In March 2020, the Iran government ordered a strict lockdown in reaction to the COVID-19 pandemic. A major disruption was made by the COVID-19 pandemic in different aspects, especially in routine hospital services all over the world (
9). In the interests of patient support and safety, elective surgery decreased during this pandemic (
10,
11). In otolaryngology, similar to other specialties, government protocol restricted surgery to emergencies (
12). It is noteworthy to mention that TO and AD are considered elective surgeries (
13).
The current study is the first one to evaluate the incidence rates of tonsillectomy, adenoidectomy, and ear surgeries before and during the COVID-19 pandemic in Iran. The results showed a significant reduction in surgery rates of TO, AD, and oto-surgery. However, there is no related study in Iran. Nevertheless, several studies all over the world have reported this significant issue (
8,
13,
14).
Those types of oto-surgeries that were not directly affected by COVID-19 were enrolled. It means it can be considered a control group. It is noteworthy to mention that the amount of this reduction was much more in TO and AD than in oto-surgery (control group). Additionally, this difference is observed in various months during the pandemic in the current study figures. It is known that the rate of all types of surgeries had a fall (
15) due to different factors, such as patients’ anxiety, lockdown, and government protocol about the cancellation of elective surgery (
16,
17). However, all of these factors affected all types of operation approximately the same. Therefore, "Why did the amount of reduction differ between AD and TO ones and oto-surgery?" is the main question.
Additionally, previous studies did not report any theory that can exactly explain why TO and AD differed (
13). It could be due to the one main reason for the tonsil and adenoid glands’ infection. Most surgical indications of tonsillectomy and adenoidectomy are directly due to the infection, such as recurrent tonsillitis, adenoiditis, otitis media, and abscess. Furthermore, most of the rest of the indications are indirectly related to the infection, such as obstructive sleep apnea (OSA) due to adenotonsillar hypertrophy and sinusitis (
18). This finding means that infection plays a key role in rates of TO and AD.
The infection rates that cause tonsilitis and adenoiditis have decreased during the COVID-19 pandemic. This could be the result of wearing masks, the closure of schools, and social distancing during the pandemic. It means that these factors filtered different viruses entering, such as viruses that are related to tonsilitis and adenoiditis plus the COVID-19 virus. Following this, the rates of TO and AD probably decreased during the pandemic. On the other hand, tonsils and adenoids are lymphoid structures, and there is an equilibrium between the local immunologic response of adenotonsillar tissue and their normal flora. Acute viral infection or its colonization can disrupt this equilibrium and finally lead to hypertrophied lymphoid tissue (adenotonsillar hypertrophy) (
19).
As mentioned previously, adenotonsillar hypertrophy can result in OSA as one of the surgical indications of tonsillectomy and adenoidectomy. Therefore, exposure to viruses can be reduced by wearing masks among many infected individuals during the pandemic. Following this, the risk of adenotonsillar hypertrophy decreased during the pandemic, and the rates of TO and AD were reduced. Some studies reported a reduction in the transmission of pediatric viral infections, such as otitis media (
20) and tonsilitis (
21). Moreover, their findings support the current study but are not certain.
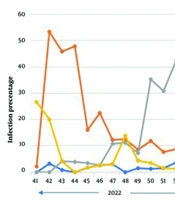
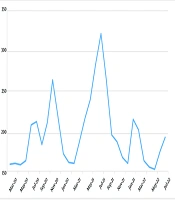
The findings of the present study revealed that all operations were reduced to near zero in the first peak. It was due to the public stress and heavy restrictions at the beginning of the pandemic. However, in the second and fifth peaks, the number of TO and AD was less than in the current control group. It could be the result of the season. In Iran, that season is summer, and schools are closed, and physical interaction is very low for children. This issue highlights the present study hypothesis. In addition, the findings of Alde M. et al.’s study support it (
20). However, its sample size is too smaller than the present study.
Generally, the rates of TO and AD dramatically declined during the peaks. In the third peak, the number of TO increased due to the nature of the season, and there was a cold atmosphere in Iran in autumn. Following this, the rates of upper airway infections were upwards. Again, in the 4th peak, a decrease occurred for all operations. However, it was more for TO and AD than the control group. It could be due to the virtual teaching of schools for children. Additionally, the months of the 4th peak are the best time for traveling in Iran. Therefore, many families traveled to different provinces, and the physical interaction was reduced.
The current study did not have any limitations except for some missing information about patients. It is suggested that future studies should be conducted on the pathophysiology of the present study hypothesis. Additionally, further studies could be better performed as clinical trials.
5.1. Conclusions
To sum up, the findings of the current study presented that the rates of TO, AD, and oto-surgery decreased significantly during the COVID-19 pandemic. However, this reduction was much more for TO and AD in comparison to oto-surgery. This difference proposes a hypothesis of the “impact of restrictions during the pandemic on the transmission of tonsillar and adenoidal glands infection among pediatric patients”.
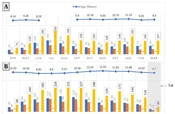





. A and B are related to ‘before COVID-19', and C and D are related to 'during COVID-19’. Each gray highlighted area presents one peak that is shown by the arrow and the number of peaks.")
. A and B are related to ‘before COVID-19', and C and D are related to 'during COVID-19’. Each gray highlighted area presents one peak that is shown by the arrow and the number of peaks.")
. A and B are related to ‘before COVID-19', and C and D are related to 'during COVID-19’. Each gray highlighted area presents one peak that is shown by the arrow and the number of peaks.")
.")