1. Background
According to the World Health Organization (WHO), tobacco use is responsible for the death of about six million people each year (1). There is a linear dose-response relationship between smoking and tobacco-related diseases such as cardiovascular disease (2, 3). It has been argued that about 65% of smokers intend to quit, which half of these attempts to quit at least once a year (4). A smoke-free work environment under the International Labor Organization’s (ILO) mandate can create healthy and safe workplaces (5, 6). Compared to 16 countries of the Eastern Mediterranean Region of WHO, Iran ranked sixth in workplaces smoking. Based on this report, Iran with a population of 26% smokers, ranked 33rd globally. Furthermore, it has been estimated that 11.7% of people (22.4% males and 0.8% females) start smoking approximately around the age of 15 in Iran (5, 6).
The risk of smoking for some diseases could be reversed, while for others the risk was approximately frozen at the point when smoking stopped (7). Some pieces of evidence claim that roughly 75% - 80% of smokers who have attempted to quit relapse within the first six months (8). Smoking cessation interventions are commonly influenced by theories and models of behavioral change, including the Transtheoretical Model (TTM) (9). Several studies have shown the effectiveness of TTM based educational interventions on smoking cessation (10-12). In fact, TTM enables us to design suitable interventions for the stages of change by which the smokers can increase their success for smoking cessation up to 39.5% (13-15). The stages of change consist of five, including pre-completion, completion, preparation, action, and maintenance (16). The TTM suggests designing interventions, which are appropriate for each stage of change among the individuals (17). This model consists of four constructs, including the stage of change (SOC), the processes of change (POC), self-efficacy (SE), and decisional balance (DB). The temptation to smoke is conceptualized to be inversely related to feelings of confidence and self-efficacy with regards to remaining abstinent from smoking (18).
2. Objectives
This study has aimed to evaluate the effectiveness of a designed TTM based educational program on smoking cessation among automobile factory workers in Bam, Iran.
3. Patients and Methods
The present interventional study was conducted on male workers who were working in an automobile manufacturing factory located in Bam city, Iran, from April 2017 to October 2017. The inclusion criteria were from 18 to 60 years of age, being motivated to quit smoking, having smoked at least 100 cigarettes at the beginning of the study, confirmed smoking habit by using exhaled carbon monoxide level test (measured by the Smoker lyzer Bedfont Pico instrument), and being able to read and write Farsi language. The exclusion criteria were suffering from or having a history of psychotic diseases, consuming psychotropic drugs, attending smoking cessation sessions before the study, having a history of any systemic diseases that encounter the study results and being reluctant to be studied. All procedures of the study were explained to the potential participants. The informed consent form was signed by them. Ethics Committee of Tarbiat Modares University approved the study (code no: 52D, 5608).
3.1. Intervention
Considering the need assessment of the participants that was done at the beginning of the study, the educational intervention was designed for four sessions, each session 45 minutes per person, based on TTM variables in which the educational program was conducted through lectures, discussions, and question/answer techniques. In the first and second sessions, the mechanisms of temptation construct of TTM for smoking were discussed. Therefore, during these two sessions, the ways through which participants were supposed to overcome temptation and to continue smoking cessation in addition to the ways for reducing obstacles of smoking cessation, and the techniques for replacing smoking with some healthy behaviors were assessed and discussed.
In the third session, the construct of change process was assessed. In this regard, self-awareness, self-reassessment, and self-release were discussed. The most important topics of this session included the ways of quitting smoking, the techniques for successful smoking cessation, assessing the reasons for failing to stop smoking, recapturing the reasons for deciding to quit smoking, reviewing the impact of being a smoker and how they currently feel after smoking cessation, setting short/long term goals for quitting smoking, being committed to short-term goals and the process of quitting. All these topics were assessed through discussion and question/answer techniques.
During the fourth session, the decisional balance of smoking cessation was mentioned. The main points of this session were the importance and benefits of smoke quitting, the barriers towards smoke quitting and solutions to remove mentioned barriers in order to achieve the goals. After completing the educational program, the participants were recommended to quit smoking at most the next two weeks. During the follow up period while smoking cessation happened, especially at the first days after the intervention, the recommendations for continuing smoking cessation, tempting situations and the likelihood of error and sliding back into smoking, nicotine dependence and signs of nicotine deprivation, stress induced by smoking cessation and the techniques to cope with this situation, as well as the importance of doing physical exercise were counseled with the participants through phone contacts. The interventional program was just applied for intervention group. However, both groups received routine messages for smoking cessation. In this study, the primary outcome was smoking cessation and the secondary outcomes were the TTM constructs of stage of change, temptation, process of change and decisional balance.
3.2. Measurements
To measure TTM constructs, the short form of TTM questionnaire was used. This 38-item questionnaire with 5 points Likert scale was developed by Prochaska et al. (19). This instrument consists of four constructs, including stage of change, process of change, temptation, and decisional balance. The Persian version of this instrument was confirmed and validated in the previous study (20).
Fagerstrom Test for Nicotine Dependence (FTND) was used to measure smoking cessation. Based on this questionnaire, if one smokes his first daily cigarette within the first 5 minutes, 6 to 30 minutes, 31 to 60 minutes, and after 60 minutes after waking up in the morning, she/he gets a score of 3, 2, 1, and 0, respectively. The reliability and validity of this questionnaire were evaluated/confirmed and validated in several previous studies in Iran (21, 22). The specificity and sensitivity of the Fagerstrom test have been 67.5% and 76.2%. This questionnaire was translated from English into Persian by two translators and back-translated by two independent translators. The translators were fluent in both English and Persian. They were all experienced healthcare professionals with many years of experience in the field. Then, having examined the questionnaire, the accuracy was confirmed by the research team and translators (21, 22).
3.3. Sample Size
To determine the sample size, the parameters of previous studies (23, 24) such as (α = 0.05, β = 0.1, effect size = 0.55, P1 = 33.3% and P2 = 2.7%) were considered, so the sample of 46.1 subjects for each group was calculated. However, considering (10%) for probable drop-out rate, the sample size increased to 51 subjects.
3.4. Sampling
To provide this sample size, multi-stage sampling was done. At first stage, from all eligible workers of the factory, 122 workers were selected through simple randomization and at the second stage, the 110 remaining eligible and willing workers were divided into two groups of intervention and control through random permutation blocking (55 AB, BA block) of every participant (each group included 55 workers). From each group, 5 participants were excluded due to not continuing the study or not complying with the study. Thus the study was completed by 50 participants in each group. Figure 1 shows the procedure of sampling. As the participants were provided with an ID code, the statistician who assessed the outcomes was blinded. However, because of the nature of the study the educator and participants were not possible to be blinded. Participants were enrolled, generated to random allocation sequence, and then assigned to the groups. The data were gathered from the participants in both groups at four-time points of the baseline, immediately post-intervention, 3 and 6-month follow-up.

Figure 1.
Follow diagram of the study is presented
3.5. Statistics Method
Chi-square test was used to compare the categorical variables and repeated measure ANOVA were utilized to compare parametric variables between the two groups. In this study, significant was determined statistically through P ≤ 0.05. In this study, SPSS version 21 was used for data analysis.
4. Results
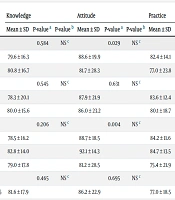
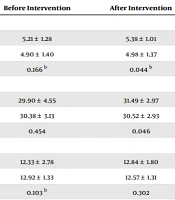
In general, 100 participants, including 50 individuals with a mean age of 30.90 ± 4.22 in the intervention group and 50 individuals with a mean age of 31.44 ± 3.55 in the control group completed the study. Table 1 shows demographic characteristics. There was no significant difference between the two groups at baseline (P > 0.05). Both groups were low smokers with regard to nicotine dependency (Fagerstrom Test) before the intervention. There was no significant difference between the two groups in terms of the smoking rate. The number of used cigarettes and the level of exhaled carbon monoxide in both groups at baseline indicated that the participants were not heavy smokers before the intervention (Table 1). Competition of TTM constructs (Table 2) shows significant differences between the two groups in terms of decisional- balance, temptation, and change processes, in three-time points of post-intervention, 3 and 6-month follow-up. However, there was no significant difference between the two groups in terms of these variables at the beginning of the study. Figure 2 shows the trend plot for these variables during the study in both groups. Table 3 indicates smoking cessation rate values and the stage of change of smoking cessation. According to this table, the smoking cessations were 18% and 4% in the intervention and control groups.
Table 1.
Demographic Characteristics of the Participants in Both Groups at Baseline
| Group Variable Number | Intervention (N = 50) | Control (N = 50) | P Value |
|---|---|---|---|
| Age (y)a | 30.90 ± 4.22 | 31.44 ± 3.55 | 0.574 |
| Average age of smoking start | 19.0 ± 3.05 | 18.36 ± 1.94 | 0.214 |
| Average duration of smoking | 5.44 ± 1.65 | 4.94 ± 1.83 | 0.158 |
| Educational level, No. (%) | 0.525 | ||
| Lower diploma | 7 (14) | 4 (8) | |
| Upper diploma | 43 (86) | 45 (92) | |
| Marriage status, No. (%) | 0.760 | ||
| Single | 7 (14) | 5 (10) | |
| Married | 43 (86) | 45 (90) | |
| Number of citrate using per day, No. (%) | 0.806 | ||
| ≤ 10 | 40 (80) | 39 (78) | |
| > 10 | 10 (20) | 11 (22) |
aValues are expressed as mean ± SD.
Table 2.
Comparison Between the Two Groups in Terms of Decisional-Balance, Temptation and Change Processes, at Four Time Points
| Group a | T | P Value (RM - ANOVA) | ||
|---|---|---|---|---|
| Control (N = 50) | Intervention (N = 50) | |||
| Decisional - balance | ||||
| Baseline | 22.6 ± 1.9 | 22.6 ± 2.7 | 0.04 | 0.9 |
| Immediately after the intervention | 22.73 ± 2.28 | 18.7 ± 2.2 | 7.4 | < 0.0001 |
| 3-month follow-up | 21.9 ± 2.2 | 18.2 ± 2.1 | 8.8 | < 0.0001 |
| 6-month follow-up | 22.2 ± 2.4 | 18.6 ± 1.9 | 8.1 | < 0.0001 |
| P value | F = 1.151; DF = (3, 147); P = 0.325 | F = 14.163; DF = (3, 147); P < 0.001 | ||
| Temptation | ||||
| Baseline | 33.9 ± 3.1 | 33.8 ± 2.8 | 0.2 | 0.8 |
| Immediately after the intervention | 32.3 ± 5.1 | 20.72 ± 3.01 | 13.8 | < 0.0001 |
| 3-month follow-up | 31.9 ± 5.09 | 24.04 ± 3.05 | 9.3 | < 0.0001 |
| 6-month follow-up | 32.6 ± 4.7 | 24.08 ± 2.6 | 11.09 | < 0.0001 |
| P value | F = 1.441; DF = (3, 147); P = 0.233 | F = 9.807; DF = (3, 147); P < 0.001 | ||
| Change processes | ||||
| Baseline | 70.7 ± 6.8 | 69.2 ± 9.08 | 0.9 | 0.4 |
| Immediately after the intervention | 70.9 ± 6.3 | 58.7 ± 5.9 | 10.08 | < 0.0001 |
| 3-month follow-up | 71.5 ± 6.88 | 60.5 ± 6.4 | 8.3 | < 0.0001 |
| 6-month follow-up | 72.3 ± 6.7 | 63.02 ± 6.4 | 6.9 | < 0.0001 |
| P value | F = 17.797; DF = (3, 147); P < 0.001 | F = 1.711; DF = (3, 147); P = 0.082 | ||
Abbreviations: RM - ANOVA, repeated measure analyze of variance; DF, degree of freedom; SD, standard deviation.
aValues are expressed as mean ± SD.
Table 3.
Cumulative Relative Frequency Distribution of the Study Groups in Terms of Smoking Cessation a
| Group | Preparation Stage | Action Stage | ||
|---|---|---|---|---|
| Baseline | Immediately After the Intervention | 3-Month | 6-Month | |
| Intervention | 50 (100) | 5 (10) | 7 (14) | 8 (16) |
| Control | 50 (100) | 1 (2) | 2 (4) | 2 (4) |
aValues are expressed as No. (%).

Figure 2.
The trend plot is shown for the variables during the study in both groups
5. Discussion
The results of this study showed after the intervention program, more participants were getting into the action-stage in the intervention group compared to another group.
This finding is in line with previous studies who reported successful cessation rate after education (25-27). This study could persuade a few people to quit smoking because in addition to improving beliefs there are many barriers to smoking cessation. A previous study revealed that barrios such as weight gain, craving a smoke, loss of pleasure, post-quitting stress, depression, and temptations interfere with smoking cessation (28).
This study showed that educational intervention improved the stage of behavior change, so more participants in the intervention group were ready to quit smoking. This was in agreement with other studies (23, 25, 29-32). Moreover, at the 6-month follow-up, the success rate of smoking cessation stage was significantly better than the control group, so more participants moved from preparation action stage. However, the previous study concluded that at the 6-month follow-up, few smokers had gone through fitness phase and stop smoking and there was a possibility of recurrence (20). Thus it seems that the success of the present study may be due to the interventions and the target group who were ready and motivated to quit smoking.
In this study, the temptation was reduced in the intervention group at different follow-ups that may be due to explaining the symptoms associated with smoking withdrawal and ways to deal with them. These results are consistent with previous studies (21, 23, 30, 33).
Furthermore, change processes score in the intervention group was more than the other group. The Narimani et al. study showed that empirical processes such as environmental reappraisal, and behavioral processes, such as stimulus control could lead to positive progress in the process of change in smokers (33). During the follow-up process, the subjects of the intervention group used more behavioral processes than the control group. Moreover, they used less cognitive processes, which are consistent with the expected pattern in the theory. According to the meta-theory pattern, individuals who quit smoking, stay in the stage of operation and reach the maintenance stage, use behavioral processes such as stimulus control, reverse conditioning, auxiliary relationships, and reinforcement management. However, individuals in the early stages of pre-thinking, thinking, and practice using more cognitive processes (34).
According to this study, perception of smoking cessation benefits in the intervention group was significantly better than the control group and adversely the barrier perception in the intervention group was lower than the other group. All these benefits might be due to the interventional program. These findings indicate that the intervention has been able to reduce the barriers, and increase the benefits of the cessation of smoking. Furthermore, the effectiveness of interventions remained stable up to six months after interventions. According to the pattern of the theory, it is expected that the intervention group becomes closer to the maintenance stage; the perceived disadvantages/perceived benefits of quitting smoking, the benefits/barriers and cost of smoking cessation to be decreased (15).
Educational programs can have immediate effects on the audience; therefore, they should seek the most effective methods with acceptable consistency, which the results of the study conducted by Rashidi et al. (35). However, this research showed that the designed theory-based education could be effective in progressing stages of smoking cessation.
5.1. Conclusions
Although the current manuscript concluded that TTM-based intervention program can be taken as an effective method for smoking cessation for smokers in the preparation stage, the findings should be evaluated in future studies with lower limitations.
5.2. Study Limitations
This study had several limitations such as conducting just among male workers, so the results may not be generalized to females. However, all smokers in the preparation stages were invited, and the census sampling methods were applied. The final limitation was the small sample size of the study.