1. Background
Breast cancer is the most frequent diagnosed visceral cancer and is the second cause of death due to cancer among Iranian women based on the cancer registry system (1).
There are 13400 new cases of breast cancer with an incidence rate of 32 in 100000 in Iranian women annually. In Iran, breast cancer is diagnosed 10 years earlier than most developed countries, therefore, we had major health and treatment problems of burden of this disease (2).
For more than 70 years, radical mastectomy and modified radical mastectomy (MRM) were known as a standard surgical treatment in the breast cancer. After that, breast conserving surgery (BCS) with adjuvant radiotherapy was developed as the standard treatment in early-stage breast cancer from 30 years ago.
2. Objectives
In this historical cohort study, we compared local recurrence, distant recurrence, 5-year DFS, and 5-year OS in patients with breast cancer who were treated by BCT or MRM at Cancer Research Center of the Shahid Beheshti University of Medical Sciences between September 2002 and December 2014.
3. Methods
In this historical cohort study, a consecutive series of 6000 patients with breast cancer were treated by BCT or MRM. Data were extracted from the database of Cancer Research Center, Shahid Beheshti University of Medical Sciences, a referral breast clinic in Tehran, Iran. Our sampling method was a time-stratified 1:1 approach for selecting 1310 women who were eligible for our study. BCS was followed by adjuvant radiotherapy to the whole breast with or without boost was done in 655 cases and MRM with or without adjuvant radiotherapy was determined in 655 cases between September 2002 and December 2014.
All 1310 patients were matched based on a time-stratified 1:1 approach with stage I to III without distant metastasis and were matched based on 10 baseline variables (age at diagnosis, stage of tumor, tumor histology, tumor grade, number of positive nodes, pathologic tumor size, type of chemotherapy ER, PR and HER2 status) that are believed for having a significant role with distant recurrence, LR, DFS and OS, based on previous studies. The exclusion criteria were: patients with breast cancer who did not have acceptable follow up after initial diagnosis, patients with metastatic, and patients without pathologic diagnosis. The inclusion criteria were: patients with breast cancer with stage I to III who had acceptable follow up after initial diagnosis and had all 10 baseline variables (age at diagnosis, stage of tumor, tumor histology, tumor grade, number of positive nodes, pathologic tumor size, type of chemotherapy ER, PR and HER2 status).
All patients with breast cancer had pathologic diagnosis which was performed by biopsy or surgery of the primary breast tumor. In the BCT group, resection of the primary tumor with an adequate negative margin of axillary lymph node dissection (ALND) or sentinel lymph node biopsy (SLNB) was performed and all patients were followed by adjuvant radiotherapy to the whole breast with or without boost to the primary site of tumor. In the MRM group, the surgical procedure included resection of the whole breast with an adequate surgical negative margin with ALND were followed by adjuvant radiotherapy to the chest wall with or without irradiation to the regional lymph nodes.
After all treatments were over, every breast cancer patient was visited and examined every 3 to 6 months for five years and yearly afterward. The patients underwent mammography annually. Breast cancer patients who did not have acceptable follow up after initial diagnosis were excluded from the study. In the case of clinical symptoms or signs of any recurrences, patients underwent imaging or biopsy to identify any recurrences.
Until April 2015, breast cancer patients had a follow-up period of 41 months. As the time interval between initial diagnosis and local or distant recurrence was defined as DFS and the time interval between initial diagnosis and death was defined as OS.
In the act provided by Shahid Beheshti University of Medical Sciences, the ethical regulations dictated were approved to review of the medical records for the purposes of our study (ethical code: IR.SBMU.MSP.REC.1396.358).
Differences in all variables on local and distant recurrence and death were evaluated and analyzed by the chi-square test. DFS and OS rates were estimated by Kaplan- Meier analysis and compared by the Log-rank test. P value < 0.05 was considered significant. All statistical analyses were performed using the IBM SPSS 22.0.
4. Results
In BCT group and MRM group, the median age was 48.11 years (range 22 - 84 years) and 48.64 years (range 17 - 85 years), respectively. In the both groups 68 patients (10.4%) had age ≤ 35 years and 587 patients (89.6%) had age > 35 years.
Total of 563 patients (86%) had pathologic report of infiltrating ductal carcinoma, 79 patients (12%) had other pathology except infiltrating ductal carcinoma and 13 patients (2%) had unknown pathology reports in both groups. Fifty-two cases (8%) had well-differentiated grade, 354 patients (54%) had moderately differentiated grade, 184 patients (28%) had poorly differentiated grade, and in both groups the grade of 65 cases (10%) was unknown.
In group A and group B there were 197 patients (30%) with zero involved lymph nodes, 268 patients (41%) with ≤ 3 pathologic positive lymph nodes, 144 patients (22%) with ≥ 4 pathologic positive lymph nodes, and 46 patients (7%) with unknown pathologic lymph nodes.
In group A and group B there were 105 cases (16%) with tumor size > 5 centimeters (cm), 452 cases (69%) with tumor size ≤ 5cm, and 98 cases (15%) with unknown tumor size.
Based on tumor stage, in group A and B, 59 cases (9%) had stage I, 321 cases (49%) had stage II, 216 cases (33%) had stage III, and 59 patients (9%) were with unknown stage.
In group A and B, 219 patients (33%) received NAC and 437 patients (67%) received AC.
For ER status in group A and group B there were 426 (65%) patients with ER positive, 203 cases (31%) with ER negative and 26 (4%) cases were with unknown ER receptor status.
For PR status in group A and group B there were 360 (55%), 236 (36%), and 59 (9%) patients with PR positive, PR negative, and unknown PR receptor status, respectively.
In BCT group and MRM group there were 151 (23%), 439 (67%), and 65 patients (10%) with HER2 positive, HER2 negative, and unknown HER2 status, respectively.
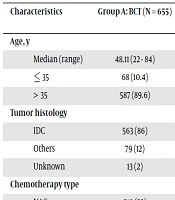
Table 1 summarizes baseline characteristics and the clinical-pathological features of 1310 adult patients with breast cancer (655 patients in each group).
Table 1.
Baseline Characteristics and the Clinical-Pathological Features of 1310 Adult Patients with Breast Cancera
| Characteristics | Group A: BCT (N = 655) | Group B: MRM (N = 655) |
|---|---|---|
| Age, y | ||
| Median (range) | 48.11 (22 - 84) | 48.64 (17 - 85) |
| ≤ 35 | 68 (10.4) | 68 (10.4) |
| > 35 | 587 (89.6) | 587 (89.6) |
| Tumor histology | ||
| IDC | 563 (86) | 563 (86) |
| Others | 79 (12) | 79 (12) |
| Unknown | 13 (2) | 13 (2) |
| Chemotherapy type | ||
| NAC | 219 (33) | 219 (33) |
| AC | 437 (67 | 437 (67) |
| Tumor size, cm | ||
| ≤ 5 | 452 (69) | 452 (69) |
| > 5 | 105 (16) | 105 (16) |
| Unknown | 98 (15) | 98 (15) |
| Nodal status | ||
| Node-negative | 197 (30) | 197 (30) |
| 1 - 3 positive nodes | 268 (41) | 268 (41) |
| ≥ 4 positive nodes | 144 (22) | 144 (22) |
| Unknown | 46 (7) | 46 (7) |
| Tumor stage | ||
| I | 59 (9) | 59 (9) |
| II | 321 (49) | 321 (49) |
| III | 216 (33) | 216 (33) |
| Unknown | 59 (9) | 59 (9) |
| Tumor grade | ||
| Well differentiated | 52 (8) | 52 (8) |
| Moderately differentiated | 354 (54) | 354 (54) |
| Poorly differentiated | 184 (28) | 184 (28) |
| Unknown | 65 (10) | 65 (10) |
| Receptor status | ||
| ER positive | 426 (65) | 426 (65) |
| ER negative | 203 (31) | 203 (31) |
| Unknown | 26 (4) | 26 (4) |
| PR positive | 360 (55) | 360 (55) |
| PR negative | 236 (36) | 236 (36) |
| Unknown | 59 (9) | 59 (9) |
| HER2 positive | 151 (23) | 151 (23) |
| HER2 negative | 439 (67) | 439 (67) |
| Unknown | 65 (10) | 65 (10) |
Abbreviations: AC, adjuvant chemotherapy; BCT, breast-conserving therapy; MRM, modified radical mastectomy; NAC, neo-adjuvant chemotherapy
aValues are expressed as No. (%) unless otherwise indicated.
Since December 2014, a median follow-up time was 71 months (range 48 - 192 months), 11 cases (1.68%) of local recurrence were shown in the BCT group and seven patients (1.07%) of local recurrence were shown in MRM group during the five years of follow up. Thus the 5-year local recurrence- free survivals were 98.32% in BCT group and 98.93% in MRM group. There was not any significant local recurrence differences between BCT group and MRM group based on the log-rank test 5-year local recurrence analysis, (P = 0.173, RR = 1.13, 95% CI = 1.05 - 1.22) (Table 2). Then patients in BCT group did not show more local recurrence than MRM group.
Table 2.
Comparison of Local Recurrence and Distant Recurrence During 5-Years, Between Group A and Group B.
| Group A | Group B | |
|---|---|---|
| Included patients, N | 655 | 655 |
| Local recurrence during 5-years, No. (%) | 11 (1.68) | 7 (1.07) |
| RR 95%CI | 1.13 (1.05 - 1.22) | |
| P value (log-rank test) | 0.173 | |
| 5-years local recurrence-free survival, No. (%) | 644 (98.32) | 648 (98.93) |
| RR 95%CI | 1.13 (1.05 - 1.22) | |
| P value (log-rank test) | 0.173 | |
| Distant recurrence during 5-years, No. (%) | 68 (10.38) | 121 (18.47) |
| RR 95%CI | 1.78 (1.58 - 1.98) | |
| P value (log-rank test) | < 0.001 | |
| 5-years distant disease-free survival, No. (%) | 587 (89.62) | 534 (81.53) |
| RR 95%CI | 1.78 (1.58 - 1.98) | |
| P value (log-rank test) | < 0.001 | |
Abbreviations: CI, confidence interval; RR, relative risk
In BCT group, 68 patients (10.38%) were diagnosed with distant metastasis during of the 5-year follow up and 121 patients (18.47%) had distant recurrence in MRM group. Thus the 5-year- distant recurrence free survival were 89.62% in BCT group and 81.53% in MRM group. We found a significant difference between two groups as distant recurrence free survival based on log-rank test analysis (P < 0.001, RR = 1.78, 95% CI = 1.58 - 1.98) (Table 3).
Table 3.
Comparison of the Five Years Disease Free Survival (DFS) Rate and Five Years Overall Survival Rate (OS), Between Patients with Breast Cancer in Group A and Group B
| Group A | Group B | |
|---|---|---|
| Included patients, N | 655 | 655 |
| 5-year DFS Rate, % | 87.94 | 80.46 |
| P value (log-rank test) | < 0.001 | |
| 5-year OS Rate, % | 89.31 | 83.02 |
| P value (log-rank test) | 0.041 | |
Abbreviations: DFS, disease free survival; OS, overall survival
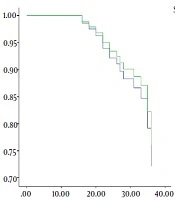
The five-year DFS rate was 87.94% and 80.46% in BCT and MRM groups, respectively. We observed a significant difference between two groups as the five-year DFS based on the log-rank test analysis (P < 0.001) (Table 3). Then patients in BCT group showed better DFS than MRM group.
In BCT and MRM groups, the five-year OS rate was 89.31% and 83.02%, respectively. We showed a significant difference between two groups as the five-year OS based on log-rank test analysis (P = 0.041) (Table 3). Then patients in BCT group showed better OS than MRM group.
5. Discussion
The results of this study showed that 5-year DFS and 5-year OS rates in BCT group were better than the MRM group. In the current study, which has been conducted at Cancer Research Center of the Shahid Beheshti University of Medical Sciences, we compared local recurrence, distant recurrence, 5-year DFS, and 5-year OS in 1310 matched patients who underwent MRM or BCT. To the best of our knowledge, it is the greatest series in Iran.
There are seven prospective randomized clinical trials which have found that BCT is equivalent to MRM as OS in breast cancer patients, in spite of a higher rate of LR (3-9). In many Western countries, BCT has been performed in clinical practice for more than 25 years. In Iran, there are lower rates of BCT in comparison to western countries that might relate to some factors such as socioeconomic factors and concern over the increased risk of LR. In addition, distant recurrence appears to have been related to both breast cancer patients and their physicians.
We minimized the selection bias between BCT and MRM groups and all data were matched and analyzed according to 10 baseline variables (age at diagnosis, stage of tumor, tumor histology, tumor grade, number of positive nodes, pathologic tumor size, type of chemotherapy, ER, PR and HER2 status) that are believed for having a significant role with distant recurrence, LR, DFS, and OS based on previous studies.
In the BCT group and MRM group, the median age was 48.11 and 48.64 years old, respectively. In both groups, 68 cases (10.4%) had age ≤ 35 years and 587 cases (89.6%) had age > 35 years, and there were no differences in the frequency of patients ≤ 35 years. These findings indicate that age is not an important factor to predict LR and distant metastases in both groups. This result is consistent with most studies (8, 9).
Wang et al. (10, 11) showed the 6-year LR-free survival (LRFS) rates was 98.2% in the BCT group and 98.7% in the MRM group (P = 0.182). These findings were consistent with our study which showed that the 5-year LRFS was 98.32% in the BCT group and 98.93% in the MRM group (P = 0.173). They also showed the 6-year DFS rates in BCT and MRM groups was 91.3% and 86.3% (P < 0.001) that were consistent with our study, which found that the 5-year DFS rates were 87.94% in the BCT group and 80.46% in the MRM group (P < 0.001). They could not show any comparison as overall survival between two groups, but in this study, we showed that the 5-year OS was 89.31% in group A and 83.02% in group B (P = 0.041).
Veronesi et al. (12) found higher risk of LR, distant recurrence, and breast cancer mortality associated with BCS than MRM. These findings were inconsistent with our study which showed that BCT group did not have more local recurrence, distant recurrence, and breast cancer mortality than the MRM group.
Hwang et al. (13) demonstrated that in stage I and II of breast cancer, the 5-year PFS and the 5-year OS were worse in the MRM group than BCT group. These findings were consistent with this study, which found that the 5-year PFS and the 5-year OS in the BCT group were better than MRM group. In this study we compared stage I, II, and III and found the same results.
Yuan et al. (14) showed that BCT patients had worse LR , inferior 5-year DFS, and inferior 5-year OS than MRM cases as stage I, II, and III of breast cancer; in the present study, We showed 5-year DFS and 5-year OS in both groups were compatible, that were inconsistent with Yuan et al.’s study.
In another study carried out by van Dongen et al. (15) in July of 2000 showed the 10-year local recurrence rates were 20% in the BCT patients and 12% in the MRM cases (P = 0.01). These findings were inconsistent with our study which that found the 5-year LR rates were 1.68% in the BCT cases and 1.07% in the MRM patients (P = 0.173). They also showed that the 10-year OS rates in BCT and MRM groups were 66% and 65% (P = 0.011), respectively. These findings were consistent with our study. Based on this study the 5-year OS rates were 89.31% in group A and 83.02% in group B (P < 0.001).
Agarwal et al. (16) demonstrated the 5-year OS of BCT cases, a mastectomy alone cases, or a mastectomy with adjuvant radiation therapy were 97%, 94%, and 90%, respectively (P < 0.001). These findings were consistent with our study that the 5-year DFS was 87.94% in the BCT cases and 80.46% in the MRM cases (P < 0.001), and the 5-year OS was 89.31% in the BCT patients and 83.02% in the MRM cases (P = 0.041).They also found the 10-year breast cancer-specific survival rates in the BCT group, in mastectomy alone group, and in mastectomy with radiation therapy group were 94%, 90%, and 83%, respectively (P < 0.001). In the present study, there were not any findings about 10-year PFS and 10-year OS.
The limitations of this study included the missing data of some patients’ information and the short follow up period.
5.1. Conclusions
The findings of this study showed that 5-year DFS and 5-year OS rates in BCT group were better than the MRM group. The local recurrence rate in the BCT group was more than MRM group, but increased LR was not associated with worse DFS and OS. However, because of short follow up period, this study cannot prove that BCT is definitely superior to MRM.