



Dear Editor,
Open radical nephrectomy (RN) in large renal tumors with hilar invasion or extensive hilar lymphadenopathy is a demanding surgery, with a high propensity for blood loss and post-operative morbidity. These complex surgeries require extensive surgical skills and considerable expertise in vascular techniques. The presence of tumor thrombosis, which occurs in 5% to 15% of cases, makes nephrectomy even more complicated (1). Moreover, extensive fatty tissue over the renal hilum in some kidneys and insufficient space for dissection, is another complicating factor, imposing some surgeons to implement en-bloc stapler or suture for ligation of the entire pedicle (2).
Recent advancements in robotic surgery and its wide adoption across the United States and Europe have drifted the trend towards robotic-assisted radical nephrectomy for large renal masses. However, due to higher overall costs, it is still not accessible in all urologic centers. Moreover, it has the potential disadvantage of lack of tactile feedback, making the open RN favorable in complex renal masses (3). Hence, open RN is still recommended for large/complex kidney tumors, cytoreductive nephrectomy, and RCCs with high-level of the Inferior Vena Cava (IVC) thrombosis (4).
Given these difficulties, we aimed at introducing a technique called “Tactile Ligation Technique” to facilitate the ligation of renal vasculature in open RN in complex renal masses either with or without tumor thrombosis.
Technique Presentation: For complex renal masses, the general approach is through a midline laparotomy incision. However, our technique is also practical through a chevron or thoracoabdominal incision. After reflecting the small bowel and the colon, the retroperitoneal space is opened. Before manipulating the cancerous tissue, we should dissect the ipsilateral artery and vein by first opening the posterior peritoneum over the IVC on the right side or the most medial part of the renal pedicle (adjacent to the aorta) on the left side.
From the anatomical standpoint, in the right RN, we do have access to the right renal artery in the inter-aorto-caval space, beneath the left renal vein. Since this has some distance from the right renal hilum, it makes the right renal artery more accessible than the left renal artery, which is only accessible underneath the left renal vein adjacent to the left renal hilum. Nevertheless, in extensive lymphadenopathies, reaching the inter-aorto-caval space is equally difficult and the surgeon has no choice but to ligate the artery in proximity to the renal pedicle.
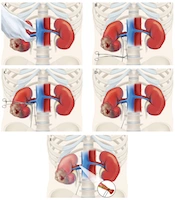
In right-side nephrectomy, after opening the posterior peritoneum over the IVC, the next step is to encircle the tissues around the renal hilum, adjacent and anterior to vertebrae, with the thumb and index finger, trying to control all the tissues around the renal hilum, i.e., renal artery (ies) and vein (s), as well as lymphatic and adipose tissue (Figure 1A). With tactile sensation, the finger is kept over the vertebrae, trying to include all the hilar structures. In some cases, the pulsation of the renal artery can be felt, which makes the dissection much easier.

A, Encircling the tissues around the renal hilum with the thumb and index finger; B, Passing a 1-0 silk tie around the hilum with a Satinsky clamp; C, Passing the silk tie beneath the vein with the help of the forceps; D and E, Force closure of the tissues behind the renal vein.
After encircling the tissues with two fingers, with the help of a right angle forceps or a Satinsky clamp, a 1-0 silk tie is placed around the whole hilum (Figure 1B). Then, the surgeon dissects the renal vein, separating it from the rest of the tissues, and again with the help of a right angle forceps, the silk tie is passed beneath the vein (Figure 1C). Now, the tie circles the artery, as well as the other adipose and lymphatic structures. In the next step, the silk suture is tied with as much force as possible to force shot the renal artery (ies). The effect of arterial clamping should be seen immediately in the kidney (Figure 1D and E). If not, another tie should be placed in the same manner to augment the closure. After clamping the renal artery, the rest of the surgery will be the same as a regular nephrectomy; however, it is worth mentioning that this is only a temporary vascular control and after excising the kidney, the renal artery should be isolated and suture ligated to prevent delayed bleeding. This technique can be implemented for the left radical nephrectomy in the same manner. In cases with tumor thrombosis, after clamping the renal artery, the vein is kept intact until the cephalad part of the tumor thrombosis is found and controlled.
Vascular control is a critical step during RN, which can be accomplished with several techniques (5). To our knowledge, the “Tactile Ligation Technique” has not been mentioned in the literature. So far, we have applied this technique in over 50 locally advanced RCC cases with extensive hilar involvement and we found it safe with a low learning curve. Evidently, this claim needs verification in a comparative trial with statistical details.
