





1. Background
In 2020, approximately 2.3 million women were diagnosed with breast cancer (BC) and 685,000 died from the disease. The BC accounts for 25% of all cancer cases in women and was the most commonly diagnosed cancer among women in 2020. Its burden is rising, particularly in developing countries. The number of disability-adjusted life years (DALYs) due to BC among women worldwide is higher than that of any other cancer (1, 2).
Although BC is recognized as a disease in developed countries, approximately 50% of patients with BC and 58% of BC – related deaths occur in less developed countries. Between 1980 and 2020, age-adjusted BC mortality in high-income countries declined by 40%. If a global annual reduction in mortality of 2.5% were achieved, an estimated 2.5 million BC deaths could be prevented between 2020 and 2040 (2, 3).
In 2019, the number of patients with BC in Iran was 78,415 with an age standard incidence rate of 98.5 per 100,000 population (4). Approximately 51% of patients were younger than 50 years old. It is estimated that around 10,000 women are diagnosed and treated for BC annually (5). According to the 2020 World Health Organization (WHO) data, Iran reported 16,967 new BC cases, accounting for 0.75% of global cases. The BC represented about 12.9% of all newly diagnosed cancers in the country (131,191 cases) (6).
Breast cancer is a costly disease for both insurance organizations and patients. A study in Italy revealed that over 75,000 women are hospitalized annually due to BC, with total cost hospitalization costs reaching approximately 300 million euros per year. This study found that early-stage BC costs €8,828 per year, while secondary neoplasms cost 9,780€, with an average total economic burden of 257€ million per year (7). A study in the Netherlands showed that the overall incidence of BC increased from 103.4 to 153.2 per 100,000 women between 1990 and 2014. The BC is also responsible for approximately 3,100 deaths, 26,000 years of life lost (YLLs), 65,000 DALYs and an economic burden of 1.27€ billion annually in the Netherlands (8). An estimate of the costs of the National Health Fund (NHF) in Poland for the diagnosis and treatment of patients with BC showed that nearly 50% of the total direct costs were spent on pharmaceutical costs, 15% on surgery, 12% was spent on radiotherapy and 10% on screening program (9).
Out-of-pocket (OOP) costs incurred by BC patients are significant even for patients with insurance coverage (10, 11). A study by Daroudi et al. in 2014 estimated that the economic burden of BC in Iran was 947$,374,468. Most of the cost (77%) was related to lost productivity due to BC mortality. Direct medical costs accounted for 18.56% of the total estimated cost. Of the 175,860,607$ in direct medical costs, chemotherapy accounted for the largest cost (76,755,740$), and trastuzumab accounted for 41% (31,529,280$) (12). Evidence suggests that one of the challenges faced by BC patients during the COVID-19 pandemic in the country was the inadequate financial support of health insurances providers in covering the costs of services and medicines they need (13).
The Iranian Health Insurance Organization (IHIO) covers almost half of Iran's population under basic insurance (14). To date, no study has utelized IHIO data to examine the frequency and costs of BC in Iran.
2. Objectives
Therefore, considering the high prevalence of BC and Iranian families facing the back-breaking and impoverishing costs of this disease, this study was conducted with the aim of determining the prevalence, mortality and costs of BC using the IHIO database.
3. Methods
3.1. Study Population
This study was conducted as a descriptive, cross-sectional, and retrospective study using the database of the IHIO. Data were extracted and collected using a census method from the profile of 42,296,124 indiniduals in 2021 and 44,303,244 individuals in 2022 who were covered by IHIO. First, BC patients were examined in terms of demographic variables such as age, sex, and province of residence. Then, incidence, prevalence, mortality and cost data were extracted for all profiles of BC patients.
3.2. Data Procedures
Data on prevalence (any BC diagnosis during 2021 and 2022) and incidence (new BC diagnosis in a given year without a previous diagnosis in the previous year) were collected. International classification of diseases, 10th revision (ICD-10) was used to diagnose BC patients.
Information on BC mortality was collected from the discharge statuses of inpatients indicating death. Once death was confirmed, the percentage of the population that died from BC was calculated by merging the records of the deceased with the existing cancer group records.
The BC-related costs were calculated by summing service costs using the ICD-10 from outpatient and inpatient data. Additionally, for patients with an ICD-10 diagnosis code associated with BC for each year, chemotherapy costs were included in total costs. The average cost of each person was calculated by adding up hospital costs (hospitalization, surgery, medicine, etc.) and chemotherapy for each patient. Then, the total average was calculated based on the type of cost, separated by year for 2021 and 2022. The eligibility criteria for selecting patients for cost analysis were:
3.2.1. Inclusion Criteria
- No complete recovery within the past year (continuation of the treatment process).
- Having a ducumented BC profile in the incurable fund of the IHIO.
3.2.2. Exclusion Criteria
- Incomplete patient medical records.
- Having other chronic diseases that may interfere with the analysis of the results.
3.3. Statistical Analysis
Descriptive statistical methods (mean, frequency, and percentage) were used to analyze the data, which were processed using SPSS version 21 and Microsoft Excel 2016.
4. Results
In 2021, the total insured population covered by IHIO was 42,296,124, of which 12,333 were diagnosed with BC. In 2022, the total insured population covered by IHIO was about 44,303,244, of which 15,897 were diagnosed with BC (Table 1). Table 2 shows the gender distribution of BC patients.
| Year | The Insured Population Covered by IHIO | Prevalence | Incidence | Mortality | Prevalence per 100,000 Individuals | Incidence per 100,000 Individuals | Mortality per 100,000 Individuals |
|---|---|---|---|---|---|---|---|
| 2021 | 42,296,124 | 12333 | - | 287 | 29.16 | - | 0.68 |
| 2022 | 44,303,244 | 15897 | 3109 | 382 | 35.88 | 7.02 | 0.86 |
Prevalence, Incidence, and Mortality of Breast Cancer Patients Covered by Iran Health Insurance Organization
| Gender | Frequency (%) |
|---|---|
| Female | 27429 (97.16) |
| Male | 801 (2.84) |
| Total | 28230 (100) |
Gender of Breast Cancer Patients
Table 3 shows the frequency and percentage of BC patients by age group. The largest number of BC patients were in the age group of 41 - 50 years.
| Age Group | Frequency (%) |
|---|---|
| 21 ≤ | 63 (0.22) |
| 21 - 30 | 451 (1.60) |
| 31 - 40 | 3,550 (12.58) |
| 41 - 50 | 8,778 (31.09) |
| 51 - 60 | 8,038 (28.47) |
| 61 - 70 | 4,992 (17.68) |
| 71 - 80 | 1,982 (7.02) |
| 81 ≥ | 376 (1.33) |
| Total | 28,230 (100) |
Frequency and Percentage of Breast Cancer Patients by Age Group
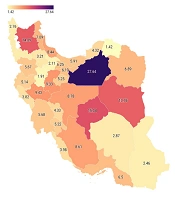
Figure 1 shows that the highest number of BC cases per 10,000 individuals during 2021 and 2022 was in Semnan province (27.64), Yazd province (15.04), East Azerbaijan province (14.09), and South Khorasan province (13.76). The lowest number was in North Khorasan (1.42) and Hamedan province (1.91) per 10,000 individuals. Overall, the number of BC cases in Iran during 2021 and 2022 was 63.7 per 100,000 individuals.
 cases per 10,000 population in Iran by province during 2021 and 2022")
Number of breast cancer (BC) cases per 10,000 population in Iran by province during 2021 and 2022
Figure 2 shows the frequency of ownership of health service providers from the total expenses of the IHIO. Most BC patients refer to government-university medical centers for inpatient services with 76% and 18% refer to private centers for inpatient services.
")
Frequency of ownership of centers providing health services from the total expenses of the Iran Health Insurance Organization (IHIO)
Figure 3 shows the frequency of ownership of health service providers from the total cost (IHIO share and patient share or OOP). Considering the patient share or OOP, 50% of BC patients went to government-university medical centers for inpatient services, and 40% went to private centers. Figures 2 and 3 show that IHIO pays a smaller share of costs in private sector.
![Frequency of ownership of health service providers from the total cost [Iran Health Insurance Organization (IHIO) share and patient share or out-of-pocket (OOP)]](https://services.brieflands.com/cdn/serve/3170b/63c7ba2fdfa3639c1ae59d0cb941dd1cf0ecf6c9/ijcm-157981-i002-F3-preview.webp "Frequency of ownership of health service providers from the total cost [Iran Health Insurance Organization (IHIO) share and patient share or out-of-pocket (OOP)]")
Frequency of ownership of health service providers from the total cost [Iran Health Insurance Organization (IHIO) share and patient share or out-of-pocket (OOP)]
Figure 4 shows that the highest costs (organization's contribution) were at the ages of 49 to 55.
![Total cost [Iran Health Insurance Organization (IHIO) share and patient share or out-of-pocket (OOP) in 2021 and 2022] by age](https://services.brieflands.com/cdn/serve/3170b/4f48bfee3979f085d0614194579c3dfcdf9812f9/ijcm-157981-i003-F4-preview.webp "Total cost [Iran Health Insurance Organization (IHIO) share and patient share or out-of-pocket (OOP) in 2021 and 2022] by age")
Total cost [Iran Health Insurance Organization (IHIO) share and patient share or out-of-pocket (OOP) in 2021 and 2022] by age
Table 4 shows that among inpatient expenses, the highest expenses related to radiotherapy (22.70%), Hotelling (18.80%), and drug (16.57%), respectively.
| Services | Percentage |
|---|---|
| Radiotherapy | 22.70 |
| Hoteling | 18.80 |
| Drug | 16.57 |
| Surgical services | 13.10 |
| Chemotherapy | 3.46 |
| Visit | 3.23 |
| Nursing Care | 3.17 |
| Medical diagnostic tests | 2.96 |
| Operating room consumables | 2.40 |
| Pathology | 2.40 |
| Nursing services | 1.77 |
| Consulting services | 1.13 |
| Medicine used in the operating room | 1.12 |
| Consumables in the department | 1.06 |
| Others | 6.14 |
Inpatient Expenses by Service
Table 5 shows that in 2021, 71.43% of the costs for physiotherapy services were paid OOP, 71.25% for laboratory services, 68.35% for imaging, and the lowest percentage for drug services was 15.32% and inpatient services were 48%. Overall, the OOP costs for BC patients in 2021 were 33.72%. Drug costs accounted for 52.13%, inpatient costs for 30.75% of the total costs in 2021.
| Type of Service | Number of Service | Total Cost (USD) | Share of the IHIO (USD) | Share of the IHIO (%) | OOP (%) |
|---|---|---|---|---|---|
| Drug | 309,517 | 1,964,722 | 1,663,686 | 84.68 | 15.32 |
| Laboratory | 225,171 | 126,224 | 36,294 | 28.75 | 71.25 |
| Imaging | 25,318 | 162,240 | 51,349 | 31.65 | 68.35 |
| The service of doctors | 3,613 | 54,837 | 27,302 | 49.79 | 50.21 |
| Physiotherapy | 344 | 7,098 | 2,028 | 28.57 | 71.43 |
| Visit | 11,448 | 294,921 | 114,766 | 38.91 | 61.09 |
| Inpatient | 12,282 | 1,158,760 | 602,554 | 52 | 48 |
| Total | 587,693 | 3,768,803 | 2,497,980 | 66.28 | 33.72 |
Costs by Service in 2021
Table 6 shows that in 2022, 72.29% of laboratory, 67.96% of physiotherapy, and 65.96% of visits were paid OOP. The lowest percentage of OOP related to drug services was 13.21% and doctor service was 47.32%. Overall, the OOP costs for BC patients in 2022 were 29.45%. Drug costs accounted for 59.72%, Inpatient costs for 30.08% of the total costs in 2022.
| Type of Service | Number of Service | Total Cost (USD) | Share of the IHIO (USD) | Share of the IHIO (%) | OOP (%) |
|---|---|---|---|---|---|
| Drug | 401,849 | 4,230,900 | 3,672,016 | 86.79 | 13.21 |
| Laboratory | 274,143 | 196,253 | 54,384 | 27.71 | 72.29 |
| Imaging | 34,018 | 268,944 | 94,925 | 35.3 | 64.7 |
| The service of doctors | 5,099 | 107,746 | 56,765 | 52.68 | 47.32 |
| Physiotherapy | 445 | 11,875 | 3,818 | 32.15 | 67.85 |
| Visit | 10,643 | 137,579 | 46,838 | 34.04 | 65.96 |
| Inpatient | 15,897 | 2,130,847 | 1,069,083 | 50.17 | 49.83 |
| Total | 742,094 | 7,084,144 | 4,997,831 | 70.55 | 29.45 |
Costs by Service in 2022
Tables 5 and 6 showes that in 2022, compared to 2021, OOP payments decreased. Also, the OOP costs for drug services in 2021 were 15.32%, which decreased to 13.21% in 2022. The total cost of BC in 2021 was equal to 1,884,401,272,775 Rials (considering the dollar of five hundred thousand rials was equal to 3,768,802$) and in 2022, it was equivalent to 3,542,071,922,859 Rials (considering the dollar of five hundred thousand rials was equal to 7,084,143$). The total cost of BC in 2022 has increased by 88% compared to 2021. The annual cost per person was 305$ in 2021 and 446$ in 2022.
5. Discussion
The prevalence of BC in the population covered by IHIO per 100,000 was 29.16 and 36.88 in 2022. The incidence rate in 2022 was 7.02 per 100,000 population. The OOP costs accounted for 33.72% in 2021 and 29.45% of total direct BC costs in 2022. In 2021, there were 0.68 deaths per 100,000 and in 2022, 0.86 per 100,000. The results of our study showed that among different age groups, the highest cost was related to the 50 - 60 age group. Other studies have shown that BC treatment costs decreased significantly with age, from 69,121$ for women younger than 45 years to 23,805$ for those 80 years or older (15). Other studies have shown that BC treatment costs generally increase as the disease progresses (7, 16-18). Another study showed that the highest cost occurred during the first 2 years after diagnosis (19). Since the average age in BC diagnosis in Iran is approximately 10 years lower than in European countries, the burden of BC in Iran is expected to be significantly high (20).
The results of this study showed that drug costs accounted for 52.13% of the total costs in 2021 and 59.72% in 2022. Other studies have shown that almost 50% of the total direct costs are spent on drugs (9). A review study by Davari et al. showed that drug cost was the main component of direct medical costs for BC management (20). A study in Jordan indicated that three quarters of direct medical expenses were allocated to medicines (21). Another study in America showed that 44% of all BC costs are related to treatment costs (active treatment, toxicity management and medical follow-up), 31% are related to palliative/supportive care costs, and 21% was related to lost productivity costs (22). A study showed that the total cost of BC in Sweden in 2002 was estimated at 3 billion kroner (1 euro = 9.4 kroner). Direct costs were estimated at 895 million kroner and constituted 30% of the total cost. Indirect costs were estimated at 2.1 billion kroner and accounted for 70% of the total cost (23).
The results of this study showed that radiotherapy costs were the highest among inpatient expenses. Jalali et al.'s study found that the annual cost per patient with BC was 11,979$ in 2021. Direct medical costs accounted for 70.69% of the total costs. Among these direct costs, 39.67% were attributable to radiotherapy and 39.06% to transportation (24). A study in Hungary showed that, of the total treatment costs for BC, 61% was attributable to chemotherapy, 20.9% to radiotherapy, 9.4% to surgery, and 8.6% to mammography (25).
The results of this study showed that the annual cost of BC treatment per person was 305$ in 2021 and 446$ in 2022. Jalali et al.'s study in Fars Province reported that the annual cost per BC patient was 11,979$ in 2021, including both direct and indirect costs (24). According to the study by Broekx et al., the average total cost of BC per patient over six years was 107,456€, with lost productivity accounting for 89% of costs and health care representing 11% (16). According to Roine et al.'s study, the mean total costs were 22,876€ for initial treatment, 3,456€ for rehabilitation, 1,728€ for advanced remission, and 24,320€ for metastatic. Average direct health care costs were 11,798€ for initial treatment, 2,398€ for rehabilitation, 1,147€ for advanced remission, and 13,923€ for metastatic. Average productivity costs ranged from 18% to 39% while indirect costs (productivity and informal) ranged from 31% to 48% of total costs (26). Other studies have shown that the average public health cost of BC was NZ 44,954$ per patient for the three-month period before and five years after cancer diagnosis. The treatment phase accounts for 70% of the cost, while the follow-up phase accounted for the remaining 30%. During the treatment phase, surgery costs accounted for the largest share (35%) of total costs, followed by immunotherapy costs (18%), radiotherapy costs (17%), and diagnostic tests, scans, and biopsy costs. (16%) were placed (15). According to a study in Hungary, the total annual health insurance cost of the National Health Insurance Fund Administration for BC treatment is estimated at 12.09 billion Hungarian Forints (HUF) or 58.09 million dollars (USD) (25).
The results of this study showed that, considering the total population covered by IHIO in 2022, there were 0.86 deaths per 100,000 population. In 2021 this figure was 0.68 deaths per 100,000 population. The study by Taghavi et al. (27) showed that the age-standardized mortality rate of BC in Iran increased from 1.40 to 3.52 per 100,000 population during the years 1995 to 2004. The 2018 burden of disease study showed that the deaths rates for BC in the Philippines (4.36), Thailand (4.35), Colombia (0.75) and Brazil (0.44) had increased significantly.
The 2018 burden of disease study showed significant increases in deaths per 100,000 population in the Philippines (4.36), Thailand (4.36), Colombia (0.75), and Brazil (0.44) (28). According to international and domestic studies, the death rate reported in this study is lower than that in other studies, suggesting that the death registration data in the IHIO may not be accurately reported.
The results of this study showed that the total cost of BC has increased by 88% in one year. A study in South Korea showed that, from 2007 to 2010, the prevalence of treated BC increased from 7.9% to 20.4%. The total socioeconomic costs of BC have increased by approximately 40.7% (29). Jalali's study in Fars province estimated the economic burden of BC in the country at 193,090,952$ USD (24).
The results of this study showed that the prevalence of BC in the population covered by IHIO was 29.16 per 100,000 population in 2021 and 36.88 per 100,000 population in 2022. Another study showed that the prevalence of BC in Iran was 35.08 per 100,000 population in 2020 (30). Breast cancer is the most common cancer among Iranian women, with an incidence rate of 25 per 100,000 population (31).
The results of this study showed that the OOP costs for BC patients in 2021 were 33.72% and in 2022, they were 29.45% of the total direct costs of BC in the population covered by the IHIO. Manzouri et al.'s study showed that OOP costs for BC patients included 32.89% of the total direct medical costs (32). Studies have shown that direct medical OOP costs (i.e., for physician fees) ranged from 300$ to 1,180$ per month during active treatment and were approximately 500$ per month for one year after diagnosis (10). Another study showed that OOP costs are almost two thousand dollars per year, and spend 20% of the income on BC treatment (33). Breast cancer treatment costs cause women to report an average of three economic burden events, including changes in economic lifestyle and income, using savings or borrowing money, and sacrificing plans such as vacations or other events (34).
5.1. Conclusions
The incidence, prevalence and mortality rates of BC in Iran are increasing. The costs associated with BC result in impoverishment and catastrophic expenditures for many families. Addressing the incidence, prevalence, mortality rates, and direct costs associated with BC requires a multifaceted approach that considers clinical data alongside socio-economic factors. Ongoing research is essential for developing strategies that improve early detection methods while ensuring equitable access to treatment across all demographics. Therefore, increasing awareness, implementing effective prevention strategies, and ensuring better access to medical treatment are critical to curbing BC.
5.2. Limitations
The data from this study only include direct treatment costs extracted from the IHIO databases, which do not account for indirect and intangible costs. Therefore, the results should be interpreted in the context of the study’s limitations. Another limitation of the study is that, due to its descriptive nature, causality cannot be reliably attributed to the observed trends. However, possible contributing factors should be considered and further studied. A further limitation was that the time of BC diagnosis was not available in the data, meaning it is possible that patients were at either the beginning of the disease or at the end of the recovery period, leading to estimated costs that may not reflect reality. Additionally, since this study used secondary data, it was not possible to interpret outcomes, exposures, predictors, potential confounders, and effect moderators. Another limitation was that during the two-year period of the study, significant changes occurred in Iran’s health insurance policies, including the establishment of the incurable patients fund, which now covers BC patients. As a result, the establishment of this fund likely influenced patients' OOP costs.
