


1. Background
Malnutrition, as one of the common problems in today’s societies, occurs when a person gets too much or too little of certain nutrients. This condition has clinical consequences for malnourished individuals and exerts adverse effects on their body shape and function (1). On the other hand, dental caries is a common preventable chronic disease worldwide, resulting from an imbalance in demineralization and remineralization of the dental hard tissue. Early childhood caries (ECC) is the most common chronic childhood disease. It is defined as “the presence of one or more decayed (non-cavitated or cavitated), missing (as a result of caries), or filled tooth surfaces in any primary tooth in a child 71 months of age or younger” (2). Although ECC is not a fatal disease, it has significant effects on the person’s self-confidence, eating habits, and overall health (3).
Some evidence suggests that malnutrition, especially protein-energy malnutrition, increases the risk of ECC. Common risk factors appear to increase the prevalence of both ECC and malnutrition. These conditions seem to be correlated and often occur concurrently in individuals. Therefore, ECC can result in the reduced growth rate of children (4). However, the presence of confounding variables, such as diet and socioeconomic status, besides underlying factors, such as age, health status, and dietary fluoride intake, makes it difficult to make a definite conclusion about the relationship between these two conditions. Overall, it is evident that some nutritional habits and malnutrition affect the incidence of ECC due to their undeniable effects on the secretion and composition of saliva (5).
The body mass index (BMI) is an accepted index for assessing a person's body weight relative to height (6). Many studies have investigated the relationship between BMI and ECC in deciduous and permanent teeth and reported different results. Some of these studies demonstrated a positive relationship between BMI and caries in deciduous teeth (7); some showed an inverse relationship (8-10); and some revealed no significant relationship (11). In this regard, two studies by van Gemert-Schriks et al. (12) and Alkarimi et al. (13), examining the effect of dental treatment on children’s growth and development, revealed no significant difference in the anthropometric markers of children, who received comprehensive dental treatments and those who did not. However, in a study by Sachdev et al. (14), comprehensive full-mouth rehabilitation was observed in the catch-up growth of children with severe ECC.
2. Objectives
Regarding the contradictory results of previous studies and the cross-sectional design of most of these studies, we aimed to investigate the relationship between BMI and ECC in this case-control study and to determine the effect of dental treatment on the BMI changes of Iranian children, aged 3 - 6 years.
3. Methods
In this longitudinal case-control study, three groups were included: children diagnosed with ECC receiving treatment (group I); children diagnosed with ECC without treatment (group II); and caries-free children, with no ECC (group III). In this study, our main goals were to determine BMI changes in group I, group II, and group III and to compare BMI changes in each group.
3.1. Study Population
Based on the sample size formula (α = 0.05, 80% power, and 10% error rate), a total of 96 children were examined in three groups (n = 32 per group). The study population consisted of 64 children (aged 3 - 6 years) from preschool centers, who were selected by cluster random sampling (group II and III), in this way that 24 children were selected from District 1 of Zahedan, which has 71 preschools. Six preschoolers were randomly selected and from each preschool 4 children were selected who were two girls and two boys. Also 40 children were selected from District 2 of Zahedan, which has 99 preschools. Ten preschoolers were randomly selected and from each preschool 4 children were selected who were two girls and two boys. as well as 32 children (aged 3 - 6 years), referred to a pediatric dentist for a comprehensive dental treatment under general anesthesia (with a minimum of eight severely decayed teeth and at least four teeth with pulpal involvement), selected by convenience sampling (group I).
Pulpal involvement was confirmed by clinical examination and radiography. The children were matched in terms of age and gender in the three groups. This study was conducted from May 2017 to February 2018. The inclusion criteria were as follows: (1) absence of a systemic disease; (2) parental consent; (3) child’s cooperation; and (4) similarity of socioeconomic status (medium level of education and economic income).
This study was approved by the Ethics Committee of Zahedan University of Medical Sciences (code: IR.ZAUMS.REC.1396.49).
3.2. Methods and Measurement Tools
Initially, the importance of the study was explained to the children’s parents. If they consented to their child's participation in the study, they were asked to sign an informed consent form. A questionnaire, including the child’s age and gender and the parents’ education level, occupation, and monthly income, was completed by the parents. Next, a dental examination was performed by a trained senior student to determine the decayed, missing, and filled teeth (DMFT) index for each child, using a disposable mirror and explorer, as well as a headlight.
Dental caries was diagnosed according to the World Health Organization (WHO) criteria (WHO, 1997). Next, the children's height was measured using a tape meter with 1 mm precision (Arka, Taiwan), and weight was measured in kilograms (with light clothes and no shoes), using a PS25 digital scale with 100 g precision (Beurer, Germany) by a trained nurse, who was unaware of the study interventions. BMI was also calculated and recorded by dividing weight by the square of height. The BMI percentile was then calculated for each child, according to standard tables relative to age and gender (15). After six months, BMI and DMFT index were re-measured. All measurements were performed in the same manner at both baseline and follow-up. Any changes in BMI and DMFT index were recorded in the follow-up. The BMI changes were considered as any statistically significant difference in the recorded BMI series.
Since some children were likely to be excluded from the study due to non-attendance of follow-up or treatment session, 35 children were examined in group I, all of whom attended the follow-up session; therefore, the last three children were excluded from the study. In group II, 43 children were examined, 11 of whom were excluded due to treatment or non-attendance of the follow-up session. Possible reasons why other children in group II have not been treated include: Parental neglect, financial problems and lack of insurance coverage for dental services. Finally, in group III, 38 children were examined; however, three children had tooth decay, and three did not attend the follow-up. The sample size was finalized after excluding illegible children.
3.3. Data Analysis
Data were analyzed using SPSS version 20. Independent t-test was used to compare BMI between genders, and Mann-Whitney U test was used to compare ECC between males and females. Also, ANOVA and Kruskal-Wallis tests were used to compare BMI and ECC in children of different ages, respectively. Moreover, to compare the BMI of each group at two different intervals (data with a normal distribution), paired t-test was used, while ANOVA test was performed to compare the BMI of the three groups (data with a normal distribution). All tests were performed at a P-value less than 0.05 (95% confidence interval).
4. Results
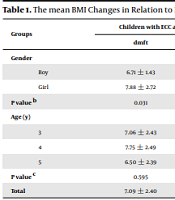
In this study, 96 children, aged 3-6 years, were examined in three groups. Group I consisted of 32 children (14 boys and 18 girls), diagnosed with ECC, who received a comprehensive dental treatment under general anesthesia; group II consisted of 32 children (15 boys and 17 girls) diagnosed with ECC, who did not receive any treatment during six months; and group III consisted of 32 caries-free children without ECC (17 boys and 15 girls). The mean DMFT index values at baseline were 7.09 ± 2.40 and 5.19 ± 1.72 in groups I and II, respectively. Table 1 presents demographic characteristic of children and the mean changes of BMI with respect to gender and age in the three groups after six months.
| Groups | Children with ECC and Treatment (First Group) | Children with ECC and Without Treatment (Second Group) | Caries Free Children (Third Group) | |||
|---|---|---|---|---|---|---|
| DMFT | BMI Changes (kg/m2) | DMFT | BMI Changes (kg/m2) | DMFT | BMI Changes (kg/m2) | |
| Gender | ||||||
| Boy | 6.71 ± 1.43 | 0.181 ± 0.450 | 5.60 ± 1.99 | 0.023 ± 0.491 | 0 | -0.0212 ± 0.683 |
| Girl | 7.88 ± 2.72 | 0.155 ± 0.361 | 4.81 ± 1.37 | -0.011 ± 0.311 | 0 | -0.068 ± 0.616 |
| P value b | 0.031 | 0.163 | 0.208 | 0.588 | 0 | 0.841 |
| Age (y) | ||||||
| 3 | 7.06 ± 2.43 | 0.151 ± 0.393 | 5.10 ± 1.66 | 0.111 ± 0.486 | 0 | -0.232 ± 0.674 |
| 4 | 7.75 ± 2.49 | 0.200 ± 0.462 | 5.60 ± 1.57 | -0.009 ± 0.335 | 0 | 0.048 ± 0.406 |
| 5 | 6.50 ± 2.39 | 0.108 ± 0.382 | 4.90 ± 1.97 | -0.072± 0.382 | 0 | 0.093 ± 0.791 |
| P value c | 0.595 | 0.593 | 0.657 | 0.575 | 0 | 0.575 |
| Total | 7.09 ± 2.40 | 0.118 ± 0.425 | 5.19 ± 1.72 | 0.0050 ± 0.399 | 0 | -0.043 ± 0.643 |
The mean BMI Changes in Relation to Demographic Characteristics in Study Groups After the Six Months a
As shown in Table 2, the mean BMI changes were 0.11 ± 0.42, 0.00 ± 0.39, and -0.04 ± 0.64 kg/m2 in groups I, II, and III after six months, respectively. The results of ANOVA test showed that changes in BMI were significantly different between the three groups. In other words, the BMI increase in the treated ECC group was significantly higher than the other two groups. Comparison of BMI at baseline and six-month follow-up only showed a significant difference in group I (using paired t-test).
5. Discussion
In this study, 96 children in the age group of 3 - 6 years were examined in three groups (treated ECC, untreated ECC, and caries-free). BMI was evaluated in all three groups at baseline and after six months. We did not focus on the direct relationship between BMI and ECC, and our main goal was to determine the effect of ECC treatment on BMI changes, which indirectly indicated the relationship between ECC and BMI. The present results showed that BMI increased more significantly in treated children with ECC, compared to the other two groups. This finding is consistent with the results of previous studies, which examined the effect of treatment of deciduous teeth on BMI in children (16, 17). This finding indicates the importance of dental treatments in improving the physical health of children. However, many parents do not pay particular attention to the deciduous teeth of children and consider them to be temporary; accordingly, they avoid spending time or money on treatment.
On the other hand, the present study showed that the BMI of children increased with a decrease in the DMFT index. It can be concluded that ECC is significantly related to BMI. The WHO recommends all countries to consider oral health; identify risk factors that are directly involved in caries through oral healthcare planning; and control or prevent caries by adopting appropriate strategies. Generally, dental health promotion strategies are a part of general health promotion strategies and have several common risk factors. The common risk factor approach suggests that we prevent common risk factors in a number of common diseases by controlling them (18). Certain types of food and eating habits can increase the risk of weight problems and dental caries in children (15). However, our results are not consistent with the results reported by van Gemert-Schriks et al. (12) and Alkarimi et al. (13), who showed no significant difference in the anthropometric indices of children who received comprehensive dental treatments and those who did not. The discrepancy between the findings can be attributed to the normal weight of all children in the present study, besides more severe cases of dental decay in our study population, compared to the mentioned studies.
The majority of previous studies, which examined the relationship between BMI and caries in deciduous teeth, have shown an inverse relationship between BMI and DMFT index (8-10, 19); the findings of these studies are consistent with those of the present study. The inverse relationship between these two indices can be explained by the fact that the presence of decayed and infected teeth in children prevents proper nutrition. In other words, toothache impedes children from having adequate sleep and rest, which in turn affects the secretion of growth hormones (15). However, Elger et al. (20) and Davidson et al. (7) showed that obesity was significantly associated with the higher risk of caries in deciduous teeth. There are also studies, indicating no significant relationship between these two indices (11, 21). The cause of discrepancy between the findings of these studies and the present research can be the multifactorial etiology of obesity and dental caries, genetics, and environmental factors. Moreover, in a narrative review, Alshihri et al. found that obesity and dental caries were both multifactorial diseases. According to their findings, the relationship between these two conditions is so complex that it cannot be explained by a common risk factor (22). In the present study, the children’s BMI was normal at baseline, while it increased significantly with ECC treatment. However, the index value remained within the normal range. Therefore, it was not possible to evaluate and compare BMI changes in obese and low-birth-weight children in the present study. Nevertheless, considering the increase in BMI six months after the ECC treatment, it can be concluded that ECC influences the body weight.
In the present study, we attempted to include children with a similar socioeconomic status to reduce the effect of this variable. We did not find a significant relationship between BMI changes and age or sex in any of the three groups. There was also no significant relationship between the DMFT index and age or gender; the DMFT value was only higher in girls in group I, and the difference was statistically significant (P ≤ 0.05). Consistent with the present study, Quadri et al. (23) showed that the incidence of ECC was higher in girls than boys. However, in some studies, the incidence of ECC was higher in boys (15, 19). The current study showed no significant difference between males and females in terms of BMI changes, whereas some studies reported that girls had higher BMI than boys (10, 24).
There are some limitations of this study should be taken into account. They include the relatively small sample size, the role of confounding variables such as age, oral hygiene and nutritional behavior, and fluoride intake. It is recommended to conduct further studies with a larger sample size within a longer period to investigate other variables affecting BMI. However, in our study, we tried to reduce the effect of some confounding variables by including subjects from the same age group with a similar socioeconomic status. On the other hand, one of the strengths of the present study was data collection through a longitudinal method.
5.1. Conclusions
The findings of the present study showed that the BMI of children, aged 3 - 6 years, significantly increased within the normal range following dental caries treatment. Therefore, there is a need for long-term planning to change false beliefs about deciduous teeth to improve oral and general health of children in the community. It can be concluded that there is a significant relationship between ECC and BMI. Therefore, clinicians can prevent dental caries and malnutrition by identifying high-risk children and consulting with the parents about diet and behavior modifications.
