






1. Background
Due to the young age structure of the population in Iran and more vulnerability to risky behaviors among adolescents and young people, the health of this group is one of the most important issues (1). The adolescent period is a dynamic one with possible repercussions related to making logical decisions during this period (2). Adolescents usually tend to test their limits and experience new behaviors; since they regard themselves as immortal, they worry less about the long-term implications of engaging in dangerous behaviors, particularly sexually risky behaviors (3). At the International Conference on Population and Development held in 1994, access to educational information and counseling services was mandated for everyone at a suitable age to help safeguard their sexual and reproductive health (4). The United Nations Educational, Scientific and Cultural Organization (UNESCO) guidelines suggest that parents and families should present sexuality education to adolescents; however, no specified content or teaching methods have been proposed. At the same time, parents are motivated to be more open and to communicate with their children peacefully and honestly (5).
Sexuality education helps people think more deeply about these issues, become more sensitive and conscious in interpersonal relations, and have more logical and responsible sexual relations. Sexuality education is associated not only with the cognitive (awareness) domain but also with both affective (feelings, values, and attitudes) and behavioral (communication and decision-making skills) domains (6). The common viewpoint in many communities is that adolescents in the transition from childhood to adulthood should not engage in sexual activity; however, it is a fact that many people in the world begin sexual activity at a young age, with the first sexual activity experienced, on average, by teenagers below the age of 14 years (1). Thus, adolescents face many questions about sexuality and its relevant emotional and psychological reactions, which often go unanswered in many societies due to cultural reasons (7). In many countries, there is serious resistance against providing sexuality education for adolescents because of the misunderstanding of nature, purpose, and effect of such training, thus denying adolescents’ access to such training (8). On the other hand, the spread of mass media and the increasing speed of information flow in recent years has provided fertile ground for the transmission of false sexual information (9). Additionally, social and cultural changes in Iran, some of which are linked to a greater incidence of premarital sexual relations, as well as harmful social conditions and serious health problems, including an increase in cases of sexually transmitted diseases, particularly acquired immunodeficiency syndrome (AIDS), have made sexuality education an essential matter of public health (10).
In Iran, as in many other communities, adults -as parents, those involved in planning and implementation of health services, and decision-makers about the reproductive health services and information for adolescents- affect the nature and type of information and services that adolescents receive. Most people are still not convinced of the need for sexuality education for adolescents and consequently prevent this type of education. Furthermore, many people do not have the skills necessary to offer this type of education (10). Teachers and parents are afraid that sexuality education will result in sexual experiences among adolescents; therefore, they omit and ignore it. As a result, peer-aged friends are the main source of information associated with sexuality, with families ranked sixth in this regard (11, 12). Studies have revealed that a lack of education not only does not prevent teenagers from engaging in sexual relations but also leads to the formation of misconceptions and misinformation (13). Sexuality education is of great importance for young women since they, as future mothers, play a key role in their own and the community’s health. Family, as the first social institution, plays a critical role in training and transferring information to children and adolescents (9).
Health behaviors, including sexual relations, in most adolescent girls are learned from their mothers. However, studies have shown that most parents are not aware of this issue and even hold negative attitudes towards providing sexuality education for adolescents (7, 14). Some students have mentioned that they do not talk with their parents about sexuality because of their parents’ lack of awareness and communication skills (15). On the other hand, although some parents would like to provide their children with information about self-control, contraceptive methods, and sexually transmitted diseases, they have difficulty communicating with them (4).
Given the key role of parents as critical individuals in providing sexuality education for children and adolescents, the design and implementation of programs to empower families is a necessity (16). Considering the lack of a comprehensive and systematic program on sexuality education for adolescents and young adults, empowering parents, especially mothers, and reconfiguring social attitudes in this area is of paramount importance (13).
2. Objectives
In the current study, a training program was designed, implemented, and evaluated to improve mothers’ skills in communicating effectively with their daughters to present sexuality education.
3. Materials and Methods
This field trial was conducted among 140 mothers with 12- to 18-year-old adolescent girls in Mahshahr, Southern Iran, during the second half of 2014. No control group was used. A multi-stratified sampling method was applied along with convenience sampling. Lower and upper secondary high schools and public and private high schools were considered as stratum variables. Selecting subjects was based on a list of girls’ high schools in Mahshahr, including 24 high schools at the lower secondary level (19 public and five private) and 28 high schools at the upper secondary level (17 public and 11 private) with total populations of 3,554 and 5,545 students in public and private schools, respectively. From these schools, one lower secondary and one upper secondary school from both public and private schools were selected randomly. Thereafter, a total of 140 students (65 students in the lower secondary level [40 from a public and 25 from a private school] and 75 students in the upper secondary level [45 from a public and 30 from a private school]) were selected based on the population proportion to answer the questionnaire.
One grade from each school and one class from each grade were randomly selected, and simple random sampling was then used according to class lists to reach the desired sample size. After specifying the samples, the researchers asked the mothers to participate in the study. An informed consent was obtained from all participants before conducting the study. The Ethics Committee of Yasuj University of Medical Sciences approved the study protocols (code: IR.YUMS.REC.1394.52).
To determine the sample size, the mothers’ communication skills were considered as the most important variable. A preliminary study found that 40% of mothers had good communication skills. According to Cochran’s sample size formula and multi-stage sampling and considering the mothers’ communication skills and the project coefficient (1.2) in two stages with an attrition value of 10%, the sample size was estimated to be 140.
Considering the level of education and socioeconomic status, the mothers were divided into four groups and provided with educational information during three two-hour sessions. The curriculum topics were determined based on a need analysis performed before the intervention established from group discussions. In the first session, the principles and objectives of the program were introduced, and necessary information was presented about human genital organs, the physiology of pregnancy, contraception methods, and breast cancer. In the second session, topics including mental health at puberty, sexual maturity, maturity-related health issues, and sexually transmitted diseases were discussed. In the third session, effective communication and interpersonal skills were explained. All sessions were held in the health center of Mahshahr. Lectures and interactive (question and answer) methods were used during all three sessions, while educational content was presented in the form of slides and manuals. Considering the topic and the mothers’ education level, different teaching methods were used for each group.
The data collection instruments included two questionnaires. The first questionnaire was used to assess individuals’ awareness and attitudes towards sexual issues. The questionnaire framework was extracted from “Illustrative questionnaire for interview-surveys with young people” developed by John Cleland, available on the World Health Organization (WHO) website (17). The questionnaire was translated into Persian by a qualified translator, then back-translated by a native-like translator. The mistakes of Persian version were identified and modified by comparing the original scale with its English equivalent. Since parts of the questionnaire were inconsistent with Iranian culture, some items were removed after consultation with sexuality education experts. Finally, an 80-item questionnaire was defined, consisting of three subsections: demographic information, awareness-relevant items, and statements on attitudes towards sexuality. The score of awareness ranged between 23 and 46, and the score of attitude ranged between 20 and 60.
The questionnaire’s content validity was confirmed by experts, and its reliability was also established using the test-retest approach for 20 respondents who were independent of the selected sample. Cronbach’s alpha values were 0.71 and 0.81 for the awareness and attitude items, respectively. In social science research, 0.70 is generally held to indicate a reliable scale.
The second instrument was the “Child-Parent Relationship: Mother” questionnaire consisting of 24 items to gauge the opinion of young people about their relationship with their parents (18). The score of this questionnaire ranged between 24 and 168. This questionnaire has previously been used by Iranian researchers. To indirectly measure the mothers’ communication skills, this questionnaire was administered to adolescent girls whose mothers participated in the study before the intervention and then three months after the study. A seven-point Likert scale (ranging from zero [almost none] to seven [very much]) was used to score the scale. The data obtained from both questionnaires were analyzed using SPSS software version 16 with parametric statistics such as paired-sample t-tests and the equivalent for non-parametric statistics. The questionnaires used before the intervention were administered again three months after the intervention and then compared. Means and standard deviations were calculated, and statistical analysis was performed using a paired t-test. A confidence interval of 95% with significance at P < 0.05 was used.
4. Results
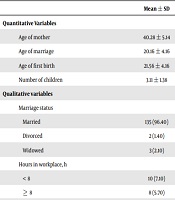
The mean age and standard deviation of girls were 14.6 ± 1.7 years. The average age of mothers participating in the study was 40 ± 5 years. Table 1 shows the demographic characteristics of the mothers. Compared with the pre-intervention phase, mothers’ awareness of sexual issues and attitudes towards sexuality education significantly increased; however, no significant difference was observed between mothers’ communication skills before and after the intervention (Table 2). Only 23% (32) of girls talked about sexuality with their mothers, and 22% (31) talked with persons other than their mothers. Moreover, 78% (109) of mothers asserted that they did not talk about sexuality with any other family members or friends except their own mothers.
| Variables | Mean ± SD |
|---|---|
| Quantitative Variables | |
| Age of mother | 40.28 ± 5.14 |
| Age of marriage | 20.16 ± 4.16 |
| Age of first birth | 21.56 ± 4.16 |
| Number of children | 3.11 ± 1.38 |
| Qualitative Variables | |
| Marriage status | |
| Married | 135 (96.40) |
| Divorced | 2 (1.40) |
| Widowed | 3 (2.10) |
| Hours in workplace, h | |
| < 8 | 10 (7.10) |
| ≥ 8 | 8 (5.70) |
| Job | |
| Employed | 18 (12.90) |
| Housewife | 122 (87.10) |
| The number of daughters aged 12 - 18 | |
| One | 110 (87.60) |
| Two | 30 (21.40) |
| Education level | |
| Illiterate | 11 (9.70) |
| Under diploma | 71 (50.70) |
| Diploma | 35 (25) |
| Academic | 23 (16.40) |
| Education level of husband | |
| Illiterate | 7 (5) |
| Under diploma | 55 (39.30) |
| Diploma | 56 (40) |
| Academic | 22 (15.70) |
| Ethnicity | |
| Lor | 19 (13.60) |
| Turkish | 4 (2.9) |
| Arab | 72 (51.40) |
| Persian | 45 (32.10) |
Demographic Information of Mothers
| Before | After | P-Valueb | |
|---|---|---|---|
| Knowledge | 30.06 ± 4.33 | 36.50 ± 7.20 | < 0.001 |
| Attitude | 46.65 ± 6.80 | 48.57 ± 5.26 | < 0.001 |
| Intercommunication skills | 94.88 ± 12.10 | 94.85 ± 11.78 | 0.98 |
| Effective communication skills | 40.01 ± 6.75 | 40 ± 6.09 | 0.98 |
Comparison of Knowledge, Attitude, Intercommunication Skills and Effective Communication Skills of Mothers
In general, mothers regarded their major source of information on sexual issues, in a descending order of importance, as follows: mother, teacher, sister, other family members, books, magazines, and friends. However, 15%, 30%, and 33% of these mothers had received no education about puberty, the reproductive system, or sexual relationships, respectively. A total of 32% (45) participants had received training on maturity at school when they were adolescents; however, 43% had received no training in this area at schools. Furthermore, about 54% (75) had received no training on maturity, sexual issues, the reproductive system, or sexual relations at school, and only 42% (58) had received such training at schools.
In the present study, a significant correlation was observed between mothers’ employment and education level and acceptance of sexuality education for their daughters. All working mothers and mothers with higher levels of academic education agreed with the importance of teaching their daughters about sexuality; however, only 61% of housewives agreed with this issue (P < 0.001). Maternal ethnicity was not significantly associated with the acceptance of sexuality education for their daughters. In general, mothers both before and after the study preferred sexuality education to be provided by mothers and teachers, family members, books and magazines, and friends, respectively, in descending order of importance. However, some participants suggested not teaching adolescent girls about sexuality at all. Although priorities specified by mothers concerning educational resources for girls did not change after the intervention, a small percentage of mothers changed their minds about who should provide training, shifting from mothers to teachers as a better option. During the training sessions, mothers were informed that sexuality education for girls should be scientific and accurate, and some mothers were not confident in their ability to provide such information.
Before the intervention, 52% (73) of mothers were familiar with all contraceptive methods. After the intervention, 75% of participants became familiar with all contraceptive methods (Table 3). In response to the question on teaching the most significant contraceptive method to adolescent girls, before the intervention, 46% (65) preferred none of the methods, and 17% (24) agreed that all contraceptive methods should be taught. Again, before the intervention, 14% (20) and 13% (18) of participants regarded the use of condoms and pills as essential knowledge, respectively. Following the intervention, the percentage of mothers who preferred none of the methods should be taught decreased to about 38% (54), and the percentage who agreed that all contraceptive methods should be taught increased to 24% (33). Additionally, the number of mothers who considered the use of condoms and pills as essential knowledge increased slightly to 15% (21) and 14% (19), respectively.
| Number of methods | Before, No. (%) | After, No. (%) |
|---|---|---|
| One method | 37 (26.40) | 25 (17.90) |
| Two methods | 11 (7.90) | 1 (0.70) |
| Three methods | 7 (5) | 9 (6.40) |
| Four methods | 5 (3.60) | 0 (0) |
| Five methods | 6 (4.30) | 0 (0) |
| All methods | 73 (52.10) | 105 (75) |
| None of them | 1 (0.70) | 0 (0) |
Comparison of Mothers’ Awareness about Contraceptive Methods
5. Discussion
In our study, the mothers’ levels of awareness increased after the educational intervention. Moreover, the mothers’ attitudes towards sexuality education positively improved following an educational intervention. However, after the intervention, some mothers still believed that their adolescent daughters’ premarital knowledge of sexuality and contraception methods could motivate them to experience it. They also believed that there is no need for girls to be familiar with sexual issues before the marriage.
Our results are consistent with most of the similar studies. For example, significant changes were reported in terms of awareness and attitudes towards sexuality education of children in South Korea (19). Similar to our results, a study in Iran found that parents did not hold a positive attitude towards sexuality education for adolescents (12, 13). However, in a study by Latifnejad et al. (20), a majority of adolescent girls and adults acceded to the importance of sexual health education for adolescent girls. The results of another study in Sari, Iran, indicated that puberty was an unpleasant experience for most of the study participants, and they often needed to be educated about sexual maturity-related issues (21). Hence, adolescents, especially girls, should receive adequate information about different aspects of sexuality since sexuality education has effects on health behaviors, healthy sexual behavior, mental health, prevention of sexual dysfunction, family health, appropriate gender identity, and increasing sexual health and satisfaction in future marital life (12, 22-24). Such training should be associated with issues such as sexual harassment, sexual orientation, abortion, birth control (25), and the use of condoms to prevent sexually transmitted diseases and enhance behavioral interventions in preventing unwanted pregnancies and resistance to sexually transmitted diseases (26).
The findings of the present study revealed that some mothers believed that it would be problematic if their husbands found out that their adolescent girls posed questions about sexuality. In other studies conducted in Iran, cultural taboos and resistance were mentioned (2, 7, 12).
In the current study, no significant difference was observed between mothers’ communication skills before and after the educational intervention. Other studies reported poor relationships between parents and adolescents in terms of sexual and reproductive health issues (13, 14, 27, 28). Regarding the ineffectiveness of intervention programs in developing communication skills, several points should be noted. First, according to psychologists, communication skill assessments should be done by observing behaviors in a natural setting to obtain realistic results. Assessing these skills through self-report approaches is often of limited value. Most of the girls were unaware of the course topics and objectives of this program; hence, they may not have addressed relevant sexual questions with their mothers within the first three months after the intervention. Consequently, mothers may have had no opportunity to apply these skills to convey information to their daughters.
Due to the mothers’ unwillingness to participate in multiple sessions, skill training sessions were limited to two sessions, and class practices and exercises that required more time were removed from the program so that the training sessions would suffice. Further findings from the current study showed that a majority of mothers before and after the study preferred sexuality education for girls to be provided by mothers and teachers, family members, books and magazines, and friends, respectively. Some participants, however, suggested not teaching girls about sexuality education at all. In line with the results of the present study, mothers were the most important source in providing information about sexual maturity and sexual issues (29, 30).
It is recommended to conduct similar studies among adolescent boys and girls to assess their educational needs and to develop a comprehensive training program for adolescents. In addition, concurrent studies with parents and teenagers could be designed to achieve better and more efficient results (e.g., among fathers and their adolescent sons). Although the educational needs of mothers from different ethnic groups and cultures were assessed in this study, these mothers belong to a limited population of our country. Hence, it is suggested to perform a needs assessment across the country to design a curriculum based on the needs of the audience to be submitted to the Ministry of Education and to be adopted for training parents. Furthermore, preparation and distribution of various audio-visual programs relevant to communication skills by the media, which can enhance the effectiveness of the training, as well as the use of the program and training manuals designed for this project by health centers in cities to train parents, teachers, and adolescents, are also proposed.
Lack of randomization and lack of a comparison group were the major limitations of this study. Moreover, due to cultural and legal limitations, we could not include adolescent girls in the study, in which case more comprehensive results and clearer views would be obtained. As another limitation, there was no possibility of direct observation for mother-child mutual relations; thus, the assessment criterion was the adolescents’ reports.
5.1. Conclusions
Awareness increased, and attitudes improved towards sexual issues after the intervention for mothers with adolescent girls aged 12 to 18 years old living in Mahshahr. However, no changes were found in terms of effective communication and interpersonal skills. Most mothers believed that the best sexuality education resource for teaching adolescent girls is having trained mothers. Considering the results of this study and other similar studies, teaching family members, especially mothers, to practice effective communication skills with their children and to transmit correct scientific information about sexual issues seems necessary. The implementation of this training should be regular and continuous for parents and school authorities to be fruitful in raising adolescents.
