


1. Background
Throughout history, humans have tried various methods to influence their sexual behavior. In some cases, there is a general belief that sexual desire is higher in those who use stimulants or narcotics. Some individuals describe drug use as an alternative to adverse sexual experiences, and some note it as a way to achieve intimacy and eroticism in a relationship. Stimulants are substances that increase mood, activity, alertness, awareness, and stimulation of the central nervous system.
Findings confirm the link between substance use and high-risk sexual behavior (1, 2). By showing the complexity of the relationship between substance use and sexual risk behaviors, Stall and Purcell (3) concluded that situational studies often show a positive relationship between substance use and high-risk sexual behaviors. With different underlying mechanisms, we can explain the relationship between substance use and high-risk sexual behaviors. The two basic theories in this regard are the theory of expectation and the theory of cognitive escape.
The theory of expectation (4) emphasizes the importance of internalized cultural and social expectations about the effect of substances on sexual behavior. In this sense, people's expectations that substance abuse reduces or increases sexual pleasure make a person's sexual behavior more risky. Cognitive escape theory (5) based on the social psychological literature in relation to the cognitive burden imposed by behavioral limitations. In this sense, the constant suppression of thoughts about the tendency to engage in risky sexual behaviors predicts unsafe sexual encounters (6). Consistent with recent models of social psychology, Stall and Purcell (3) have suggested that for many people, sexual risk is not due to a lack of societal norms or personal standards, but to a desire to escape cognitive awareness of very precise norms and standards. They suggested that both substance use and the high arousal approach or other sexual settings facilitate this cognitive impairment, in which individuals execute "automated" sex scripts. Two categories of drugs that are usually abused in this regard are amphetamines and narcotics.
Amphetamine was discovered over 100 years ago. Initially, it was used as a panacea for several conditions; however, it has been converted into a highly controlled drug with restricted therapeutic applications (7). Amphetamines are psychostimulant drugs and speed up the messages traveling between the brain and the body (8). Amphetamines are a group of synthetic drugs that contain methamphetamine. The latter is a globally popular drug of abuse that induces euphoria, which in turn influences cognitive/psychomotor function and sleep. It also increases inclination toward risky behaviors and violence. The major impacts of methamphetamine can be attributed to the overproduction of neurotransmitters, which in turn increases the level of dopamine (9).
Narcotic is the term used by Drug Enforcement Administration (USA) to refer to drugs that are opioid analgesics (10). In this group, drugs with morphine-like action (narcotics) are known as narcotic pain relievers, which are used to treat all types of severe pain. The wide range of actions mediated by narcotic receptors justifies the use of these drugs in various clinical conditions. Narcotic analgesics and antagonist drugs are classified based on their origin or action on the narcotic receptor.
Researches have shown that consumption of methamphetamine is connected with an enhanced risk of human immunodeficiency virus (HIV) infection and high-risk sexual activity (11-14). Long-term methamphetamine use is associated with physical, psychological, and social adverse effects. The increased use of the drug is associated with more frequent sexual high-risk behaviors and increased risks for HIV transmission (15). Those who take methamphetamine at high frequencies are more likely to have sexual intercourse before the age of 13 (by four times), to have multiply sexual partners, and to becoming/get someone pregnant in comparison to those who use methamphetamine once to twice (16). In other hands, narcotic substances, such as opioids, have long been known to inhibit sexual behavior. For adolescents and young adults, opioid use is connected with drug use, high-risk sexual intercourse (e.g., HIV), and opioid overdose (17).
According to the literature provided by the psychosocial outpatient sample, consuming cocaine is connected with a higher likelihood of having several partners (by more than two-fold), trading sex for drugs, and anal sexual intercourse. In addition, some studies reported that alcohol or opioid use was connected with fewer risky behaviors. In the methadone maintenance sample, the use of cocaine, alcohol, and opiate each was connected with one or two risky behaviors. Associations between sexual risk and substance use days were less frequent in both samples (18). A total of 43 adolescents were treated for substance abuse over 20 months, and 70% of the subjects reported using three or more drugs, with a mean of 5.35 used drugs. Synthetic drugs, like cocaine or ecstasy, were the most frequently abused substance, behind the Cannabis. Additionally, 73.3% of adolescents who had high-risk multiple substance abuse fulfilled the diagnostic indicators for nonsuicidal self-injury (19).
Due to the fact that substance abuse affects sexual behavior (20), there are numerous different substances that change an individual’s sexual response cycle in a negative way, a positive way, or both (21). Some individuals use methamphetamine to increase sexual pleasure (22). Furthermore, sexual exaggeration, high Viagra, and high sexual impulses are observed in most methamphetamine users (21). However, the use of some narcotics leads to sexual dysfunction and orgasmic problems (22, 23). The present study sought to compare individuals’ beliefs about the effect of the drug or substance abuse on their sexual behaviors.
2. Objectives
The present study aimed to compare the effects of methamphetamine and narcotics on sexual high-risk behaviors. To this end, the following research questions were posed:
Can the use of methamphetamine and narcotics be a factor in high-risk sexual behaviors?
Which substance is most associated with dangerous behaviors?
3. Patients and Methods
This comparative study by comparing the sexual behaviors of two groups of substance abusers (amphetamines and narcotics) investigated the effect of these substances on sexual behaviors. For this purpose, 49 men with amphetamine abuse, including benzedrine, methamphetamine, and methylphenidate, and 42 men with drug abuse, including opium, heroin, codeine, morphine, and methadone, (for at least 6 months) were selected from the patients of Yareegar Clinic, Tehran, Iran, within 2019 - 2021 as the available sample. Before filling out the research questionnaires, they were completed by a few participants to ensure the understandability of the items. The ambiguities were removed to reduce misunderstandings and increase the accuracy of the items. Informed consent was obtained from each participant. The inclusion criteria were the age of 15 years and older and informed consent to participate in the study. Moreover, the exclusion criteria were having symptoms of psychosis, and suffering from a disease inhibiting cooperation in the study.
3.1. Instruments
3.1.1. High-Risk Sexual Behaviors in Substance Abuse
This 15-item questionnaire, which has prepared by Vaziri and Lotfi Kashani (24), evaluates drug users’ sexual desire and high-risk behaviors. Items are ranked on a 4-point Likert scale from never to ever. Each item in this questionnaire can be analyzed individually or in combination. The reliability of this questionnaire has reported 0.89 through test-retest method and 0.76 by Cronbach's alpha coefficient of 0.76.
4. Results
The descriptive components of variables showed that the mean age value of amphetamine and narcotics users was equal to 30.91 ± 4.59 and 32.16 ± 4.46 years respectively. Age differences between the two groups were not significant (P = 0.194) and There were no significant differences between the two groups in terms of education, marital status, and use duration (P > 0.05) (Table 1).
| Variables | Amphetamine Group | Narcotics Group | P Value |
|---|---|---|---|
| Age | 30.91 ± 4.59 | 32.16 ± 4.46 | > 0.05 |
| Marital status | |||
| Married | 31 (63.26) | 29 (69.04) | > 0.05 |
| Single | 18 (36.73) | 12 (28/57) | |
| Divorced | 0 | 1 (.02) | |
| Education | |||
| Diploma | 6 (12.24) | 4 (9.75) | > 0.05 |
| Bachelor | 34 (69.38) | 29 (69.04) | |
| Master and higher | 9 (18.36) | 9 (21.42) | |
| Use duration | 3.93 ± 1.54 | 4.04 ± 1.46 | > 0.05 |
Demographic Data of Participants
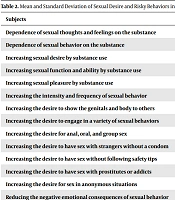
Table 2 shows the descriptive statistics (i.e., mean and standard deviation) of the research variables.
| Subjects | Methamphetamine | Narcotics | Total |
|---|---|---|---|
| Dependence of sexual thoughts and feelings on the substance | 2.41 ± 0.734 | 2.24 ± 2.33 | 0.850 ± 0.790 |
| Dependence of sexual behavior on the substance | 2.00 ± 0.935 | 1.71 ± 1.019 | 1.87 ± 0.980 |
| Increasing sexual desire by substance use | 2.31 ± 0.871 | 1.71 ± 0.944 | 2.03 ± 0.948 |
| Increasing sexual function and ability by substance use | 2.45 ± 0.503 | 2.55 ± 0.504 | 2.49 ± 0.503 |
| Increasing sexual pleasure by substance use | 2.45 ± 0.614 | 1.64 ± 0.656 | 2.08 ± 0.749 |
| Increasing the intensity and frequency of sexual behavior | 2.51 ± 0.681 | 2.60 ± 0.627 | 2.55 ± 0.654 |
| Increasing the desire to show the genitals and body to others | 2.27 ± 0.884 | 2.14 ± 0.977 | 2.21 ± 0.925 |
| Increasing the desire to engage in a variety of sexual behaviors | 1.96 ± 0.978 | 2.02 ± 0.950 | 1.99 ± 0.960 |
| Increasing the desire for anal, oral, and group sex | 2.35 ± 0.830 | 2.38 ± 0.936 | 2.36 ± 0.876 |
| Increasing the desire to have sex with strangers without a condom | 2.43 ± 0.577 | 2.48 ± 0.505 | 2.45 ± 0.543 |
| Increasing the desire to have sex without following safety tips | 2.31 ± 0.871 | 2.50 ± 0.707 | 2.40 ± 0.801 |
| Increasing the desire to have sex with prostitutes or addicts | 1.98 ± 0.989 | 1.88 ± 0.889 | 1.93 ± 0.940 |
| Increasing the desire for sex in anonymous situations | 2.27 ± 0.785 | 1.52 ± 0.671 | 1.92 ± 0.820 |
| Reducing the negative emotional consequences of sexual behavior | 1.57 ± 0.590 | 2.27 ± 0.569 | 1.95 ± 0.673 |
| Increasing intimacy and eroticism in a relationship | 2.45 ± 0.679 | 1.86 ± 0.814 | 2.18 ± 0.797 |
Mean and Standard Deviation of Sexual Desire and Risky Behaviors in Amphetamine and Narcotic Groups a
In Table 3, we have compared sexual desire and high-risk behaviors in two amphetamine and narcotic groups. Since the homogeneity of variances in all 15 items was not significant for the groups, analysis of variance was used to compare the two groups.
| Subjects | SS | df | MS | F | Sig. | |
|---|---|---|---|---|---|---|
| Dependence of sexual thoughts and feelings on the substance | Between groups | 0.654 | 1 | 0.654 | 1.05 | 0.308 |
| Dependence of sexual behavior on the substance | Between groups | 1.846 | 1 | 1.84 | 1.94 | 0.167 |
| Increasing sexual desire by substance use | Between groups | 7.922 | 1 | 7.92 | 9.66 | 0.001 |
| Increasing sexual function and ability by substance use | Between groups | 0.220 | 1 | 0.220 | 0.869 | 0.354 |
| Increasing sexual pleasure by substance use | Between groups | 14.69 | 1 | 14.69 | 36.57 | 0.001 |
| Increasing the intensity and frequency of sexual behavior | Between groups | 0.164 | 1 | 0.164 | 0.379 | 0.540 |
| Increasing the desire to show the genitals and body to others | Between groups | 0.339 | 1 | 0.339 | 0.393 | 0.532 |
| Increasing the desire to engage in a variety of sexual behaviors | Between groups | 0.094 | 1 | 0.094 | 0.101 | 0.751 |
| Increasing the desire for anal, oral, and group sex | Between groups | 0.026 | 1 | 0.026 | 0.034 | 0.855 |
| Increasing the desire to have sex with strangers without a condom | Between groups | 0.051 | 1 | 0.051 | 0.172 | 0.679 |
| Increasing the desire to have sex without following safety tips | Between groups | 0.850 | 1 | 0.850 | 1.32 | 0.252 |
| Increasing the desire to have sex with prostitutes or addicts | Between groups | 0.220 | 1 | 0.220 | 0.247 | 0.621 |
| Increasing the desire for sex in anonymous situations | Between groups | 12.43 | 1 | 12.43 | 23.04 | 0.001 |
| Reducing the negative emotional consequences of sexual behavior | Between groups | 10.88 | 1 | 10.88 | 32.47 | 0.001 |
| Increasing intimacy and eroticism in a relationship | Between groups | 7.922 | 1 | 7.922 | 14.31 | 0.001 |
Summary of Analysis of Variance of Variables in Two Groups
According to Table 3, the investigation of behaviors in the two groups presented significant differences between the two groups in increasing sexual desire, sexual pleasure, desire for having sex in anonymous situations, intimacy, and eroticism by substance use and reducing the negative emotional consequences of sexual behavior.
5. Discussion
In this study, the investigation of sexual behaviors of 91 amphetamine and drug users showed that amphetamine and drug use was significantly effective in sexual desire, function, and high-risk sexual behaviors. This finding is consistent with previous findings, such as high-risk sexual behaviors (11-13, 17), frequent sexual risk behaviors (15, 16), and vaginal, anal, or oral sex (14).
Amphetamines as psychostimulant drugs who speed up the messages traveling between the brain and the body (8) results in a rapid, delightful rush followed by euphoria, increased attention, and high energy. these drugs are connected with an enhanced high-risk sexual activity (11). The past presented results showed that the initiation of methamphetamine use increases sexual high-risk behaviors (12). Long-term methamphetamine use is associated with physical, psychological, and social adverse effects. The increased use of the drug is associated with more frequent sexual high-risk behaviors and increased risks for HIV transmission (15).
Those who take methamphetamine at high frequencies are more likely to have sexual intercourse before the age of 13 (by four times), to have multiply sexual partners, and to becoming/get someone pregnant in comparison to those who use methamphetamine once to twice (16). Researchers showed that a large proportion of methamphetamine users engaged in risky sexual behaviors, such as having sex without a condom, having several sexual partners, and having a history of sexually transmitted infections (13). Findings also show that men use methamphetamine to increase sexual pleasure; however, women, through their sexual partners, become acquainted with this substance and use it to lose weight (9). The likelihood of having vaginal, anal, or oral sex, becoming pregnant/being responsible for a pregnancy, and being diagnosed with a sexually transmitted infection were significantly higher among students with a history of methamphetamine in the past 30 days in comparison to those who did not use methamphetamine (14).
Narcotic substances, such as opioids, have long been known to inhibit sexual behavior. For adolescents and young adults, opioid use is connected with drug use, high-risk sexual intercourse (e.g., HIV), and opioid overdose (17). For women with childhood sexual abuse, an increase in days of cocaine/stimulant use was connected with a significant enhancement in unprotected sexual occasions (USOs). However, the longer the duration of opiate use, the lower the USOs. There was a significant increase in USOs with enhanced opiate use among women who did not report childhood sexual abuse (25). It seems that, the activation of micro receptors by endomorphin-1 modifies parameters associated with ejaculation (increasing ejaculation latency and reducing the number of ejaculations), confirming the release of opioids during sexual intercourse (26). A total of 43 adolescents were treated for substance abuse over 20 months, and 70% of the subjects reported using three or more drugs, with a mean of 5.35 used drugs. Synthetic drugs, like cocaine or ecstasy, were the most frequently abused substance, behind the cannabis. Additionally, 73.3% of adolescents who had high-risk multiple substance abuse fulfilled the diagnostic indicators for nonsuicidal self-injury (19).
More important in this study were the answers of methamphetamine and drug users to items 14 and 15. Narcotic users reported that the negative emotional consequences of their high-risk sexual behaviors are decreased through substance use. Nevertheless, methamphetamine users reported that using the substance helps them to increase their intimacy and eroticism in the sexual relationship. The aforementioned issues need to be addressed in terms of controlling negative emotions and increasing pleasure. However, drug use motivations are complex and might vary by population. Following a thematic analysis approach, Stanton et al. showed that substance use was considered (1) a way to increase intimacy and have better sexual intercourse; (2) a pathway to improve access to partners and gain entry to a community; and (3) a potential way for empowerment (27). Methamphetamine is a stimulant that powerfully activates brain chemicals linked to feelings of reward and pleasure. Some methamphetamine users find that, at first, the drug enhances sexual desire; nonetheless, over time, the drug’s effects on your sex life can be very negative.
These results show that the conceptualization of consumer beliefs as a latent variable may play an important role in consumer spending. There is evidence that expectancies alone, even in the absence of actual consumption, are enough to change people’s behavioral intentions. For example, in a balanced placebo design study, individuals who believed they had consumed alcohol, but who had actually consumed a placebo drink, reported stronger intentions to engage in unsafe sex and lower perceptions of risk when compared to those who consumed a placebo and did not believe they were drinking alcohol (28). In research with men who have sex with men, those who reported unprotected sex more strongly believed in the sexual effects of substances, when compared to men who did not engage in unprotected sex (29).
5.1. Conclusions
As shown in Table 2, thoughts, feelings, sexual behavior, libido, sexual function and ability, and sexual pleasure increase with using amphetamines. A kind of sexual arousal in the form of a sharp and frequent increase in sexual behavior increases the desire to show the genitals and body to others, perform various sexual behaviors, and the likelihood of penetration, anal intercourse, oral sex, and masturbation as consequences. However, there was no difference between the two groups in high-risk behaviors such as having sex with strangers without condoms, insecure sex with prostitutes, and addicted or infected people. Both groups are exposed to the disuse of condoms, carelessness in choosing a sexual partner and having high-risk sex with prostitutes or unknown individuals.
Based on the findings, it is suggested that the sexual problems of drug abusers should be evaluated before and after drug use and considered in therapeutic interventions. Also, examining this issue among women and comparing their circumstances with men can be effective in clarifying the issue further.
