




1. Background
The universal newborn hearing screening enables the early detection of congenital hearing loss. In this regard, OAEs and AABR, as two safe and equally accurate techniques, are used to conduct hearing screening for newborns (1).
The recommended screening time to detect any hearing loss is within the first three months of life (2). A study showed that the referral rate of one-step OAE was about 5.8% (3); however, the combination of OAE and AABR resulted in a significantly decreased referral rate (3-5).
False-positive test results often arouse anxiety in mothers (6). Delaying the first screening and retests increased the pass rate (7). In other words, delaying screening time reduced the referral rate; however, it may not be practical in all settings (7).
The confirmation of appropriate hearing screening time can reduce the number of tests, thus decreasing the imposed economic costs. Moreover, parents' anxiety may be relieved, and a close parent-child relationship can be established following a definite hearing test. However, few studies have examined the hearing screening time, especially in China.
2. Objectives
In this study, we analyzed the referral rate of non-high-risk newborns in our center from June 2011 to June 2018 to detect an appropriate rescreening strategy and time points for newborns who need hearing rescreening.
3. Methods
3.1. Patients
The retrospective study included the newborns screened in our center from June 2012 to June 2019. According to the Joint Committee of Infant Hearing 2007 (JCIH), all newborns with one or more risk factors were excluded, and 2493 newborns having undergone secondary screening for congenital hearing loss using the OAE and/or AABR techniques were included in the study. Regarding the examination day, the participants were categorized into five groups: (1) < 42 days, (2) 42 - 56 days, (3) 57 - 70 days, (4) 71 - 84 days, (5) > 84 days. Our study was approved by the Local Ethics Committee (code. 20120106), and the informed consent was obtained.
3.2. Testing Equipment
Screening was performed by experienced audiologists. Distortion product otoacoustic emission (DPOAE) was also measured using the GSI 70 automated OAE screener system (GSI Audera, USA, and an AABR test was conducted using the MB11 AABR screener (MAICO, Germany). A 35-dB nHL alternating polarity click was used to evaluate the response of the auditory nerve.
3.3. Statistical Analysis
SPSS software version 19.0 was used to analyze the data, and the SNK test was used to compare the hearing screening performance among the groups. P < 0.05 was set as the level of significance.
4. Results
4.1. Participants’ Features
From June 2012 to June 2019, 2493 newborns without no high-risk factor confirmed by JCIH underwent the hearing screening test in our center. OAE was performed 24 - 48 hours after birth, and the following results were achieved: (1) 119 cases (4.7%) passed the left ear screening test; (2) 138 cases (5.5%) passed the right ear screening test; (3) 107 cases (4.4%) failed the screening test of both ears; (4) 2129 cases (85.4%) passed the screening test of both ears.
4.2. Total Referral Rate of Newborns’ Hearing Screening
Among 1366 newborns undergoing the OAE test, the total referral rate was 13.1%; however, the total referral rate was 16.5% for 1127 newborns undergoing both OAE and AABR tests.
4.3. Referral Rates of Newborns’ Hearing Screening By Different Examination Days
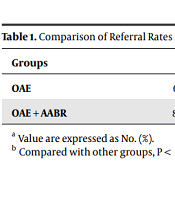
Newborns with no high risks underwent OAE during 42 days, and their referral rate was 14.8 %. Moreover, the referral rates for those who underwent the test during 42 - 56 days, 57 - 70 days, 71 - 84 days, and > 84 days were 10.1, 13.2, 13.9, and 13.5%, respectively (Table 1).
Newborns with no high risks underwent OAE+AABR during 42 days, and their referral rate was 20.2%. Moreover, the referral rates for those who underwent the test during 42 - 56 days, 57 - 70 days, 71 - 84 days, and > 84 days were 11.6, 17.1, 18.1, and 14.1%, respectively (Table 1).
The referral rate for those who underwent OAE and OAE+AABR was the lowest in the 42 - 56-day group compared to the other groups (P < 0.05).
5. Discussion
Many diseases need to be examined and detected as early as possible (8-10). The delayed diagnosis of hearing impairment may have serious harmful effects on the development of newborn’s language, social, emotional, cognitive, academic, and vocational abilities (11). Accordingly, the early detection of congenital hearing loss by using a universal newborn hearing screening test is of paramount importance.
Compared to OAE, the AABR test requires more knowledge and expertise to be performed. Moreover, more time and higher economic costs were associated with AABR than OAE (12). Accordingly, the initial screening in China has been performed using the OAE test. As described in the guidelines on the examination and intervention for infants, the second screening in China is recommended to be 30 - 42 days after birth (13). The target population of the second screening are newborns who fail the initial screening or have high-risk factors. This is, while the screening strategy and time are still controversial. No previous study explored the correlation between screening time and the referral rate. We selected a two-week interval to compare the referral rates at different time points because our preliminary experiment revealed one-week or one-month intervals to be inappropriate. The one-week interval was too short, while the one-month interval could also affect the referral rate.
Our previous study showed that delaying the screening time (> 57 days) may reduce the referral rate in newborns with high-risk factors (14); hence, we concentrated on newborns with no high-risk factor in this study. The findings showed that the referral rate of the first screening was only 14.6%. For the second screening, the referral rates of those undergoing OAE and OAE + AABR were 13.1 and 16.5%, respectively, implying that only a small number of the participants may need intervention.
As JCIH suggested, each country should draw up its protocol according to local government’s decisions and budget (2). After comparing different screening techniques, we noticed that the referral rate of the two screening techniques was the lowest in the 42 - 56-day group, implying that delaying the screening time (42 - 56 days) may lower the referral rate and result in higher cost-effectiveness. However, the referral rates in the other groups showed no significant difference, suggesting that the auditory system is well-developed, and the referral may be due to irreversible damage to the auditory system. We also found out that the referral rate at intervals longer than 56 days was higher than those at 42 - 56-day intervals. This may be explained by the fact that some parents refuse to have further consultation as they believe that their children are normal and respond well to sounds.
The JCIH guidelines suggest that the referral rate of an acceptable UNHS program should be < 4% (2). As discussed in previous studies, the main reasons leading to the false-positive results of the OAE testing were ear canal collapse and the debris in the external auditory canal, amniotic fluid or mucus in the middle ear, and ambient noise (7). Such content is often restored within the first few hours or days of life, and the pass rate will be higher if more than one OAE test is performed. Lower frequencies (1 - 4 kHz) adopted in the OAE tests were another factor leading to the high referral rates (7). In contrast, tests with higher frequencies contribute to lower referral rates as the presence of liquid and debris has less effect on the outcome (7, 15). IN general, both developmental and environmental factors may affect the hearing test results and lead to false-positive or false-negative results. Accordingly, audiologists should reduce the intervention caused by the tested ear, test machine, or test environment as much as possible.
The present study first explored the correlation between the examination day and the referral rate of secondary hearing screen among non-high-risk newborns; however, this study had some limitations: (1) the confirmed outcomes of newborns were not evaluated because our study focused on the screening strategy; and (2) this study was a one-center study with a small sample size.
5.1. Conclusion
Despite the aforementioned research limitations, the present study suggested that the delay in newborn rescreening by 42 - 56 days after birth may result in a lower referral rate, which would have remarkable consequences for policymakers. Further studies are recommended to address diagnostic hearing tests to triangulate the present findings.
