






1. Background
Larynx cancers are the most common malignancies that are diagnosed in the head and neck. Their incidence rate is so much higher in men than women (1). Timely diagnosis, correct staging, and the right choice of treatment for each individual patient are required for having the successful treatment of the disease. If larynx cancer is treated at an early stage, more than 90% of the patients will live without any symptoms of the disease for up to 5 years. At present, surgical treatment plays a vital role in the treatment of invasive tumors. Although hypopharyngeal cancer is rare, it has a generally poor prognosis and it has one of the most challenging head and neck surgery cases. Supraglottic and subglottic cancers have a difficult prognosis (2-4). The thyroid gland and larynx are anatomically close together. Logically, this anatomical closeness leads to a possible thyroid gland involvement in larynx and hypopharynx cancers (1). The rate of thyroid gland involvement in larynx and hypopharynx cancers has been reported from 5% to 30% in various studies (3-8). There are no clear vascular and lymphatic linkages between the thyroid gland and larynx, and most researchers agree that thyroid involvement in the larynx and hypopharynx cancers could occur only through local invasion (5-9). The major risk factors for thyroid gland involvement in larynx cancers are laryngeal cartilage involvement, extensive subglottic, and transglottic involvement (5-7), but the degree of tumor differentiation effect on thyroid gland involvement and invasion is not clear. Being contiguous or non-contiguous is reported to be associated with the level of tumor differentiation and well-differentiated type of tumors may be more prone to spread and moderately differentiated tumors are less likely contiguous. The presence of tracheostomy before surgery and the involvement of pre-tracheal lymph nodes are also considered as risk factors (7, 9). On the other hand, several studies repudiated the definite risk factors for thyroid gland involvement in larynx and hypopharynx cancers. Several studies have been conducted on the indications and consequences of total thyroidectomy or lobectomy in larynx cancers (10). There are no exact statistics available regarding the consequences of the larynx and hypopharyngeal cancer surgery and the efficiency of thyroidectomy in Iran. There are different recommendations for the thyroidectomy during surgery that vary from total thyroidectomy in all patients to thyroidectomy in case of direct observation of invasion (1-3). In fact, the hormones secreted from the thyroid gland play critical roles in the evolution of different body systems and the differentiation of various cells (11). It has been reported that it could be preferably better to leave a small portion of thyroid tissue for the purpose of protecting the supply of blood to the parathyroid glands in order to prevent hypoparathyroidism, but the remaining thyroid tissue may increase the chance of recurrence (12).
According to another study, it was shown that there was no difference between total thyroidectomy and partial thyroidectomy in terms of cancer mortality or recurrence rates, but on the other hand, there were more severe complications in cases where total thyroidectomy was performed (13). Thus, it has been recommended to perform partial thyroidectomy as the treatment of choice for nonmedullary thyroid involvement (13).
2. Objectives
Considering the above-mentioned information, an appropriate sample size of the study for evaluating the incidence of thyroid gland involvement in different types of larynx and hypopharynx cancers, the efficiency of thyroidectomy and the impact of thyroid involvement on the rate of relapse and survival of patients seems necessary.
3. Methods
This study was performed extensively and reviewed by written medical records of 117 patients admitted with the larynx and/or hypopharyngeal cancer diagnosis in the ear, nose and throat (ENT) and Head and Neck Surgery Department of Loghman Hakim Hospital from 2001 to 2015. Our target population underwent laryngectomy with or without thyroidectomy as a primary treatment of cancer. After considering several parameters, including gender, prevalence, location of the thyroid gland and lymph node involvement, the exact type of malignancy, differentiation stage of the tumor cells, the exact method of thyroidectomy, thyroid function, and its post-surgical cancer recurrence, 117 patients were chosen based on the available data. The informed consent form for using clinical information in their files has been completed by all patients. The required information is extracted from the patient’s clinical records. The information that was analyzed include age, gender, onset and duration of symptoms, clinical stage, location of involvement, grade, preoperative thyroid function, clinical examination results of larynx, thyroid and neck, surgical type, type of thyroidectomy, surgical complications, radiotherapy, postoperative results of thyroid and parathyroid biochemistry tests, smoking history, and overall disease-free and disease-related survival. Patient tracking duration was at least 5 years.
3.1. Statistical Analysis
Statistical tests were performed, using SPSS for Windows software and the results were evaluated for their meaningfulness. For qualitative variables, the Qi-square test was used and for quantitative variables, the t-test was performed.
4. Results
The results of this study showed that in our study, the prevalence of laryngeal cancers was significantly higher in males (92.31%) than females (7.69%) (Figure 1A). The mean age of the disease was 58.47 years. The level of involvement in the anatomical regions of the larynx was the highest in the supraglottic area with 34.19%, the glottic involvement was 26.50%, the transglotitic was 23.93%, and the subglottic area was 15.38% of the patients (Figure 1B).

A, Comparison of the number of laryngeal cancers in males and females, in which the percent of male involvement is much higher than female; B, it shows the extent of involvement in different anatomical regions of the larynx. The highest level of involvement is in the supraglottic area with 34.18% of the patients, 26.49% glottis, 23.95% transglottis, and 15.38% subglottis; C, it shows the extent of the tumor and the extent of the lymph node involvement and metastasis. T2 was 27.35%, T3 61.53%, and T4a 11.11%; D, the rate of lymph node involvement, 74.35% had no lymph nodes involvement, while in the N1 stage of involvement 16.23% and in N2a patients, 8.54 %, and in N2b patients were less than 1%.
TNM STAGING examined the extent of the tumor and the rate of lymph node involvement and metastasis. It showed that T2 was 27.35 %, T3 61.54%, and T4a 11.12% (Figure 1C).
In assessing the rate of lymph node involvement, out of 117 examined patients, 74.35% had no lymph nodes involvement, while this rate was 16.23% in the N1 stage of involvement, 8.54% in N2a patients, and less than 1% in N2b patients (Figure 1D).
Regarding thyroid gland involvement in laryngeal carcinoma in 117 patients, 11.96 % of them had thyroid gland involvement (Figure 2C).
The study of surgical procedures utilized in the treatment of patients with laryngeal carcinoma demonstrated the number of supraglottic surgery procedures in 3 patients, the verticular procedure in 3 subjects, and the total method in 111 patients (Table 1).
| Frequency | Percent | Valid Percent | Cumulative Percent | |
|---|---|---|---|---|
| Valid | ||||
| Supra-glottic | 3 | 2.6 | 2.6 | 2.6 |
| Vertical | 3 | 2.6 | 2.6 | 5.2 |
| Total | 111 | 94.9 | 94.9 | 100 |
| Total | 117 | 100 | 100.0 |
The Surgical Methods Used in the Treatment of Patients with Laryngeal Carcinomaa
Regarding the staging of patients, who have been diagnosed with laryngeal carcinoma, out of 117 patients, 23.1% were in stage 2, 60.7% in stage 3, 13.7% in stage 4a, and 2.6% in stage 4b (Table 2).
| Frequency | Percent | Valid Percent | Cumulative Percent | |
|---|---|---|---|---|
| Valid | ||||
| Stage 2 | 27 | 23.1 | 23.1 | 23.1 |
| Stage 3 | 71 | 60.7 | 60.7 | 83.8 |
| Stage 4a | 16 | 13.7 | 13.7 | 97.5 |
| Stage 4b | 3 | 2.6 | 2.6 | 100 |
| Total | 117 | 100 | 100 |
Staging of 117 Patients, Who Have Been Diagnosed with Laryngeal Carcinomaa
According to the results, the rate of differentiation in cancer cells based on pathologic findings was 20.5% poorly differentiated, 63% distinct, and 16.5% distinct differentiated (Figure 2A).

A, Shows the degree of lymph node involvement based on TNM; B, the extent of cancer cell differentiation based on pathologic findings. According to the results, 24 cases were poorly differentiated, 74 cases were distinct, and 19 cases were distinctly differentiated; C, the rate of thyroid gland involvement in the laryngeal carcinoma, 88.04% had no thyroid involvement, while 11.96 % of them had thyroid gland involvement; D, comparison of thyroid gland involvement with laryngeal carcinoma. Patients in stages 2 and 3 had a progression of the disease to 43% of gland involvement and 57% of them had no thyroid gland involvement; we had 67% thyroid gland involvement in stage 4a, while 33 % of them had no involvement of thyroid. In stage 4b, thyroid gland involvement was 88% and in 12% of them, thyroid gland involvement was not present.
The major risk factors for thyroid gland involvement in larynx cancers are laryngeal cartilage involvement, extensive subglottic, and transglottic involvement. By comparing thyroid gland involvement in the patients with laryngeal carcinoma in stages 2 and 3, 43% of them had thyroid gland involvement and the thyroid gland involvement in stage 4a was 67% and in stage 4b, thyroid gland involvement was 88%, which is significantly higher than those in patients in stages 4a, 2, and 3 (Figure 2B).
A comparison of thyroid gland function before and after surgery showed that 21% of the patients with thyroid gland involvement had hypothyroidism after the surgery (Table 3).
By comparing the relationship between the relapse rates of the tumor with thyroid involvement after the initial surgery, 88.04% of all patients had no thyroid involvement; among them, 1.94% cases had recurrence while out of 11.96% of all patients with thyroid gland involvement, after surgery, 28.5% had recurrence of thyroid gland involvement (Table 4).
The rate of thyroid gland involvement in the pathology report after surgery was 3.41% of the thyroid gland involvement, while 88.04% had no involvement and 8.56% were not evaluated (Figure 3A).

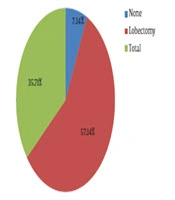
A, The extent of thyroid surgery during laryngeal surgery. Thyroidectomy was performed in 57.14% of the patients with lobectomy, and in 35.71% of them with total thyroidectomy and in 7.14% of cases, no thyroidectomy was performed; B, The rate of thyroid gland involvement in the post-surgical pathology report was 3.41% of the thyroid gland involvement, while 88.03% had no involvement and 8.56% were not evaluated.
In the study of thyroid gland involvement in patients undergoing surgery and subsequent radiotherapy, out of 88.03% of patients, who did not have thyroid gland involvement, 58.25% of the patients did not have radiotherapy, but 41.75% of them had, and out of all patients, who had thyroid involvement, 50% of them had no radiotherapy, and 50% of the cases had radiotherapy (Figure 3B).
5. Discussion
The results of this study showed that the prevalence of laryngeal cancers was significantly higher in males than females and the highest decades of age for the patients were in men, who were mostly in their sixth decade and in women who were mostly in their fifth decade. A comparison of the extent of involvement in different anatomical regions of the larynx showed that the highest level of involvement was in the supraglottic region, which is 34.19%. The involvement of the glottic was seen in 26.50% of the patients, 23.93% of the transglotitic region, and 15.38% in the subglottic area. Previous studies suggested a greater involvement in the supraglottic region, which was consistent with our results (14, 15). In a study, glote had a higher level of involvement (16). Only 16.5% of cancer cells were distinctly differentiated and the degree of differentiation could be a critical factor in the thyroid gland invasion in laryngeal carcinoma.
Regarding thyroid gland involvement in laryngeal carcinoma in all patients, it was shown that 11.96% of them had thyroid gland involvement (Figure 2A). Extensive subglottic and transglottic involvement are the major risk factors for thyroid gland involvement in larynx cancers.
Thyroidectomy was performed during laryngeal carcinoma with lobectomy or total thyroidectomy and in 7.14% of cases, no thyroidectomy was performed. The researchers concluded that routine thyroid resection in larynx cancers should be limited to cases of subglottic or transglobic involvement (3). They recommended thyroidectomy in cases of bilateral tumors, high staging, post-cricoid involvement, and clear radiological evidence (5) or in the event of muscle involvement or in case of subglottic involvement of more than 10 mm (7).
5.1. Conclusions
The prevalence of laryngeal cancers was significantly higher in males than females; this type of cancer is more common in men because far fewer women than men use tobacco. Based on our findings, the rate of thyroid gland involvement in the pathology report after surgery was approximately 3.41% of the thyroid gland involvement, which is low. We concluded that thyroidectomy is a very efficient way, but it should be limited to cases of subglottic or transglottic involvement or in cases of bilateral tumors, high staging, post-cricoid involvement, and clear radiological evidence or in the event of muscle involvement.
