
Fulltext
Neonatal congenital diaphragmatic hernia (CDH) is a complex anomaly, the clinical course of which depends on the timing and duration of herniation and the amount of viscera herniated. Acute gastrointestinal complications of neonatal CDH are mainly caused by the incarceration of the stomach and intestines[1], which are significantly reduced by prenatal diagnosis and appropriate neonatal treatment. Neonatal gastric perforation associated with CDH is an unusual surgical emergency, the symptoms of which may be quite nonspecific[1], and the radiographic findings may show pleural effusion and massive hydroperitoneum[2,3]. Rapid diagnosis and appropriate treatment are essential. We present a 4-day-old neonate with gastric perforation and CDH, who was treated successfully.
A 2.85 kg male infant was born at term by Cesarean section. The US at 25 weeks was normal. Milk feeding was accepted 2 hours after birth. He presented with recurrent non-bilious vomiting after meals during the first 3 days. Stools were passed during this period. On day 4 of life he had tachypnea and abdominal distension and greenish vomiting and his condition deteriorated rapidly. Then he was admitted to our hospital. On physical examination there were marked abdominal distension and decreased bowel sounds. The auscultation revealed decreased air entry on the lower left side of the chest. A nasogastric tube was passed and it drained bilious aspirate. A supine thoracoabdominal radiography showed an opacified left lower lung field resembling pleural effusion and the presence of gas in the left lower chest with shifting of the mediastinum to the right and a diffuse ground-glass opacity with paucity of bowel gas (Fig. 1). An erect thoracoabdominal radiography showed changes similar to the supine radiography except for the presence of gas fluid level in the left hemithorax (Fig. 1). Subsequent US showed left hydrothorax and an abundant volume of peritoneal fluid. Oral feeding stopped and he was intubated soon after admission. Prompt laparotomy was performed, which revealed the posterolateral diaphragmatic hernia, with a hernia orifice measuring 4×3 cm and consisting a large part of the stomach. A perforation, 4 cm in diameter, was located at the back wall of greater curve of the stomach. An abundant amount of yellow fluid was identified in the peritoneal cavity. The defect of the diaphragm was closed primarily and the perforation was repaired by two-layer closure. He was extubated on the seventh postoperative day and discharged from hospital
A 2.85 kg male infant was born at term by Cesarean section. The US at 25 weeks was normal. Milk feeding was accepted 2 hours after birth. He presented with recurrent non-bilious vomiting after meals during the first 3 days. Stools were passed during this period. On day 4 of life he had tachypnea and abdominal distension and greenish vomiting and his condition deteriorated rapidly. Then he was admitted to our hospital. On physical examination there were marked abdominal distension and decreased bowel sounds. The auscultation revealed decreased air entry on the lower left side of the chest. A nasogastric tube was passed and it drained bilious aspirate. A supine thoracoabdominal radiography showed an opacified left lower lung field resembling pleural effusion and the presence of gas in the left lower chest with shifting of the mediastinum to the right and a diffuse ground-glass opacity with paucity of bowel gas (Fig. 1). An erect thoracoabdominal radiography showed changes similar to the supine radiography except for the presence of gas fluid level in the left hemithorax (Fig. 1). Subsequent US showed left hydrothorax and an abundant volume of peritoneal fluid. Oral feeding stopped and he was intubated soon after admission. Prompt laparotomy was performed, which revealed the posterolateral diaphragmatic hernia, with a hernia orifice measuring 4×3 cm and consisting a large part of the stomach. A perforation, 4 cm in diameter, was located at the back wall of greater curve of the stomach. An abundant amount of yellow fluid was identified in the peritoneal cavity. The defect of the diaphragm was closed primarily and the perforation was repaired by two-layer closure. He was extubated on the seventh postoperative day and discharged from hospital
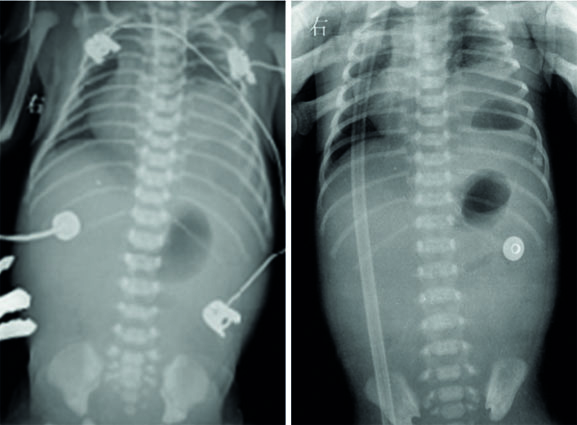
Fig. 1: Left: Supine radiography showing an opacified left lower lung field with a cyst and a diffuse ground-glass opacity with paucity of bowel gas; Right: Erect radiography showing gas fluid level in the left hemithorax.
35 days after admission. He recovered well after seven months of follow up.
There have been only a few case reports of neonatal CDH presenting with gastric perforation[1-3]. Two cases were discovered before birth[2,3]. Our case highlights the clinical course and radiography of neonatal gastric perforation associated with CDH, which are important in the diagnosis. There was one similar case observed after birth, symptoms of which were gastrointestinal rather than respiratory in origin[1]. In our case, the symptom of CDH before gastric perforation was recurrent non-bilious womiting rather than tachypnea, which is quite nonspecific, and the clinical course such as tachypnea, abdominal distension, greenish vomiting and rapid deterioration of the neonate came with gastric perforation. The radiography of neonatal CDH often shows an opacified hemithorax with mass effect and contralateral shift of the mediastinum. Bowel gas is lacking in the abdomen and can be identified in the chest[4]. In our case, the radiography showed an intrathoracic cyst rather than loops of bowel in the chest because the hernia consisted only a large part of the stomach. Pleural effusions and massive ascites indicated gastrointestinal complication associated with CDH, which is similar to some other cases[2,3]. Our case suggests that congenital diaphragmatic hernia should also be suspected in the neonate presenting with recurrent womiting. When massive ascites and pleural effusions are noted in association with CDH, gastrointestinal perforation should be considered. Early diagnosis and fluid resuscitation and prompt surgical treatment are imperative.