


1. Background
Coronaviruses constitute a large group of viruses capable of causing a range of respiratory infections, from common colds to more severe illnesses. The recent emergence of the novel coronavirus, COVID-19, led to a global epidemic in 2019 (1). The areas with COVID-19 cases, approved by the World Health Organization (WHO), include Africa, America, Europe, Southeast Asia, and the Western Pacific (2). In Iran, COVID-19 quickly spread, posing a significant threat to both the physical and psychological well-being of its citizens. Typical symptoms of the virus include fever, cough, and dyspnea (3). COVID-19 is characterized by its unpredictability, posing a substantial threat to individuals' physical health and affecting their mental well-being (4). Home quarantine measures have been widely adopted as a key strategy for controlling the global spread of the disease (5).
Quarantine involves the separation and restriction of movement for individuals potentially exposed to an infectious disease to prevent its transmission, thus reducing the risk of infecting others (6). The term "quarantine" originated during a leprosy outbreak in Venice, Italy (7) and has become a common practice during the COVID-19 pandemic, with many countries implementing this measure to avoid the further spread of the disease (8). Domestic violence refers to aggressive behavior occurring in couples' relationships. Incidents of domestic violence have increased as couples are confined to their homes due to the pandemic. According to Barnett et al., domestic violence is a form of aggressive and coercive behaviors, including physical, sexual, and psychological abuse, as well as economic pressure and threats used by individuals against their spouses or partners (9).
Anxiety caused by COVID-19 is a significant factor associated with couples' violence. Anxiety stemming from the COVID-19 pandemic has affected numerous individuals, negatively impacting their immune systems, rendering them more susceptible to diseases, occasionally leading to maladaptive behaviors, and significantly diminishing their quality of life. Ahmadzad-Asl et al. (10) examined the association between domestic violence, anxiety, and depression in 615 married women, finding that 32.7% of women with depression and anxiety experienced domestic violence. Additionally, Peterman and Dixon (11) established a connection between domestic violence in couples and personality traits. Individuals with such tendencies often exhibit mental disorders, substance abuse problems, and criminal histories. Those engaging in more frequent and severe violence are more likely to have a criminal record and be subject to arrest.
Cognitive emotion regulation is another crucial variable that needs to be investigated in the context of marital violence. Many problematic couples are less skilled in the cognitive regulation of their emotions, making it challenging for them to use coping strategies to improve their emotional states (12). "Emotion regulation" is a term used to describe a person's ability to effectively manage and respond to emotional experiences. People unconsciously use emotion regulation strategies throughout the day to cope with challenging situations. Emotion regulation strategies are typically categorized into 3 groups: Attentional control, cognitive reappraisal, and response modulation. Emotion regulation plays a vital role in how individuals cognitively process traumatic and stressful events (13).
Research indicates that individuals employ various strategies in stressful situations, some of which are adaptive, while others are maladaptive. These strategies may include self-blame, blaming others, rumination, and catastrophizing. Garnefski and Kraaij (14) identified a significant association between stress, emotional problems, and cognitive regulation strategies. In other words, individuals may exhibit either adaptive or non-adaptive responses to life's stressors depending on their chosen strategies. The use of catastrophizing and rumination strategies, for example, can exacerbate emotional problems when dealing with stress. Nolen-Hoeksema et al. (15) reported an association between rumination strategies and high levels of depression. On the other hand, longitudinal and cross-sectional investigations demonstrated a high association between marital satisfaction and depressive symptoms (16).
Another factor related to marital violence is distress tolerance, defined as the ability to experience and tolerate negative psychological states. Distress tolerance is the capacity to manage emotional incidents without feeling overwhelmed, allowing individuals to return to a state of equilibrium more quickly when facing new stressors (17). Distress may arise from cognitive or physical procedures, but it primarily manifests as emotional distress. Distress tolerance is a variable of individual dissimilarities referring to the capacity to experience and tolerate emotional distress (18). Individuals with low distress tolerance may perceive emotions as unbearable and believe they lack the means to manage and control their distress. They may also deny the existence of their emotions and experience shame, as they feel incapable of coping with their emotional states (19). As reported by Tavares and Aassve, low psychological abilities are a major contributor to failures in emotional and marital relationships (20).
The coronavirus has not only triggered a global health crisis but is also evolving into an economic challenge. Home quarantine measures have been implemented to control the spread of the new coronavirus. However, these measures have given rise to issues within families, particularly among couples, leading to an increase in domestic violence and raising concerns among officials worldwide. It has become evident that for many, home is not a safe place during these times. The fear of a disease outbreak, feelings of hopelessness, reduced tolerance, anxiety over the economic consequences of the pandemic, and worries about food scarcity are contributing factors that heighten the risk of mental distress during quarantine. Importantly, these conflicts are not limited to couples who have previously experienced domestic violence; families, in general, are facing significant pressures. To prevent mental and psychological health problems, as well as other social harms, individuals can make quarantine conditions more bearable by engaging in activities like studying and reading books. Research has shown that reading, in particular, plays a significant role in preventing conditions such as depression and stress (21). Furthermore, health stress and depression among couples who are spending lengthier time alongside one another nowadays have elevated marital disputes and reduced their patience (21). Given that the family is a social system and one of the pillars, it is the core of society and is, in a way, the smallest social cell. Knowing and investigating the factors affecting it in terms of compatibility (22).
2. Objectives
The strength of the family is crucial in recognizing the predictions of domestic violence. The possibility of identifying people at risk and awareness of increasing preventive strategies given that previous research has shown that corona anxiety, cognitive emotion regulation, and distress tolerance play an effective role in domestic violence, researchers have hypothesized that the simultaneous presence of these cases may play a role in explaining domestic violence. Therefore, the present study answered this question and investigated the role of these factors in interaction with each other concerning domestic violence.
3. Materials and Methods
A descriptive-analytical multivariate design was employed to examine the research variables in couples who had experienced domestic violence during quarantine. To do so, all couples living in Mashhad City and living together during the COVID-19 quarantine period were considered as the research population.
In the data collection phase, questionnaires were administered to participants by psychiatrists and clinical psychologists. The study included couples who were married and in-home quarantine during the COVID-19 pandemic. Additionally, individuals under the age of 60 and those with at least a 6th-grade education were included as part of the criteria for participation. The research questionnaires were sent to eligible couples, who subsequently completed them. Finally, the collected data were analyzed using SPSS version 22.
In this descriptive-analytical research, the statistical population consisted of all married individuals who participated in the “participation of married people in social networks.” Considering the inclusion criteria of being married and experiencing quarantine during the COVID-19 pandemic, a total of 376 respondents completed the questionnaires using an available and targeted sampling. Responses from 26 participants were excluded because some of the items were missing. Before choosing the statistical sample, all research purposes were explained to the participants. They completed a consent form, along with the Conflict Tactics Scale (CTS-2), Distress Tolerance Scale (DTS), Emotion Regulation Strategies Questionnaire (ERQ), and Corona Disease Anxiety Scale (CDAS). The collected data were analyzed using SPSS version 22, employing descriptive statistics (mean and SD) and inferential statistics (Pearson correlation and multiple linear regression [MLR]).
3.1. The Following Tools Were Employed in This Study
3.1.1. Conflict Tactics Scale
This scale is unique in that it measures both the severity and frequency of various dimensions of violence, including perpetrating and experiencing violence. It consists of 79 questions categorized into 4 scales: Psychological aggression, physical assault, sexual coercion, and physical harm. Additionally, it is considered a non-violent method of assessing negotiation in couples’ interplays. Theoretically, the CTS is based on conflict (23), according to the hypothesis that conflict is an unavoidable part of human relationships. In contrast, violence is not thought of as a long-lasting solution without an alternative. Thus, CTS-2 measures using specific solutions and tactics, including physical violence. One of the strengths of the CTS-2 is its focus on specific actions and events in the couple's relations. The reliability of CTS, resulting from 80 investigations, is reportedly at a desired and suitable level. A mean alpha of 0.88 was calculated in heterosexual, married, and engaged couples, and a reliability coefficient of 0.79 was reported by Straus et al. (24).
3.1.2. Distress Tolerance Questionnaire
This questionnaire is a self-assessment tool designed by Simons and Gaher (2005) to measure distress tolerance. It comprises 15 items divided into 4 subscales: Emotional distress tolerance, absorption of negative emotions, mental appraisal of distress, and regulation of efforts to mitigate distress. The options of this instrument are marked on a 5-point Likert scale, ranging from 1 (complete agreement) to 5 (complete disagreement). Higher scores indicate greater distress tolerance (25). Hawkins et al. (26) reported an internal consistency of the scale at 0.91. Azizi (27) have standardized the Persian version of this questionnaire. Cronbach's alphas for the subscales of tolerance, absorption, appraisal, and regulation were reported at 0.71, 0.69, 0.77, and 0.73, respectively. The correlations of the Distress Tolerance Scale with problem-based, emotion-based, and less effective and ineffective coping styles were reported at 0.213, -0.278, -0.337, and -0.196, respectively. In Iran, this questionnaire was initially employed in a survey by Alavi et al. to evaluate the symptoms of depression in students. According to our findings, the internal consistency reliability for the whole scale was estimated at 0.71, and moderate reliability was obtained for the subscales of tolerance (0.54), absorption (0.42), appraisal (0.56), and regulation (0.58). Our estimated Cronbach's alpha of this questionnaire for the whole scale was 0.72, and values of 0.56, 0.51, 0.61, and 0.49 were obtained for the subscales of tolerance, absorption, appraisal, and regulation, respectively (28).
3.1.3. Emotion Regulation Strategies Scale
This scale was developed by Gross and John (29) in 2003. It consists of 10 items divided into 2 subscales: Reappraisal (6 items) and suppression (4 items). Answers are scored on a 7-point Likert scale ranging from 1 to 7. Cronbach's alpha coefficients for reappraisal and suppression were obtained at 0.79 and 0.73, respectively, and retest reliability for the whole scale was 0.69 (30). At the University of Milan, the internal consistency coefficient of this scale was obtained from 0.48 to 0.68 for reappraisal and 0.42 to 0.63 for suppression (31).
3.1.4. Corona Disease Anxiety Scale
This scale was developed and validated to assess anxiety related to the spread of coronavirus in Iran. It consists of 18 items grouped into 2 components (factors). Items 1 - 9 measure psychological symptoms, while items 10 - 18 assess physical symptoms. This scale is marked on a 4-point Likert scale (never = 0, sometimes = 1, often = 2, and always = 3). Hence, the uppermost and lowermost scores of the respondents to this questionnaire will be from 0 to 54. In this questionnaire, high marks suggest greater anxiety in participants. Using Cronbach's alpha procedure, the reliability values of this tool for the first factor, second, and the whole questionnaire were obtained at 0.879, 0.891, and 0.919, respectively (32).
4. Results
The study included 350 participants, comprising 175 males and 175 females, with a mean age of 39 years. Descriptive information on emotion regulation, distress tolerance, and domestic violence subscales is presented in Table 1.
| Variables | Mean ± SD |
|---|---|
| Corona anxiety (total) | 21.22 ± 10.58 |
| Suppression | 26.24 ± 9.76 |
| Reappraisal | 16.19 ± 7.93 |
| Emotion regulation (total) | 41.43 ± 18.52 |
| Tolerance | 9.15 ± 2.23 |
| Absorption | 9.28 ± 2.87 |
| Appraisal | 15.58 ± 4.63 |
| Regulation | 8.61 ± 2.97 |
| Distress (total) | 42.62 ± 12.11 |
| Psychological violence | 14.29 ± 5.63 |
| Physical violence | 3.86 ± 1.11 |
| Sexual violence | 1.79 ± 0.89 |
| Economic violence | 1.43 ± 0.64 |
| Domestic violence (total) | 21.37 ± 9.87 |
The normal distribution of research variables was assessed using the Kolmogorov-Smirnov test, which compares the observed and the theoretical or expected cumulative distribution functions. This test compares whether the distribution of a trait in a sample matches the presumed population distribution. A significant value greater than 0.05 in this test suggests a normal distribution. Accordingly, all variables have a normal distribution based on the significant levels reported for corona anxiety, emotion regulation, and distress tolerance (Table 2).
| Variables | Kolmogorov-Smirnov Significance Level |
|---|---|
| Corona anxiety | 0.21 |
| Emotion regulation | 0.32 |
| Distress tolerance | 0.15 |
| Domestic violence | 0.11 |
Table 3 shows the results of the Pearson correlation test, indicating a significant association between corona disease anxiety and domestic violence (P = 0.001). The correlation coefficient (0.51) value between corona anxiety and domestic violence suggests that the 2 variables are positively and directly correlated. It indicates the rise of domestic violence with increasing corona anxiety and vice versa.
| Variables | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Corona anxiety | - | |||
| 2. Emotion regulation | -0.59 a | - | ||
| 3. Distress tolerance | -0.62 a | 0.71 a | - | |
| 4. Domestic violence | 0.51 a | -0.45 a | -0.38 b | - |
a P = 0.01
b P = 0.05
Furthermore, there is a significant correlation between emotion regulation and domestic violence (P = 0.001). The correlation coefficient (0.45) between emotion regulation and domestic violence indicates that the 2 variables are negatively and inversely correlated, meaning that domestic violence diminishes with increasing emotion regulation and vice versa.
Lastly, distress tolerance and domestic violence (P = 0.005) are significantly correlated. The correlation coefficient (0.38) value between distress tolerance and domestic violence suggests that the 2 variables are negatively and inversely correlated. It indicates the decline of domestic violence with increasing distress tolerance and vice versa.
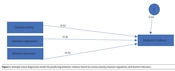
Figure 1 depicts an MLR model to predict domestic violence based on corona anxiety, emotion regulation, and distress tolerance. According to the MLR model and its standardized output in Amos version 23, it can be argued that the intensities of the effects of corona anxiety on domestic violence, emotion regulation on domestic violence, and distress tolerance on domestic violence are 52%, -41%, and -33%, respectively. The model's coefficient of determination (R2) is 53%, suggesting that 52% of the variance of domestic violence is explainable by independent research variables (corona anxiety, emotion regulation, and distress tolerance).

Multiple linear regression model for predicting domestic violence based on corona anxiety, emotion regulation, and distress tolerance.
According to Table 4, all P-values in the regression model are <5%, indicating that all 3 independent variables, namely corona anxiety, emotion regulation, and distress tolerance, have a significant influence on domestic violence. Based on the Bootstrap test, which determines the significance level of R2, the significance of this test is generally <5%, and it is not zero in the lower and upper limits (Table 5). Accordingly, it can be argued that the independent variables (corona anxiety, emotion regulation, and distress tolerance) significantly impact the dependent variable (domestic violence). Thus, domestic violence can be predicted based on corona anxiety, emotion regulation, and distress tolerance.
| Scales | β | t | R² | P-Value |
|---|---|---|---|---|
| Corona anxiety | -0.28 | -2.85 | 0.26 | 0.01 |
| Emotion regulation | 0.22 | 2.23 | 0.20 | 0.01 |
| Distress tolerance | 0.31 | 3.15 | 0.14 | 0.02 |
| Standardized Values | Lower Bound | Upper Bound | Sig |
|---|---|---|---|
| 53% | 29% | 50% | 45% |
5. Discussion
This study aimed to assess the impacts of corona anxiety, cognitive emotion regulation, and distress tolerance on couples' domestic violence during quarantine. The results of the regression analysis indicated that the variables of corona anxiety, cognitive emotion regulation, and distress tolerance explained couples' domestic violence. Altogether, the introduced model explained 52% of the variance in domestic violence. Amongst the examined factors, the emotion regulation variable most strongly affected the couples' domestic violence variable.
The first key finding of this study suggests that corona anxiety had a positive influence on couples' domestic violence, which is consistent with previous studies conducted by Ahmadzad-Asl et al. (10) and Peterman and Dixon (11). This can be explained by the idea that high levels of anxiety make couples more sensitive to both minor and major life events. As a result, couples may become more irritable and prone to reacting strongly to perceived improper behavior by their partners. This issue is aggravated when couples forcibly spend more time alongside one another throughout quarantine. Quarantine raises the couples’ interplays more than earlier, and high corona anxiety leads couples to misunderstand these interplays (33). Besides corona anxiety, quarantine itself can introduce financial stress, unemployment, social isolation, limited recreational activities, and increased anxiety, all of which can contribute to conflicts in couples' relationships. Therefore, anxiety can lead to misunderstandings and mental distress in couples, potentially escalating into aggressive behaviors toward their partners as a way to cope with this heightened anxiety.
The second significant finding supports the negative association between emotion regulation and domestic violence, which is consistent with the findings of Belyad et al. (16). To explain this finding, it can be argued that couples with better emotional regulation abilities tend to reevaluate situations when they experience negative emotions before reacting. They make an effort to change their perception or interpretation of the circumstances (34). This reevaluation process helps prevent them from experiencing intense negative emotions resulting from a faulty assessment of the situation. Consequently, they are less likely to exhibit aggressive behavior toward their partners. Additionally, couples with little ability to regulate their emotions use more emotional suppression, meaning that they repress their emotions in stressful situations. These unexpressed emotions may eventually manifest as psychophysical violence.
The final finding of this research demonstrated that increased distress tolerance is associated with lower levels of domestic violence. To explain this observation, it can be discussed that distress tolerance comprises a range of skills, including problem-solving, emotion regulation, and stress management (35). These skills are essential for constructive interactions between couples. Additionally, individuals require a certain amount of mental energy to use these skills effectively. According to the energy storage theory, individuals have a certain degree of mental energy that they use for skill utilization and event analysis. When faced with stressful life situations, such as the COVID-19 pandemic, individuals deplete a significant portion of their mental energy on anxiety. Consequently, they may have insufficient mental energy left for analyzing routine life events and interactions with their spouses due to the limitations of these resources (36). The lack of analytical capacity increases the likelihood of applying aggressive behaviors, particularly in the context of the couple's relationship. Therefore, coping skills related to distress tolerance help individuals conserve their energy when facing life stresses, enabling them to allocate it effectively when needed.
5.1. Conclusions
As a result, this study focused on couples who both experienced quarantine during the pandemic of the disease. Since there has been no prior research examining the relationship between the components of this study (corona anxiety, cognitive emotion regulation, and distress tolerance) regarding domestic violence in couples, our findings contribute significantly to this area of study.
However, our investigation had some limitations. The use of self-report questionnaires was one such limitation. Additionally, this study adopted a correlational research design, which prevented us from establishing causal attributions. Therefore, it is advisable to conduct intervention-based surveys to confirm these associations conclusively.
Another limitation of our research was its reliance on social networks for data collection, as conducting in-person studies was not feasible due to the COVID-19 outbreak. Consequently, our study sample was drawn from individuals available on these online platforms. For future research, it is recommended to explore other influential variables and conduct intervention-based surveys to mitigate domestic violence effectively.
