA is a new generation of diagnostic biomarkers, including in tumor tissue, showing different expression patterns for cancer. The pattern of expression of miRNA in human cancers is tissue-dependent and miRNA is significantly more stable under severe environmental factors (18, 19). Because miRNA circulating in the blood and other biological fluids are more stable with longer half-lives than proteins, their profile can be used to differentiate cancer from other diseases. Biological fluids such as blood and urine are convenient and non-invasive vehicles for collection and provide good samples for laboratory and diagnostic research. Finding miRNA biomarkers in such fluids that can accurately detect cancer is a major goal of researchers (20).
Stuopelyte et al. in Lithuania studied the expression of miR-21, miR-19a, and miR-19b in tissue and urine specimens. The expression of miRNA was evaluated by RT-qPCR. This study showed that the miRNAs were expressed in the tissue and the urine sedimentation of the prostate cancer group. Urinary miR-21 has a significant potential for the differentiation of prostate cancer patients and individuals with BPH. The combined panels of the three miRNAs in urine have more power to detect prostate cancer compared to the PSA (21).
Foj et al. in Spain studied the expression of miR-21, miR-141, miR-214, miR-375 and let-7c on 60 urine specimens of patients with prostate cancer and 10 healthy subjects. Their results showed that miR-21 (P = 0.001 and AUC = 0.817), miR-141 (P = 0.033 and AUC = 0.712), and miR-375 (P = 0.038 and AUC = 0.707) increased and miR-214 (P = 0.049 and AUC = 0.716) showed low expression level. No significant difference was found for let-7c (P = 0.185 and AUC = 0.636). Combined panels of miR-21 and miR-375 have been proposed for differentiation of cancerous and healthy patients (P < 0.0001 and AUC = 0.872) (22).
Koppers-Lalic et al. in the Netherlands studied the expression levels of miR-21, miR-204, and miR-375 on 48 urine specimens of prostate cancer patients and 26 urine samples from healthy subjects performed by qRT-PCR. The results showed that all three miRNAs increased in patients with prostate cancer. Ultimately, the miR-21, miR-204, and miR-375 combination had a sensitivity of 72.9, 88% specificity and, AUC = 0.866 compared to the PSA has a sensitivity of 70.8, 60% specificity, and AUC = 0.707 (23).
As mentioned, miR-21 inhibits the expression of PTEN in prostate cancer and it can increase cancer cell proliferation and cause bone metastasis. MiR-214 also controls various genes involved in prostate cancer, such as EZH2. Due to the study of these miRNAs in the serum and plasma of people with prostate cancer in previous studies, 3 miRNAs were selected and investigated in the urine samples (24).
The results of the present research showed that miR-21 in patients with prostate cancer significantly increased (P = 0.003) in comparison with the healthy subjects. It was shown that the expression of this miRNA was significantly different between the metastatic and non-metastatic subgroups. In the metastatic subgroup (P = 0.036), the expression was higher than the non-metastatic subgroup (P = 0.042). The miR-214 showed a significant decrease in expression in the prostate cancer group (P = 0.000) compared with the healthy control group. The results between the metastatic and non-metastatic subgroups indicated that the expression of miR-214 was significantly different between groups and was lower in the metastatic subgroup (P = 0.000) than the non-metastatic subgroup (P = 0.000).
The results of ROC curve analysis showed that miR-214 had more sensitivity and diagnostic power than miR-21 and the combination panel of the two miRNAs had the greater diagnostic ability and higher specificity and sensitivity than the PSA test. Compared to other methods, such as biopsy, it is superior. The results of this study were consistent with the results of other studies.
In our study, these two miRNAs were investigated as a combined panel in the urine of patients with prostate cancer in a larger group than other studies. Due to the low miRNAs in the urine and the difficulty of studying it, less research has been done on urine. Other innovations of this research include a study in two subgroups of metastatic and non-metastatic in patients with prostate cancer.
5.1. Conclusions
The miR-21 and miR-214 combined panels can be used as a non-invasive diagnostic method for the diagnosis of prostate cancer. It is hoped that, with further research on miRNAs and cancer, the use of miRNA as a non-invasive and accurate diagnostic method will replace current diagnostic tests in laboratories. Early diagnosis of cancer before metastasis can allow earlier treatment and increase the life expectancy of the affected patients.


