
Fulltext
Advances in early diagnosis and treatment have increased the survival of patients with cystic fibrosis (CF) to 30-40 years of age[1]. Interventions in nutritional status are recommended since an adequate body mass index (BMI) has been shown to be positively correlated with pulmonary function[2]. However, the development of obesity may influence the onset of CF-related diabetes[3]. We report here the case of a malnourished infant with CF who progressed to obesity at a reference center in the state of São Paulo, Brazil.
A female patient was born premature (33 weeks), weight 2,235g, length 43.5cm. At 2 months of age, CF was diagnosed, with pancreatic insufficiency (two sweat chloride >60 mEq/L and steatocrit >10%) associated with the anemia and low-protein form (Hb 7.0 g/dL; total proteins 3.0 g/dL; albumin 1.7 g/dL). Pancreatic enzyme replacement and complementation of maternal milk with an appropriate formula were started. At 3 mo 25 d, she weighed 4,745g and measured 54cm. Diarrhea, dehydration with electrolytic imbalance (Na 130 mEq/L, K 2.4 mEq/L and Cl 87mEq/L) and metabolic alkalosis (pH 7.54; bicarbonate 35,7; BE +11.5) started at 5 months of age and pseudo-Bartter syndrome was diagnosed. At 6 mo 12 d, the baby weighed 4,500g and started to receive a high-calorie, high-protein diet. At 9 mo, she weighed 6,995g and measured 64cm and at 1 year and 4 months 10,470 g and 75.5 cm. She had 5 episodes of prolonged hospitalization from 5 mo to 11 mo, when she was fed enterally (high-calorie, high-protein diet with a concentrated formula enriched with dextrin maltose and/or a nutritional supplement).
At 2 years, the patient weighed 14,300g and was 88.5cm heigh. Serum tests showed total cholesterol (TC) 200 mg/dL (VR=150), triglycerides (TG) 125 mg/dL (RV=100), low density lipoprotein (LDL) 124mg/dL (RV=100), and HDL 51 mg/dL (RV>45). A diet with normal protein, calories, lipids and increase in fibers was advised. At 2 yr 6 mo, she weighed 15,600g and measured 91.5 cm. At 3 yr, her abdominal circumference was 58 cm. At 3 yr 2 mo her weight was 17,900 g, height 98 cm and serum glucose levels were 149 mg/dL, TC 187 mg/dL, TG 100 mg/dL and LDL 126mg/dL . The weight curves are illustrated in Fig. 1.
The present case illustrates a paradoxical situation in which the clinical signs and symptoms of CF strongly encouraged the recovery of protein-energy malnutrition in order to avoid the unfavorable consequences of the disease, although the intervention led to an early triggering of obesity with possibly harmful consequences[3].
The introduction of the high-calorie, high-protein diet at 5 months and of the nutritional supplement after one year of age offered intermittently by enteral nutrition, which does not respect the mechanisms of satiety, seems to have contributed to this outcome. Despite the intense malnutrition at 5 months of age and of the various intercurrences, the nutritional recovery of the patient was rapid and progressive. Weight for age (W/A) and height for age (H/A), which were below the 3rd percentile (p3), reached the 50th percentile (p50) at 18 months of age. H/A and BMI/A were at the p90 level at 2 years and, at 3 years, BMI/A was >p90, characterizing obesity, together with the detection of dyslipidemia.
There still is no consensus about the diagnostic criteria for metabolic syndrome for children older than six years. Although we recognize the early age of the present child and the lack of references, by extrapolation she already met the criteria of NCEP/ATP-III[4], with TG>110 mg/dL, glycemia> 110 mg/dL and abdominal circumference above the cutoff point for age and sex[5].
This case underscores the difficulty in counterbalancing the positive and negative effects of weight gain during the recovery of nutritional status in patients with severe CF. Low birth weight, a high-protein and high-calorie diet and the control of the factors that trigger the malnutrition induced by CF seem to have favored the development of obesity and its complications. Despite the positive association between nutritional status and forced expiratory volume in 1 second (FEV1) reported in the literature[2], it
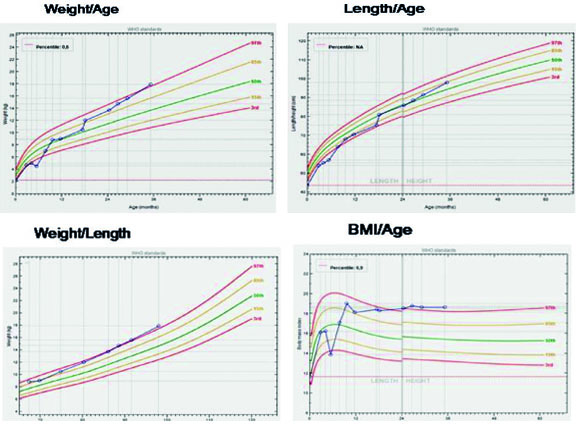
Fig. 1: Weight, length and body mass index (BMI) curves in our case with cystic fibrosis
would be prudent to maintain CF patients in an appropriate nutritional status and metabolic equilibrium in view of their currently greater longevity.