
1. Background
Pediatric cancer is one of the most disrupting factors in families. When a child is diagnosed, every person in the family goes to be upset (1). Currently, more than 50% of pediatric cancer survivors live longer than 5 years after diagnosis (2). The quality of communication in the family is vital about pediatric cancer survivors because of an increase in life expectancy.
In most of the situation, mothers are the main caregivers of sick children. When mothers experience helplessness (because of cancer diagnosis), the adjustment of the child with cancer and consequently throughout the disease are profoundly affected. Helplessness is typically defined as distress tolerance. High levels of distress tolerance explain less helplessness (3). Distress tolerance has been defined as individual differences in resistance to emotional distress and stress vulnerability (4).
Distress tolerance primarily focuses on the perceived or actual behavioral capacity to tolerate annoying or threatening stimuli. In the literature, distress tolerance is formulated in two lines: firstly, this concept refers to a cognitive capacity instead of emotional disruption and secondly, distress tolerance is focused on every effort (behavioral and physiological reaction) against aversive situations (5). This study followed the first one. Leyro et al. (6) point out to distress tolerance as a network risk and protection process such as avoidance coping, anxiety sensitivity, and emotional regulation. According to the theory, with the increasing environmental demands, individuals depending on their coping resources will experience emotional disruption. If they cannot overcome these demands, emotional disruption (experience of anxiety, depression, and anger simultaneously) appears. Emotional disruption is presented in physical, cognitive, emotional and behavioral dimensions. In this research, the focus was on the behavioral dimension. It is assumed that the mother’s emotional disturbance affects her child-rearing behavior. Also, the attachment behavior of the child is affected by the disturbance of the mother.
Mothers often experience anxiety and distress when their child is diagnosed with an illness. These symptoms occur together because of high caregiver burden. Parent’s experiences about their children suffering, distance from family due to prolonged hospitalization, concern about family members who feel abandoned, financial problems related to cancer treatment, disease burden, and neglected needs can be very frustrating sometimes. Eventually, too much stress over a long time can cause burnout, which can affect mothers’ physical and psychological function (4). The hopelessness levels appear in a range of low to very debilitating among mothers because there are obvious differences in coping strategies and social support (7). Children with cancer are dependent on their mother’s attention and most parents are extremely worried about their children. It can lead to conflict and mothers are forced to maintain sustainability in upbringing (8). In this research, we tried to find out whether the parenting style may be affected by the mother’s distress and helplessness.
Parenting styles are defined as parent-child interaction. Baumrind (9) identified 3 initial parenting styles, including authoritative parenting, authoritarian parenting, and permissive parenting. The components of authoritative parenting are warmth, firmness, and granting autonomy. This parenting style is determined by low demandingness and high responsiveness (9). Little research has been done on the effect of parenting styles in childhood cancer. The evidence suggests that parents of children with cancer exert too much control and have low expectations (10).
Previous studies confirmed the importance of early bonding on personality development, interpersonal relationships, coping strategies, social adjustment, and mental health (11). Failure to manage emotional disruption in mothers, when her child suffers from cancer, can have negative consequences in the nurture and child’s behaviors. The study of distress tolerance in mothers is necessary because of the effect on raring children with cancer and determined effective communication in the future.
2. Objectives
The aim of this study was to determine the role of distress tolerance in mothers of children with cancer for predicting her parenting style and child’s attachment behaviors.
3. Methods
3.1. Design and Study Subjects
In this cross sectional study, the predictive role of an independent variable on dependent variables has been investigated. A total of 130 mothers, who had children with leukemia and brain tumors (3 - 12 years old), in “Pediatric Oncology Mahak” participated in the present study. The available sampling method was used based on the inclusion/exclusion criteria. The inclusion criteria included (1) age range between 3 and 12 years; (2) at least 6 months after the cancer diagnosis; and (3) ability to read and write. The exclusion criteria included (1) a history of psychological problems; (2) the lack of tendency to participation, and (3) child’s death. The ethics code of this article was IR.TUMS.VCR.REC.1397.807 from Tehran University of Medical Sciences. Before the research, the consent forms were completed by parents. All participants were aware of research goals and the right to withdraw from the research at any time; they were also assured of non-disclosure of their identity. All participants were asked if they wanted to know the test results. They were informed about the confidentiality of the research. Their questions were answered in the whole of the process of research. In the end, a workshop was held for free on “parenting in the context of children with cancer” for the participants. Finally, they received the required information and some recommendations about emotion regulation strategies by telegram. Multiple regression analysis by SPSS 24 was applied for data analysis.
3.2. Instruments
3.2.1. Distress Tolerance Scale
Distress tolerance scale (DTS) is a self-report instrument developed by Simons and Gaher (12). The DTS was designed to assess an individual’s ability to tolerate distress, an individual’s appraisal of a distressing situation, an individual’s attention to negative emotions, and an individual’s ability to regulate emotions. Items are rated on a 5-point Likert scale; higher scores indicate a greater level of distress tolerance. This scale includes 15 items, which comprise 4 subscales, including (1) tolerance, (2) appraisal, (3) absorption, and (4) regulation. The Cronbach’s alpha coefficients of the mentioned subscales and the whole scale were 0.72, 0.82, 0.78, 0.70, and 0.82, respectively. The intraclass correlation coefficient was 0.61 after 6 months. The DTS showed good criterion validity and convergent validity.
3.2.2. The Kinship Center Attachment Questionnaire
The Kinship Center Attachment questionnaire (KCAQ) was designed by Kappenberg and Halpern (13). The KCAQ is a 20-item questionnaire, which is suited for children younger than 6 years old. Its purpose is to measure a child’s attachment dimensions (positive adjustment/development, negative behavior, emotional reactivity, and distancing from caregiver support).
3.2.3. Parenting Style Inventory
The parenting style inventory is based on Baumrind’s theory, which offers 3 styles of parental authority, including authoritative, authoritarian, and permissive. Each style refers to strategies that parents use in child rearing. The original form of this questionnaire was developed by Baumrind (14); it consisted of 30 Likert type items, 10 of which are related to authoritative, 10 are related to authoritarian, and 10 are related to permissive prototype. The reliability of this questionnaire through the test-retest method was 0.81 for the permissive parenting style, 0.85 for authoritarian parenting style, and 0.92 for the logical authority style of fathers.
4. Results
In this study, problem statements were emotional disruption of mothers on how to predict parenting styles (permissive, authoritarian, and logical authority) and attachment behaviors in children with cancer (positive adjustment, emotional reactivity, negative behavior, and distancing from caregiver support).
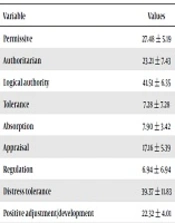
The mean ± SD age of mothers was 39.33 ± 4.93 years. Children with cancer aged between 3 and 12 years. Most mothers had an average level of education (54.3%). Table 1 shows the mean and SD of variables.
Table 1.The Mean and Standard Deviation of the Research Variablesa
| Variable | Values |
|---|---|
| Permissive | 27.48 ± 5.19 |
| Authoritarian | 23.21 ± 7.43 |
| Logical authority | 41.51 ± 6.35 |
| Tolerance | 7.28 ± 7.28 |
| Absorption | 7.90 ± 3.42 |
| Appraisal | 17.16 ± 5.39 |
| Regulation | 6.94 ± 6.94 |
| Distress tolerance | 39.37 ± 11.83 |
| Positive adjustment/development | 22.32 ± 4.01 |
| Emotional reactivity | 11.26 ± 2.85 |
| Negative behavior | 9.93 ± 2.60 |
| Distancing from caregiver support | 7.59 ± 2.87 |
| The total score of attachment | 51.40 ± 5.99 |
| Mother’s age | 33.29 ± 4.93 |
| Child’s age | 6.78 ± 4.03 |
| Mother’s education, % | |
| Under-graduation | 14 |
| Graduation | 6 |
| Post-graduation | 18 |
| Mother’s marital status, % | |
| Married | 73 |
| Divorce or Widow | 27 |
aValues are expressed as mean ± SD.
A correlation matrix of parenting styles and distress tolerance was calculated. Linear relationships between these two variables are presented in the following Table 2.
Table 2.Correlation Coefficients Between Components of Parenting Styles, Attachment Behavior, and Distress Tolerance
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Permissive | 1 | ||||||||||
| Authoritarian | -0.67a | 1 | |||||||||
| Logical authority | -0.18 | -0.49a | 1 | ||||||||
| Tolerance | -0.21 | -0.46a | 0.43a | 1 | |||||||
| Absorption | -0.12 | -0.39b | 0.34b | 0.77a | 1 | ||||||
| Appraisal | -0.13 | -0.54a | 0.53a | 0.83a | 0.75 | 1 | |||||
| Regulation | -0.061 | -0.18 | 0.69a | 0.24 | 0.083 | 0.11 | 1 | ||||
| Positive adjustment/development | -0.37b | -0.46a | 0.49a | 0.53a | 0.25 | 0.31 | 0.37b | 1 | |||
| Emotional reactivity | 0.33b | -0.51a | -0.61a | 0.65a | 0.21 | -0.36b | 0.27 | -0.16 | 1 | ||
| negative behavior | 0.28 | -0.63a | -0.32b | -0.54a | 0.23 | -0.37b | 0.14 | -0.11 | 0.17 | 1 | |
| distancing from caregiver support | 0.11 | -0.52a | -.41a | 0.13 | 0.26 | 0.22 | 0.16 | -0.21 | 0.24 | 0.28 | 1 |
aCorrelation is significant at the 0.001 level.
bCorrelation is significant at the 0.05 level.
The research hypothesis was to predict parenting styles and attachment behaviors of children with cancer based on the mother’s distress tolerance. Simultaneous multiple regression analysis was used to analyze data. The results are summarized in Table 3.
Table 3.Simultaneous Multiple Regression Analysis for the Prediction of Parenting Styles and Attachment Behaviors Based on Distress Tolerance in Mothers of Children with Cancer
| Criterion variable | β | B | SE | R | R2 | T | P |
|---|---|---|---|---|---|---|---|
| Parenting styles (mothers) | |||||||
| Permissive | -0.17 | 0.082 | 0.023 | 0.24 | 0.057 | 1.97 | 0.33 |
| Authoritarian | -0.26 | 0.064 | 0.027 | 0.39 | 0.152 | 2.91 | 0.05 |
| Logical authority | 0.29 | 0.091 | 0.031 | 0.43 | 0.184 | 3.46 | 0.001 |
| Constant | - | 13.13 | 2.054 | - | - | 6.47 | 0.05 |
| Attachment behaviors (children with cancer) | |||||||
| Positive adjustment/development | 0.43 | 0.12 | 0.066 | 0.63 | 0.29 | 2.34 | 0.001 |
| Emotional reactivity | -0.54 | 0.10 | 0.018 | 0.54 | 0.19 | 2.54 | 0.001 |
| Negative behavior | -0.24 | 0.075 | 0.051 | 0.51 | 0.16 | 3.16 | 0.001 |
| Distancing from caregiver support | -0.21 | 0.016 | 0.21 | 0.11 | 0.012 | 0.92 | 0.33 |
| Constant | - | 14.12 | 2.09 | - | - | 7.03 | 0.001 |
According to Table 3, the mother’s distress tolerance explains parenting styles. Mothers with low distress tolerance were more likely to use authoritarian style (T = 2.92, P < 0.05). Mothers with high distress tolerance were more likely to use the logical authority style (T = 3.46, P < 0.001). In other words, 15% of authoritarian style is predicted by low distress tolerance and 18% of authoritative style is predicted by high distress tolerance. Based on the beta standardized coefficient, a one-standard deviation decrease in distress tolerance (due to a negative score) increased the authoritarian score up to 0.26 and high distress tolerance increased authoritative style up to 0.29.
In addition, mothers’ distress tolerance predicted some attachment behaviors such as positive adjustment/development (T = 2.34, P < 0.001), emotional reactivity (T = 2.54, P < 0.001), and negative behaviors (T = 3.16, P < 0.001) in children with cancer. Mothers’ distress tolerance predicted 29% of positive adjustment/development, 19% of emotional reactivity, and 16% of negative behaviors in children with cancer. As shown in Table 3, a one-standard deviation increase in distress tolerance decreased positive adjustment/development, emotional reactivity, and negative behaviors score up to 0.43, 0.54, and 0.24, respectively.
5. Discussion
The results showed that the low level of the mother’s distress tolerance predicted authoritarian style and the high level of the mother’s distress tolerance predicted an authoritative style. The permissive style was not predicted by the mother’s distress tolerance.
Sherman (15) investigated cancer survivors, who indicated that overprotection, over-controlling, and overparenting were extremely high in parental behavior. This finding is congruent with our research. Authoritarian style is a part of overparenting, which comprises two related aspects of over-controlling and overprotection (16). Furthermore, previous studies have found that over-controlling parents are more prone to depression and overprotective parents are more prone to anxiety (17). Bahrami et al. (18) showed the relationship between parental emotions and interacting with children and upbringing in mothers of preschool children. They emphasized that the ability to emotional regulation plays an important role in choosing parenting styles. In the present study, this relationship was confirmed in mothers with cancer.
Groh et al. (19) showed that when the heart rate of the mother is high or low, it affects children’s attachment behaviors. When the heart rate of the mother exceeds the normal rate, it could anticipate avoidance behaviors in the child.
Vrijmoet-Wiersma et al. (20) showed that parents of children, who survived cancer most frequently use overprotective style. This study was conducted on cancer survivors, who scored higher or lower than the cut-off point in helplessness scale (anxiety and depression). They also revealed that the overprotective parenting style was more successful in children, who scored high in helplessness. These findings are congruent with our research and suggested that mothers with emotional problems tend to impose severe authority on their children in order to reduce their tension. This negative feedback occurs as compensatory responses. Mothers who are emotionally disturbed have difficulties with behavior regulation and problem-solving skills, such as extreme parental monitoring, autocratic decision-making, and punishment. Over-controlling mothers create barriers to achieving goals, decision-making, and taking advantage of opportunities (21). Authoritarian style is an attempt to control symptoms. It is an undeniable fact that parents have little control over conditions in a hospital environment. As a conflicting situation, parents with low levels of distress tolerance may try to control their children’s lives by overparenting.
Based on the obtained results, there is an inverse correlation between the permissive parenting style and distress tolerance, but it is not statistically significant. The findings of this study showed that the permissive style was not predicted by mothers’ distress tolerance. Therefore, it can be concluded that there is no significant correlation between the mother’s helplessness and the permissive parenting style. Also, any remarkable result was not found in previous studies.
The present research showed that a high level of distress tolerance positively and significantly predicted the authoritative parenting style. In other words, if mothers experience less helplessness, they will improve their ability to use an authoritative style. This finding is in line with the Dahlquist’s study (19), which suggested authoritative mothers reveal a higher level of self-regulation. Self-regulation is likely a key factor of authoritative style. High levels of self-regulation strategies in mothers of children with cancer cause a balance between kindness and control. Self-regulation and emotion regulation skills can empower mothers to manage difficult conditions.
Studies have shown that mothers of children with cancer are authoritative in child rearing when they use two effective coping strategies, namely the challenges with problems and interactions with others (11). Research showed that cancer survivors, whose mothers used overparenting style, were more anxious, which is caused by ineffective coping strategies (22). It can be concluded that controlling mothers not only have limited resources to deal with childhood disease challenges but also limit their children’s independence and confidence in how to confront stress in the future.
The high level of mother’s distress tolerance predicted positive adjustment/development and the low level of mother’s distress tolerance predicted emotional response and the negative behavior of a child with cancer, but it did not predict distancing from caregiver support.
This finding is consistent with the findings of Mellblom et al. (23). They suggested that parents, who experience negative conflicts and are extremely disturbed, can affect their child’s behavioral problems. From their viewpoint, conflict can reduce the parent’s ability to tolerate emotions and this leads to behavioral dysregulation in children. This research is based on maternal reporting and has not studied the father’s experiences.
5.1. Conclusions
Distress tolerance in mothers is a reflection of self-regulation. If mothers try to calm themselves down, they will not use over-controlling and overprotective parenting styles. Furthermore, this ability can modify attachment behaviors in children.