1. Context
The discovery and dissemination of the novel coronavirus disease 2019 (COVID-19) or severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) challenges the planet with a new public health crisis (1, 2). It has now spread to countries all over the world (1, 2). In 11 March 2020, according to the alarming levels of spread, severity and inaction, this outbreak was described as a pandemic by World Health Organization (WHO) (3). It is the first pandemic condition caused by a coronavirus (4).
According to findings of AAP, up to September 2020, children were responsible for 10% of cases in US (5).
Most of studies have reviewed the reported cases of COVID-19 in adults (6). Most important presentation of this infection in adults is pulmonary involvement that is far less severe in pediatrics. Reversely, in children there are lots of reports about multi-systemic involvement rather than adult patients and it seems that it is not possible to manage pediatric patients based on adult data; so to answer this paucity of evidences, this review tries to collect comprehensively expert opinions about both neonatal and paediatric groups in all aspects of the disease from epidemiology to prevention and treatment at the same time.
2. Methods
We searched databases including PubMed, Scopus, google scholar, and Medline. We reviewed more than 80 publications from December 2019 to mid-September 2020 with the most relevant articles about COVID-19 in children (up to 18 years old) included.
3. Results
Incidence and prevalence: In Wuhan, -the origin of COVID-19 outbreak-, the first confirmed pediatric patient was detected on January 28, 2020 (7, 8). Chinese Center for Disease Control and Prevention assessed that of 44,672 confirmed COVID-19 infection cases, about 0.9% occurred in children under the age of 10 years. Similar incidences were determined for individuals between 10 - 19 y/o. The incidence was 2.16% for people under 19 y/o (9). Based on a recent study in Wuhan, of 1391 children who were assessed for one month, a total of 171 (12.3%) were confirmed as COVID-19 (10). Similarly, in a study conducted by Qui et al. (11), of 661 COVID-19 cases, 36 (5%) were between 0 - 16 y/o and 28% of them were ≤ 5 y/o. Italian investigators stated that only 1.2% of the 22,512 Italian COVID-19 cases were children, with no deaths (3). From 4,226 COVID-19 cases in the United States, 5% were children, and they made up less than 1% of all hospitalizations in the country (12, 13). According to findings of AAP, up to September 2020, children comprised 10% of cases and 0.3% - 3.6% of all hospitalizations in US (5). It seems that prevalence of COVID-19 in children is much more than that imagined before. It may be due to their different symptoms, lack of consideration or due to the less severe course of the disease in children that leads to fewer laboratory assessment. This would be well defined now because of more availability of PCR test even for milder cases.
3.1. Age of Onset and Sex
Based on reported case series, this virus can infect children of all ages, from newborns to young adults. In a recent study by Lu et al. (10), the average age of infected children was 6.7 years. About 60.8% of pediatric cases were boys, 33.9% of patients were between 6 - 10 y/o, and 18% were under 12 months old. In a large Chinese pediatric case series of 2143 children, the average age was 7 years (14).
3.2. Transmission
Based on virus genome studies, SARS-CoV-2 originated from bats (15). The primary route of transmission thought to be through intermediate infected animals by contact or using animals’ products as food (16). According to WHO-China joint report, the transmission of SARS-CoV-2 is through droplets and household close contacts. However, during medical procedures like endotracheal intubation or removing endotracheal tube, administration of nebulized treatment, manual ventilation before intubation, open suctioning, turning the patient to the prone position, non-invasive positive-pressure ventilation and cardiopulmonary resuscitation, airborne transmission would be possible (17, 18). As infected population grows there is a bigger chance for children to get involved through household contacts (16). To this date, there is no report of confirmed fecal-oral transmission (17, 19). Xu et al. (20) observed that 8 of 10 children in their study continued to shed virus in their feces even after their nasopharyngeal specimen got negative for COVID-19. In a case report by Fan et al, nasopharyngeal and stool specimens of a 3 m/o girl with diarrhea and fever, were examined by real-time reverse transcriptase-polymerase chain reaction (RT-PCR) test for the COVID-19 repeatedly. They proposed the fecal-oral route as a possible threat to unaffected people, even up to one month after resolution of virus based on nasopharyngeal PCRs (21). Perinatal transmission of COVID-19 has been discussed later.
3.3. Sign and Symptoms
Symptoms of children with COVID-19 infection are usually less severe than that of adults. Based on Lu et al. (10) report of 171 confirmed pediatric cases, cough was the most common symptom (48.5%). Asymptomatic infection was reported in 15.8% of patients. Meanwhile, 19.3% of patients had upper respiratory symptoms and the most clinical feature in this study was pneumonia (64.9%). Fever was present in 41.5% of infected children. About 68% of the cases had a fever of < 38°C and only 16% had a fever of > 39°C. The median duration of fever was three days. Tachycardia and tachypnea were reported in 42.1% and 28.7% of cases, respectively. Another common symptom was pharyngeal erythema (46.2%). Diarrhea and vomiting were present in 8.8% and 6.4% of cases, respectively. O2 saturation < 92% during the hospitalization period, was detected in only 4% of the cases. Twelve asymptomatic patients showed radiologic features of pneumonia (8).
Chen et al. (22) reported the first case of severe pediatric pneumonia due to COVID-19 in a patient who experienced fever and respiratory distress followed by vomiting and diarrhea. This patient was intubated and received mechanical ventilation support and continuous venovenous hemofiltration; the patient eventually got better (22). Wu et al. (23) examined 74 infected children and found that only one patient had severe pneumonia. One-third of cases experienced cough and fever.
3.4. Comorbidities
In previous studies on adult population, it was suggested that COVID-19 is more frequent in people with underlying conditions (6). However, in studies performed on pediatric patients, the presence of underlying conditions was not prevalent. In two case series conducted in Iran and China, no underlying conditions were detected among pediatric patients diagnosed with COVID-19 (1, 24). In another study of 25 pediatric patients in Hubei, China, 23 (92%) of patients were previously healthy, while the other two patients suffered from congenital heart disease (25).
3.5. Diagnostic Criteria
The virus’s nucleic acid can be detected by RT-PCR assay (which is the most common technique of laboratory diagnosis), from nasal and throat swabs or from sputum, blood or stool samples. It also can be detected via viral gene sequencing (26). Viral culture is another route by which the microorganism can be isolated from human respiratory epithelial cells. Nowadays serological antibody screening kits are available in most of centers, although there are no reports in the literature regarding their routine use in children (26).
If a child had exposure to a confirmed COVID-19 patient within the last two weeks or came from a COVID-19 outbreak area, he/she is described as “high risk” of being carrier of the disease; of that, suspected cases are described when there are ≥ 2 of these criteria (14):
1) High temperature or respiratory or gastrointestinal symptoms or malaise;
2) Laboratory data: WBC count within normal or decreased range or lymphopenia or elevated level of erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP);
3) Abnormal chest imaging, including computed tomography (CT) scan.
The aforementioned diagnostic criteria are applied to children at low to medium risk, when all other serious respiratory infections, such as influenza virus, are ruled out.
Suspected ones that meet one of the following criteria are classified as proven cases (14):
1) Positive for COVID-19 nucleic acid in blood samples, nasal and pharyngeal swab specimens, as confirmed by an RT-PCR assay;
2) Genetic sequencing of samples taken from the respiratory tract or blood, which are highly similar to COVID-19.
3.6. Lab Tests
Some laboratory findings in adults include elevated inflammatory markers, such as ESR, CRP, increased liver enzymes, hyperglycemia, anemia, and high procalcitonin level (10). Data on laboratory markers in pediatric patients with COVID-19 is sparse. Lu et al. (10) found that lymphopenia was present in only 6 of 171 (3.5%) children with COVID-19. Henry et al. (27) reviewed the laboratory findings from 12 different reports. The authors reported normal leukocyte counts in 69.2% of the children and found that neutrophilia (4.6%) and neutropenia (6.0%) rarely occurred. Only 3.0% of cases had lymphocytopenia (27). Quite the reverse, in a review of adult patients, it was mentioned that elevated leukocyte and neutrophil counts were common during disease progression. Many of patients with alteration in leukocyte or neutrophil counts had no radiologic manifestations of pneumonia (28). Based on Wang et al. (29) study, only 30% of infants experienced lymphopenia. It might be due to the low prevalence of severe disease in pediatric patients (30). In a study on adult population, nearly 80% of critically ill patients and 25% of patients with mild disease had lymphopenia, suggesting that it may be linked to the severity of disease (31). Based on Henry review, procalcitonin and CRP were elevated in 10.6% and 13.6% of cases, respectively. There was no correlation between the severity of disease and serum levels of CRP or procalcitonin (27). Based on a meta-analysis in infected adults, procalcitonin rising might be associated with five-fold increase in risk of severe infection (32).
3.7. CT Scan
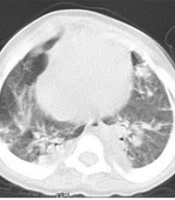
The reported CT manifestations of COVID-19 in pediatric patients are heterogenous. Some mild pediatric patients with COVID-19 had normal chest CT (33). The ground-glass opacity (GGO), mainly in peripheral and posterior of lungs even in subpleural area, is the most frequently reported finding in children exhibiting lung abnormalities (33-35).
Based on Lu et al. (10) study, the GGO was the most common CT scan feature in children with COVID-19 (32.7%), followed by local patchy (18.7%) or bilateral patchy shadowing (12.3%), and interstitial abnormalities (1.2%). Pleural effusion was not prevalent (1%). Also, 15.8% of children showed no signs of pneumonia or radiological characteristics of COVID-19 (2). Among 74 cases in Wu et al. (23) study, 37 cases (50%) had chest abnormalities in CT, including 30 patients with typical changes and 28 cases with atypical CT abnormalities. Remaining 50% of cases didn’t show any radiologic changes during the course of the disease (23).
Compared with adults, the GGO in COVID-19 pediatric patients were smaller and more localized; they also had lower attenuation, and less lobular involvement (34).
3.8. Death
In a study among 44,672 confirmed cases of COVID-19 from all age groups, the estimated death rate was 2.2%. There was 1 reported death in 10 - 19 y/o group, and there were no deaths among children aged under 9 (9). another death of a 14 y/o boy was described by Dong et al. (14). However, according to the “Chinese Center for Disease Control and Prevention” and “China’s Infectious Disease Information System” database, it seems that these two studies used the same data. Lu et al. (10) also reported a 10 m/o infant’s death tested positive for COVID-19 with intussusception accompanying multi-organ dysfunction as the clinical feature. up to March 18, 2020, Ludvigsson (2) reported two deaths in confirmed pediatric cases. Yousefzadegan et al. (36) reported three brothers, who died with same clinical features in Iran and they suggested the probability of a genetic predisposition to COVID-19 infection. In another study, none of 123 confirmed pediatric COVID-19 cases have died in the United States, however on March 28, the first infant death was recorded in Chicago, US (12). The overall death rate of children in US is 0% - 0.3% according to last update of AAP (5).
3.9. COVID-19 and Neonates
There is a debate on whether the COVID-19 virus can be transferred from an infected pregnant mother to her fetus. However, for the resuscitation of neonates born from COVID-19 suspected or confirmed mothers, medical workers must wear N95 masks, protective gowns, goggles, and head covers. Moreover, after confirmation of COVID-19 in the mother, the baby should also be isolated and tested (37, 38).
In one survey on 9 pregnant women, there was no vertical transmission to their infants (39). Fan et al. (40) could not find any evidence of COVID-19 infection in all conception products and newborns. In a recent report by Dong et al. (41), a neonate born to a documented COVID-19-positive mother had elevated antibody levels two hours after birth and exhibited abnormal cytokine test results. An elevated level of IgM antibody indicated that the neonate had been compromised in utero. Although becoming infected at the time of delivery cannot be excluded, IgM antibodies usually do not appear until some days after the initiation of the infection (41). Based on Fan et al. (40) study, two symptomatic pregnant women with positive COVID-19 RT-PCR test were examined and no virus was detected in their babies, umbilical cords, breast milk, vaginal swabs, placentas, or amniotic fluids. Thus, it was proposed that the risk of intrauterine infection is very low (40).
In another report by Chen et al. (42), 72 hours after birth PR-PCR tests of all three infants born to documented COVID-19 positive mothers were negative and none of them became symptomatic. Reversely in a recent study by Farsi et al. PCR from 1 of 3 neonates of a triplet pregnant infected mother got positive in day 3 after birth and the other 2 died with pulmonary involvement unexpected by RDS and proposed that maybe they were infected in uterus.
Treatment of symptomatic neonates consists of oxygen, correction of fluid and electrolyte disturbances to prevent over-hydration to inhibit pulmonary congestion and oxygen desaturation (43). In neonates with severe acute respiratory distress syndrome, high‐frequency oscillatory ventilation, inhaled nitric oxide, high‐dose pulmonary surfactant, and extracorporeal membrane oxygenation might be helpful (43).
3.10. Multisystem Inflammatory Syndrome in Children (MIS-C)
This syndrome is presented with fever ≥ 3 days, fatigue, inflammatory markers elevation and various signs of multiple organ (≥ 2) involvement (gastrointestinal, cardiac, renal, neurologic, dermatologic and hematologic). Positive diagnostic tests for current COVID-19/suspected exposure and lack of any other possible diagnosis are another 2 necessary criteria for confirmation of this syndrome (44, 45). Inflammatory markers defined as: elevation of CRP, ESR, fibrinogen, procalcitonin, d-dimer, ferritin, lactic acid dehydrogenase (LDH), interleukin 6 (IL-6), or neutrophils, and reduced lymphocytes and/or albumin (46), MIS-C could be present in children without any COVID-19 early stage’s manifestation or might be present several weeks after infection (44). Studies showed that most MIS-C patients improved with immunomodulatory drugs, most commonly IVIG and systemic glucocorticoids (47). Feldstein et al. (48) showed that IL-6 inhibitors, IL-1 inhibitors and anticoagulants were needed in 1%, 5% and 14% respectively. Health care providers of patients younger than 21 y/o who meet any MIS-C criteria, should report it as suspected case to the local, state, or territorial health department.
3.11. Treatment
Due to the increasing number of people infected with the SARS-CoV-2 and its potentially threatening characteristics, a competent treatment protocol is needed. It seems that prompt interventions for recognition, isolation, diagnosis, and treatment are basic principles.
3.11.1. General Management
Providing sufficient isolation to inhibit transmission to family members, other patients, and healthcare workers is necessary (20, 43). Symptomatic support is the main treatment modality of SARS-CoV-2 infection (2, 49, 50) and consists of the following general policies: Bed rest, sufficient water and calorie intake, fluid and electrolyte balance, analgesia, antipyretics, vital signs and oxygen saturation monitoring, and respiratory support (3, 23, 51-54). In case of hypoxia, all studies recommend to keep patency of airway and providing supplemental oxygen with nasal cannula/mask (24, 49, 51, 53, 55, 56). For management of persistent respiratory distress despite nasal oxygenation, it is proper to use heated humidified high-flow nasal cannula (HHHFNC], continuous positive airway pressure (CPAP), mechanical ventilation, and extracorporeal membrane oxygenation support (ECMO) if necessary (24, 49, 51, 53, 55, 56). Shen et al. (55) declared that when there is no improvement after two hours of non-invasive mechanical ventilation (NIV), severe coughing, increased airway secretions or unstable hemodynamic state, invasive mechanical ventilation (MV) should be implemented quickly. To decrease ventilator-related lung injury, lung-protective protocols with low tidal volume have been emphasized.
Treatment with approved and existing drugs seems to be the fastest technique for management of COVID-19 patients (2). There is no specific drug trial for use in children and no drug has been approved for COVID-19 in children yet (2, 57). Special therapy hasn’t been indicated for all patients. According to the severity of the disease and patient’s risk factors, treatment is selected to administer antiviral agents alone or in combination with immunomodulators and watchful follow up to consider ICU admission (24). Based on a multicenter initial instruction on applying antivirals for infected children, patients were divided into three categories (58):
1) Mild-Moderate (Cases Who Don’t Require Supplemental Oxygen): The management consists of supportive care and no antiviral agents are required at this level.
2) Severe (Cases Who Require Supplemental Oxygen but Not NIV or MV): At this stage, supportive care alone is appropriate for the majority of children. Although use of antivirals could be considered in some cases, it should be given preferably as part of a clinical trial if available.
3) Critical (Cases Who Require NIV or MV, OR There is Sepsis, Multi-Organ Failure or Rapidly Worsening of Clinical Status): Use of potentially active antivirals should be considered, preferably as part of a clinical trial.
Treatment staging in Iran’s protocol is shown below as an example (52):
1) Mild/moderate pneumonia without risk factors: Any outpatient treatment was not recommended.
2) Mild/moderate pneumonia with risk factors (chemotherapy, malignancies, treatment with corticosteroids, underlying pulmonary disorders, hypertension, and body mass index >40): Hydroxychloroquine + antiviral agent (Atazanavir/ritonavir or atazanavir or lopinavir/ritonavir) and antibiotics (ceftriaxone + vancomycin) based on the patient’s clinical status.
3) Sever pneumonia (ICU admitted patients): same as group 2. Antibiotics (vancomycin + meropenem) based on the patient’s clinical status.
3.11.2. Medical Treatments
Some of the most common pharmaceutical dosages (and their precautions) are mentioned in Table 1 (51, 52, 54, 55).
| Drug | Dosage Recommendations in Children with COVID-19 | Considerations | Drug | Dosage Recommendations in Children with COVID-19 | Considerations |
|---|---|---|---|---|---|
| Kaletra (Lopinavir/ Ritonavir) | -14 days to 12 months: 300 mg/m2* or 16 mg/kg (based on lopinavir component), twice daily, orally. 12 months to 18 years: 230 mg/m2 (based on lopinavir component) twice daily, orally (maximum dose: lopinavir 400 mg/dose and ritonavir 100 mg/dose, twice daily); based on weight: 7 - 15 kg: lopinavir/ritonavir 12 mg/3 mg/kg, twice daily, orally. 15 - 40 kg: lopinavir/ritonavir 10 mg/2.5 mg/kg, twice daily, orally. > 40 kg: lopinavir-ritonavir 400 mg/100 mg tablet, twice daily, orally. For 5 - 14 days, based on clinical improvement. | Kaletra should not be used in neonates before 42 weeks of gestation and postnatal age of at least 14 days. | Remdesevir | ≥ 40 kg: single loading dose of 200 mg on day 1, followed by maintenance dose of 100 mg once daily. 3.5 kg to < 40 kg: single loading dose of 5 mg/kg on day 1, followed by maintenance dose of 2.5 mg/kg once daily. | Administer remdesivir as IV infusion over 30 - 120 minutes. treatment duration based on disease severity and clinical response; treatment recommended for 10 days in patients who require invasive mechanical ventilation or ECMO. Five days in patients who do not require invasive mechanical ventilation or ECMO. |
| Ribavirin | < 47 kg: 15 mg/kg/day, twice daily, orally. 47 - 59 kg: 400 mg, twice daily, orally. 60 - 73 kg: 400 mg- in the morning, 600 mg- in the evening. > 73 kg: 600 mg, twice daily, orally. For up to 14 days, based on clinical improvement. | In children over 3 years of age. | Hydroxychloroquine | Infants and children: 3 - 5 mg/kg/day (maximum dose: 400 mg), twice daily, orally for 5 days. | QT interval prolongation, ventricular arrhythmias and torsade’s de pointes reported notably in concurrent use with Kaletra; hydroxychloroquine should be used with more caution in history of ventricular arrhythmias, bradycardia, hypokalemia and/or hypomagnesemia. In high-risk conditions, it can be used as a single dose. Cardiac monitoring is recommended. |
| Ribavirin | < 47 kg: 15 mg/kg/day, twice daily, orally. 47 - 59 kg: 400 mg, twice daily, orally. 60 - 73 kg: 400 mg- in the morning, 600 mg- in the evening. > 73 kg: 600 mg, twice daily, orally. For up to 14 days, based on clinical improvement. | In children over 3 years of age. | Oseltamivir | Term infants up to 12 months: 3 mg/kg/dose, twice daily; children over 12 months based on body weight: < 15 kg: 30 mg, twice daily > 15 - 23 kg: 45 mg, twice daily > 23 - 40 kg: 60 mg, twice daily > 40 kg: 75 mg, twice daily. Adults 75 mg, twice daily for at least 5 days. | In infants with a history of prematurity consult with a pediatric infectious diseases specialist. |
| Methylprednisolone | 1 - 2 mg/kg/day for 3 - 5 days. | Interferon-α | -nebulization: 100,000 - 200,000 IU/kg in mild cases, 200,000 - 400,000 IU/kg in severe cases, Two times/day for 5 - 7 days. spray: 1 - 2 puffs on each nostril and 8 - 10 puff/day on the oropharynx. For 5 - 7 days. | ||
| Intravenous immunoglobulin (IVIG) | 400 mg/kg/day for 5 days or 1.0 g/kg/day for 2 days |
Antiviral Compounds: Some (but not all) studies recommend antiviral treatment (7, 59). Antiviral treatments were broadly used in severe cases. Two drug groups were widely used (2, 23, 25, 53, 55, 57, 59):
1) Enzyme inhibitors, such as remdesivir, lopinavir, favipiravir, ribavirin, and sofosbuvir.
2) Inhibitors of SARS-CoV-2 entrance into the cell, such as Camostat, hydroxychloroquine (or chloroquine), Oseltamivir, umifenovir, and baricitinib.
FDA issues emergency use authorization (EUA) permit use of remdesivir for emergency in suspected or confirmed COVID-19 in hospitalized children/adults with severe disease (62).
Immunomodulators: Some immunomodulators have been applied for treatment of patients with SARS-CoV-2:
1) Corticosteroids: The role of corticosteroids is still unproven, and most studies advise against their use (7, 53). Some recommend administering short-term and low-to-moderate dose of corticosteroids in severe and critical cases (25, 53, 61). Chen et al. (51) stated that corticosteroids use should be limited to the following situations: (1) ARDS and rapid worsening of the chest imaging abnormalities; (2) serious conditions like hemophagocytic syndrome, encephalitis or encephalopathy; (3) septic shock; (4) wheezing.
2) Interferons: Reduction in viral loads, decreased symptom severity and course of disease shortening were reported in cases treated with interferon-α (2, 23, 51, 53). It is available in nebulizing and inhaler forms, and the prescription dose is based on previous recommendations of its use in treating bronchiolitis, viral pneumonia, and other viral infections in children. Interferon-α is a safe and effective option among the other recommended treatments for COVID-19 in children (55).
3) Monoclonal Antibodies: Fu et al proposed that IL-6 is linked to the inflammatory storm that contributes to severe COVID-19 cases. Tocilizumab as a monoclonal antibody targets the IL-6 receptor and therefore may decrease the inflammatory storm and reduce the mortality rate (63, 64).
4) Thymosin: This agent can improve the immune responses in SARS patients and relief spreading virus limitation (65). Despite lack of benefit of thymosin alpha-1 in COVID-19 treatment, it has been recommended to increase the cellular immunity as well as to reduce cytokine storms (66).
5) Passive Immunization and Intravenous Immunoglobulin (IVIG): The plasma of recovered patients and Gamma globulins are proposed as a possible treatment. Meanwhile, trials of these therapeutic interventions, is currently restricted to severe cases and their efficacy needs to be confirmed (49, 55, 61).
Antibiotics/Antifungals: It is recommended to use antibiotics and antifungals only in the probability of superinfection or co-infection (2, 51, 53, 67).
Other Medications: Ji et al. (68) reported the use of an oral probiotic in one case with mild diarrhea and disappearing the symptoms after two days of this prescription. Some studies proposed recommendations about using traditional Chinese herbs (53). But due to lack of data, it needs to be further verified.
Blood Purification: Continuous blood purification should be proposed in cases of multiple organ dysfunction (especially acute kidney injury), volume overload or serious conditions like severe water and electrolyte imbalances. It should be administered cautiously (51).
3.11.3. Discharge
It is recommended to discharge the patient from hospital by fulfilling all criteria listed below (3, 55):
1) Normal body temperature for three days.
2) Apparent improvement of respiratory symptoms.
3) Two negative SARS-CoV-2 tests (at least one day apart).
4. Discussion
Since December 2019, COVID-19 infections have spread rapidly all around the world. In the primary reports, all affected patients were adults. Pediatric patients and neonates were subsequently reported. According to the latest reports, 1% - 5% of the infected patients were under the age of 19 years. Deaths in this age group were rare, but it can occur in children with severe disease (16, 31, 51, 69).
As we mentioned in this review, the symptoms of infected children tend to be milder than those of adults. This may be related to host factors and exposure (31). Several hypotheses could explain this:
1) Children tend to have recurrent exposure to different viral infections. It is presumed that these viral episodes make their immune system more potent during an encounter with COVID-19 virus (2, 70).
2) It is also suggested that the S protein of this virus binds to the angiotensin-converting-enzyme (ACE) 2 on the host cells surface. Therefore, children may be protected against COVID-19 because this enzyme is less mature in children (14, 71).
3) Children are usually well-looked-after at home and have fewer chance of being exposed to people who are infected with this virus (14).
The median age of children who were infected with this virus is seven years (ranging from 1 day to 18 years). This indicates that children of all ages are vulnerable to this infection (13, 14, 39, 57). Children seem to have fewer symptoms than adults, but they are still likely to transmit the disease to healthy individuals (16).
Not commonly but severe and critical cases can occur especially in children with underlying diseases (24). Therefore, these children should be isolated as much as possible (25).
In adults’ studies, lymphocytopenia is a common laboratory test finding. In Guan et al. (6) study on 1099 patients, the rate of lymphocytopenia was 83.2% but only 9 of them were children. These findings are in contrast to the data presented in studies on children, where only 3% - 4% had lymphocytopenia. CRP and procalcitonin levels are often normal in pediatric patients. This phenomenon may be related to the lower severity of disease in pediatric population (10, 27, 28, 32).
Chest CT scan findings in COVID-19 pediatric patients are nonspecific and milder than in adults and some of them have normal chest CT. Main abnormalities include small bilateral multiple ground-glass opacities and/or infiltrating shadows in the middle and outer zones of the lungs. Compared with adults, the ground-glass opacities in children with COVID-19 infections are smaller and more localized, they show lower attenuation, and less lobular involvement (6, 23, 33, 34, 43).
The chance of vertical transmission from an infected pregnant mother to fetus has not been proven yet (40, 42).
Due to the potentially threatening characteristics of SARS-CoV-2, a competent treatment protocol is needed. Conservative and symptomatic management is the cornerstone of SARS-CoV-2 infection treatment (2, 49-52, 54). There is no approved drug for children yet (52, 59). Furthermore, special therapy is not indicated for all the patients, and the treatment stage will be selected from watchful waiting programs and follow-up of the administration of antiviral agents alone or in combination with immunomodulators and ICU admission (52, 55, 56, 59).
In summary, The COVID-19 disease characteristics in children are not yet fully established, which poses a significant problem for pediatric medical staffs. Special consideration should be given to children because they are a special group of patients. Most of them are asymptomatic or have mild symptoms. Critical condition is uncommon unless in children with underlying diseases. To overcome this disease, especially in these vulnerable patients, more appropriate preventive measures and treatment policies should be provided.