



1. Background
Physical health refers to the body’s capacity to perform daily activities, reserve energy for emergencies, avoid diseases, maintain overall physical fitness, and encompasses various indicators (1). Health indicators serve as a reflection of the overall health of a society, and those related to infants hold particular significance in assessing societal health (2). Neglecting to monitor infant growth indicators can lead to severe complications, including increased mortality (3), diminished cognitive and physical development, and emotional or physical disabilities (4). Therefore, it is crucial to track the growth and development of infants, detect deviations from the normal growth patterns early on, and prevent complications (5).
Among the components of infant growth, weight stands out as one of the most critical indicators for assessing an infant’s general health (6). Monitoring an infant’s weight significantly influences the management of child morbidity and mortality, long-term health outcomes, and adult weight (7). Abnormal weight can also have a substantial impact on a family’s psychological and socioeconomic well-being (8). Consequently, parents of such infants often experience concern and anxiety about their child’s long-term health and normal development (9, 10). Therefore, continuous weight monitoring from birth to age 5 years is essential (11).
Another pivotal aspect of infant growth and development is height (12). Abnormal height in infants might result from pathological or hereditary factors (13). Therefore, monitoring an infant’s height growth is indicative of their overall health. Therefore, tracking an infant’s height growth process is imperative for the early detection and prevention of various growth and developmental disorders (14).
Anthropometric measurements, including head circumference measurements in children, serve as indicators of their maturation during childhood. Rigorous monitoring of these measurements can help identify early growth faltering, necessitating timely and appropriate interventions (15). Measuring head circumference, particularly during the first year of life, holds immense importance because approximately 80% of an infant’s brain growth occurs during this period. Any issues during this critical phase might have irreparable consequences (16). Precise measurement of head circumference and ongoing monitoring of head growth (17) play a vital role in the diagnosis of certain conditions, such as microcephaly and macrocephaly (18). Consequently, accurate and consistent head circumference measurement in infants is a critical aspect of care, even for healthy infants, and must be meticulously documented (19).
Body temperature is another crucial aspect related to an infant’s health. Maintaining body temperature in its natural state is vital to prevent dysfunction in internal organs and protect the sensitive organs of the human body (20). Infants, who might not possess the ability to regulate their body temperature (21), might expend excessive energy in an attempt to control their body temperature, leading to various abnormalities, such as growth defects (22). Therefore, accurate monitoring of an infant’s body temperature is of paramount importance (23).
Heart rate is also among the most critical clinical indicators for evaluating an infant’s overall clinical condition (24). Its significance stems from the fact that the early postnatal period is characterized by heart rate variability (25). In pathological conditions, an increase or decrease in heart rate can serve as both a sign and a cause of issues, such as intraventricular bleeding (26), patent ductus arteriosus, and sepsis (27).
2. Objectives
Furthermore, it is not only the assessment and recording of growth components and vital signs in infants that are important. Other challenges, such as the requirement for additional human resources (28), distress experienced by both the infant and the parents, the frequent handling of the infant, and the considerable time involved, are significant concerns (29). Therefore, the present study aimed to design and evaluate a device capable of simultaneously and rapidly measuring an infant’s weight, height, head circumference, temperature, and heart rate without requiring the infant to be held. This data will then be automatically entered into a computer for analysis and monitoring.
3. Methods
This was a quantitative and semi-experimental study with the aim of designing and evaluating a device for the “simultaneous measurement of infants’ weight, height, head circumference, temperature, and heart rate”. This digital device was designed and constructed by a team consisting of Mr. Mohammad Eshaghi, a PhD student in general medicine, Mohammad Kozeghari, a PhD in software, Fatemeh Nikpour, a master’s student in epidemiology, and Arzoo Qadimi, a master’s student in pediatric nursing. The device was registered under number 104232 on 18/5/2021.
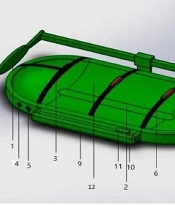
The constituent parts of this device (Figure 1) include the following components (different points of the device are numbered in the text and on the figure):

Two-dimensional model of simultaneous measurement of infants’ weight, height, head circumference, temperature, and heart rate digital device
(1) The handle has two sources of ultrasonic waves, the sender and receiver, for measuring the height of the infant. This handle is placed on the infant’s head.
(2) The digital weight sensor is embedded in the body of the device (invisible).
(3) The band is placed around the infant’s head with sources of ultrasonic waves.
(4) The digital temperature sensor site
(5) Heart rate sensor site
(6) Infant body protectors connected to the body
(7) The ultrasound waves are transmitted from section 1 to measure the height after hitting this handle; it is placed under the neonate’s feet.
(8) Rail for height adjustment
(9) Monitoring measured variables
(10) Device on and off switch
(11) Universal Serial Bus (USB) for data transfer to the computer
(12) The body of the device
In the second phase, after designing the device, to evaluate and compare it with the usual method, 100 infants were selected as a sample size from selected hospitals of Shahid Beheshti University of Medical Sciences, Tehran, Iran. G*power software (version) was used to calculate the sample size. Considering α = 0.05 (95% confidence coefficient) and a statistical power of 0.9, the minimum sample size required was 87 subjects, and 100 infants were included.
The data collection tools used included a Wong-Baker Faces scale (Figure 2) to assess infant distress and a demographic and clinical questionnaire to record growth components and measurement times. The demographic and clinical questionnaire included items such as infant age, gender, duration of intervention using routine methods and the digital device, frequency of infant movements during measurements using both methods and the number of personnel required for measurements for each infant.
After obtaining approval for the research proposal with the ethics code IR.SBMU.RICH.REC.1401.002, data collection took place within June to August 2022. Measurements of height, weight, head circumference, temperature, and heart rate of 100 infants were recorded using two routine methods and a digital device. In addition, the time of the measurement and the infant’s distress score were also recorded in both methods.
The inclusion criteria included the infantile postnatal age between 1 and 365 days, the calmness of the infant at the time of intervention, and the presence of parents. The exclusion criteria included emergency events at the time of the intervention, such as apnea or infant severe restlessness.
At first, the infant’s variables, including weight, height, head circumference, temperature, and heart rate, were measured with routine methods (Zenithmed Baby-s digital scale with a maximum capacity of 25 kg, Marathon meter (150 cm), Sk-30 digital thermometer, and Zenithmed pulse oximeter for infants). The infant’s distress score was determined and recorded with the Wong-Baker Faces scale at the time of measurement, and the number of personnel required to perform measurements for each infant was also recorded.
Subsequently, about 30 minutes after the initial measurements and once the infants had calmed down (as restlessness was one of the exclusion criteria), all measurements were repeated using the digital device, and the results were recorded. The collected data were entered into SPSS software (version 20) for analysis. The data analysis was based on the specific objectives of the study, employing descriptive statistics (mean and frequency percentage) and paired t-tests at a significance level of > 0.05.

Wong-Baker Faces Scale
4. Results
In this study, a total of 100 infants were assessed. Most of the infants fell within the age range of 1 day to 3 months (26%), and the majority (56%) were female (Table 1). The mean values and standard deviations for the time duration required to perform the measurements were 99.89 ± 4.783 and 50.74 ± 2.928 for routine methods and the digital device, respectively. The P-value (P < 0.05) indicated a significant positive difference in favor of the digital device group (Table 2).
| Variables and Category | No. (%) |
|---|---|
| Age | |
| 1 day to 3 months | 26 (26) |
| 3 months and 1 day to 6 months | 11 (11) |
| 6 months and 1 day to 9 months | 7 (7) |
| 9 months and 1 day to 12 months | 13 (13) |
| 12 months and 1 day to 15 months | 20 (20) |
| 15 months and 1 day to 18 months | 19 (19) |
| 18 months and 1 day to 21 months | 3 (3) |
| 21 months and 1 day to 24 months | 1 (1) |
| Gender | |
| Female | 56 (56) |
| Male | 44 (44) |
| Unit | |
| Emergency unit | 20 (20) |
| Intensive care unit (ICU) | 26 (26) |
| Postpartum | 18 (18) |
| Nursery | 22 (22) |
| Outpatient clinic | 14 (14) |
Demographic Results
| Variables | Group | Mean ± SD | 95% Confidence Interval of the Difference | Max | Min | P-Value | |
|---|---|---|---|---|---|---|---|
| The time spent to measure the components of the infant’s growth | Intervention | 50.74 ± 2.298 | Lower | Upper | 59 | 46 | 0.000 a |
| Control | 99.89 ± 4.783 | -50.130 | -48.167 | 113 | 73 | ||
Comparison of the Average Time Spent When Measuring Infant’s Growth Components Between Two Groups
The results of the comparison of the average distress scores of infants in both the control and intervention groups indicated that the use of the device significantly reduced infant distress during height measurements (P = 0.017), head circumference measurements (P = 0.002), temperature measurements (P = 0.000), and heart rate measurements (P = 0.004). However, there was no significant reduction in infant distress during weight measurement (P = 0.391) (Table 3).
Furthermore, the study revealed that not only did the control group require 2 or 3 personnel, although the intervention group required only 1 person, but also each infant in the control group was moved 6 times for each measurement; however, in the intervention group, they were moved only 2 times for each measurement.
| Variables | Device Measurement | Conventional Measurement | T | P-Value |
|---|---|---|---|---|
| Comparison of distress score in weight measurement time | 2.79 ± 1.080 | 2.88 ± 0.637 | -0.861 | 0.391 |
| Comparison of distress score in height measurement time | 3.29 ± 0.898 | 3.54 ± 0.878 | -2.430 | 0.017 |
| Comparison of distress score in head circumference measurement time | 3.48 ± 0.867 | 3.80 ± 0.938 | -3.156 | 0.002 |
| Comparison of distress score in temperature measurement time | 3.60 ± 0.960 | 2.18 ± 0.876 | 11.995 | 0.000 |
| Comparison of distress score in heart rate measurement time | 2.54 ± 1.22 | 2.98 ± 1.095 | -2.907 | 0.004 |
Comparison of the Distress Score in Measuring Growth Components Between Two Conventional Methods and with the Device a
5. Discussion
The present study aimed to compare the measurement of an infant’s growth components using both the routine method and the “simultaneous measurement of an infant’s weight, height, head circumference, temperature, and heart rate” device. The digital device used in this study was an innovative invention, and as such, no directly related studies were identified for discussion. However, comparing the results of this study to other studies emphasizes the significance of employing technology and novel methods in routine care to enhance precision, reduce time, and require fewer personnel.
In a study conducted by Zarezadeh et al. in 2019, a non-contact method involving capturing an overhead image of an infant’s head was introduced to calculate head circumference. This method eliminates issues associated with the previous contact-based tape measure approach (16). In the current study, a simpler programming method was used to measure an infant’s head circumference with the same level of accuracy and a more streamlined data processing and delivery process. Furthermore, the current study’s device has the capability to measure several other crucial growth components simultaneously.
In 2017, Fletcher et al. designed an infant screening platform that enables health workers to collect infant growth data automatically without manual intervention. By using a smartphone camera, the mobile app tools can automatically record an infant’s height, weight, and mid-arm circumference. Additionally, a thermal camera and a pulse oximeter were incorporated to measure the infant’s heart rate and oxygen levels. All measurements are digitally recorded and transmitted to a central server (30). A comparison between the capabilities of the device in Fletcher et al.’s study and the present study reveals that although Fletcher et al.’s device can measure multiple variables, it still relies on a separate pulse oximeter device to measure heart rate and cannot independently measure all the variables (30).
In 2015, Sokolover et al. developed a stereo system capable of capturing images of specific key points on an infant’s body, such as the top of the head, under the chin, the upper pelvis, the knee cap, and the sole. These key points are then used to calculate the child’s height. The stereoscopic system has proven to be accurate, reliable, and user-friendly, minimizes physical contact and discomfort for infants, and has the potential to measure the height of premature infants within an incubator (31). A comparison between the device used in the present study and the one in Sokolover et al.’s study indicates that the digital device in the present study performs measurements more rapidly and with greater ease, and it measures additional growth variables. However, it cannot be utilized within an incubator (31).
In 1988, Cope and Delpy introduced an article on the infrared spectroscopic technique, which offers the capability for continuous and safe monitoring of changes in blood and tissue oxygenation in children’s organs (32). Taking into consideration the potential side effects of infrared waves on infant skin in previous studies, it appears that the permanent use of infrared waves in the device designed in the aforementioned study might lead to side effects not mentioned in the article.
In 2021, Khanam et al. conducted a single-center study in South Australia titled “Non-contact Automatic Vital Signs Monitoring of Infants in a Neonatal Intensive Care Unit Based on Neural Networks”. The study aimed to remotely measure the heart rate and respiratory rate of six infants admitted to the neonatal intensive care unit (NICU) using a digital camera. The heart rate was measured using the photoplethysmography signal extracted from the camera; nevertheless, the respiratory rate was measured utilizing the photonic radar integrated into the camera. The study showed a small difference of 2.23 heart rate per minute and 2.69 respiratory rate per minute between the measured data and the reference data. A convolutional neural network was used to automatically select the region of interest, and signal decomposition was employed to minimize noise effects. Strong correlations were observed between the data obtained from the camera measurements and the data from the cardiopulmonary monitoring connected to the infants. Therefore, this technique might find application in clinical settings as an economical, non-contact, and easily implementable monitoring system (33). It is worth noting that the mentioned device in this study measures only two components. In addition, it might produce significantly different values in the presence of infant movement or camera motion and changes in environmental lighting conditions. Nevertheless, the current device has the capacity to simultaneously and accurately measure five components, even in the face of environmental changes and infant movements.
In 2018, Bauman et al. conducted an experimental study titled “Assessing Community Health: An Innovative Tool for Measuring Height and Length”. The aforementioned study’s aim was to measure the lying and standing height of children aged 1 month to 8 years in western Kenya. The device used in this study comprises a battery-operated distance meter with a range of 0.05 - 60 meters and an accuracy of 60.06 cm. It also includes a hinge between two pieces of metal, creating a 90-degree angle for laser reflection. This measurement method requires two trained individuals. Each child’s height was measured once using the routine method (with a meter) and three times with the device. The data were then analyzed and reported using t-tests, Pearson correlation, and Kappa statistics (34). In comparison to the current device, the “innovative height measuring device” is limited to measuring only the height component and necessitates the involvement of two trained individuals, rendering it less versatile than the current device.
In 2021, Wu et al. conducted a study in China involving 76 infants aged 3 months to 2.5 years. The study aimed to evaluate the correlation between head circumference measurements using the routine method and a structured light three-dimensional scanning device. Initially, the infants’ head circumferences were measured using a meter and caliper. Subsequently, the head circumferences of these infants were measured using the mentioned device and compared. The confidence interval value, with a confidence level of 95%, fell between 0.633 and 0.988. The correlation coefficient was 0.98, with a P-value of < 0.001, indicating a high correlation and statistical significance between the two measurement methods. The Bland-Altman plot also demonstrated reasonable agreement between the two methods. Therefore, the mentioned device allows for faster and highly precise measurements around the heads of infants and can be used for infants with unusual skull shapes (35). However, it is important to note that this device measures only one component in comparison to the simultaneous measurement device for multiple growth components.
5.1. Conclusions
The noteworthy point is that in the aforementioned studies, researchers have only described the characteristics of the developed devices, and none of them has investigated the effectiveness of the designed devices during use. However, it appears that the device designed in the present study might possess the positive features of the devices reviewed in those studies while simultaneously examining multiple variables in a short period.
Today, in most parts of the world, these components are measured separately and manually, a process that consumes a significant amount of time for healthcare providers and often leaves infants restless during measurements. In addition to the time-consuming nature of conventional measurements, there is a risk of human error in child care, leading to mistakes in data values and an increased need for human resources. The “simultaneous measurement of weight, height, head circumference, temperature, and heart rate of an infant” device, which was invented for the first time in the world, can accurately measure all these components simultaneously with a minimum number of personnel. Consequently, it can be asserted that this device could serve as a suitable alternative to the conventional method of measuring an infant’s growth components.
5.2. Limitations
One of the limitations of the present study was the scarcity of related studies available for discussion and comparison of study results. Furthermore, since the comparison was carried out with the routine method, which relies on individual performance and is susceptible to human error, the comparison and generalization of the results are also constrained. Additionally, other limitations of the study included the small sample size, the utilization of low-quality equipment in routine measurements, single-center intervention, and the absence of blinded measurements. Therefore, to draw more accurate conclusions regarding the accuracy of the device’s measurements, it is advisable to prepare and develop more digital devices and conduct repeated measurements in a larger population. Although the current study has its limitations due to time and financial constraints, it is recommended that further studies in this field be carried out.
