





1. Background
Dental anxiety is a distressing psychological response triggered by fear, stress, or apprehension associated with the dental setting or procedures (1). It is estimated that many individuals experience anxiety before dental appointments and may refuse dental care (2). Contributing factors to dental anxiety and fear include the dental environment, dental instruments like injection syringes and dental handpieces (3). Additionally, unpleasant dental experiences, prior head and neck trauma, and non-dental factors such as physical and mental abuse, generalized anxiety, depression, or post-traumatic stress disorder can contribute to the development of dental anxiety (4). Clinical manifestations of dental anxiety and fear in some patients may include symptoms like sweating, tachycardia, hypotension, sadness, and even panic attacks (5).
Furthermore, individuals experiencing dental anxiety may choose to avoid seeking dental care, leading to an increase in dental issues such as abscesses, oral infections, dental pain, and eventual tooth loss (6). Those with dental anxiety subject themselves to deteriorating dental conditions that necessitate more complex, time-consuming, and expensive treatments with a poorer prognosis. This avoidance can contribute to patients' painful and unpleasant dental experiences, further intensifying their anxiety and creating a cycle of dental anxiety (7).
Despite several studies challenging the significance of parental anxiety in influencing a child's response to dental treatment, conflicting results have emerged regarding the impact of both parental and children's anxiety on the development of dental caries (8, 9).
2. Objectives
Considering the pivotal role parents play in preserving oral and dental health, as well as in making decisions about their children's dental care, and noting that existing research predominantly focuses on the influence of mothers on a child's dental condition, we aimed to investigate the association between parental and children's dental anxiety with childhood dental caries. We hypothesized that parental and children's dental anxiety affects the childhood dental caries index.
3. Methods
3.1. Participants and Settings
This analytic cross-sectional study was conducted on 7 - 12-year-old students and their parents in schools in Rasht, Iran, from December 2022 to April 2023. Participants were chosen through a multistage sampling process. Initially, each district of the Guilan education system was selected using stratified sampling. From two selected districts, schools were chosen based on their proportion in each district using cluster sampling. In the final stage, one grade was randomly selected using random sampling.
3.2. Inclusion Criteria
Inclusion criteria: (1) capability of the children and their parents to answer the questions of the questionnaire, with no cognitive impairments; (2) child aged between 7 and 12 years and their ability to understand the language; (3) literate parents living with the child most of the time; (4) willingness to answer the questions despite psychological disorders in children and parents; (5) absence of chronic or acute medical disorders, neurological disorders, and history of psychological disorders, etc., in parents and children.
3.3. Exclusion Criteria
Exclusion criteria: (1) refusal to cooperate at any stage by the parents; (2) refusal by children to cooperate with oral examination; (3) children who live with only one parent for any reason.
3.4. Sample Size
To determine the sample size, considering the relationship between parents' dental anxiety and children's dental anxiety with dental caries in 7 - 12-year-old children, the correlation was included in the sample size estimation. Considering the statistical power of 80%, an error level of 0.05, and a correlation obtained from a previous study equal to 0.17 (correlation between parents' anxiety and children's tooth decay), the minimum sample size was determined to be 275 (10).
3.5. Data Gathering
Each parent completed a checklist comprising two parts. The first part gathered demographic characteristics, while the second part utilized the Modified Dental Anxiety Scale (MDAS) to assess parental dental anxiety. Clinical examinations of the children's oral cavities were conducted at the school using disposable mirrors, explorers, examination gloves, and masks. Subsequently, the examiner verbally asked the questions from the Modified Child Dental Anxiety (MCDAS) Questionnaire.
Parental dental anxiety was assessed through an interview using the Persian MDAS Questionnaire, which comprises five questions, each with five choices. The questionnaire measured anxiety levels in specific situations, including waiting for the dental session before attendance, waiting in the clinic, waiting in the dental unit for the injection of local anesthesia, waiting in the dental unit for tooth preparation, and waiting in the dental unit for scaling and root planning. Participants could choose from five options ranging from no anxiety (1 score) to severe anxiety (5 scores), resulting in a score range of 5 to 25 (11). Both parents of each child participated in this study.
Children's dental anxiety was evaluated using the Persian version of the MCDAS Questionnaire, comprising eight questions, each with five choices similar to the MDAS. The choices ranged from no worries (1 score) to very worried (5 scores). Consequently, the score range for this questionnaire was 8 to 40, and a child scoring 19 or higher was considered to have dental anxiety (12). Participants were divided into anxious and non-anxious groups (score range between 8 - 19) based on the obtained scores and were compared.
The assessment of children's dental caries using the DMFT/dmft (decayed, missing, and filled teeth) Index was performed by a trained dentist. DMFT indicated the status of permanent teeth, and dmft served as the indicator for primary teeth. The oral examination for dental decay commenced from the most posterior tooth in the right quadrant of the maxilla to the most posterior tooth in the left quadrant, following the same sequence in the mandible. In the dmft Index, primary teeth that were missing due to factors such as the child's age or reasons unrelated to dental decay, like trauma, were not considered missing teeth.
3.6. Ethical Considerations
After obtaining permission from the parents through a written informed consent letter, data were collected. Ethical approval was obtained from the ethics committee of Guilan University of Medical Sciences (ethical code: IR.GUMS.REC.1401.501).
3.7. Statistical Analysis
For describing the qualitative data, frequency and percentage were used, and for describing the quantitative data, mean and standard deviation were used. Normality was assessed through the Kolmogorov-Smirnov test, and the data were found to be normally distributed. The comparison of parental anxiety status with that of the children was performed using a chi-square test. To check the simultaneous effect of independent variables on the response variable, linear regression was used. Statistical analyses were done using IBM statistical package for the social sciences (SPSS) statistics for Windows, version 28 (IBM Corp., Armonk, N.Y., USA). The data were considered statistically significant if P < 0.05 in all tests.
4. Results
This study examined a total of 275 parents (comprising 275 fathers and 275 mothers) and 275 children. Fathers and mothers fell within the age ranges of 30 - 60 and 29 - 46, respectively, with mean ages of 41.08 ± 4.80 for fathers and 37.64 ± 4.25 for mothers. The assessed children, aged 7 to 12, had a mean age of 9.32 ± 1.85, with 137 (49.8%) boys and 138 (50.2%) girls.
Following the evaluation of parental dental anxiety, it was revealed that 47.3% (N = 130) of mothers and 20.4% (N = 56) of fathers expressed anxiety about dental care. Additionally, 12.4% (N = 34) of the children exhibited dental anxiety. The DMFT and dmft indices for children were 0.81 ± 1.22 and 2.77 ± 2.60, respectively, with an overall score (DMFT + dmft) of 3.58 ± 2.69.
According to the findings, there was no significant difference between the dental anxiety levels of mothers (P = 0.071) and fathers (P = 0.624) and the dental anxiety levels of children. The majority of children, whether their parents were anxious or non-anxious, were not anxious about clinical dental care (Table 1).
| Variables | Dental Anxiety | Dental Anxiety of Children | P-Value b | |
|---|---|---|---|---|
| Not Anxious | Anxious | |||
| Mother | Non-anxious | 132 (91) | 13 (9) | 0.071 |
| Anxious | 109 (83.8) | 21 (16.2) | ||
| Father | Non-anxious | 193 (88.1) | 26 (11.9) | 0.624 |
| Anxious | 48 (85.7) | 8 (14.3) | ||
Comparison of Dental Anxiety of Children Based on Parental Dental Anxiety a
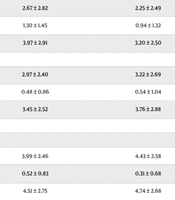
| Variables | Parental Dental Anxiety | P-Value | |
|---|---|---|---|
| Non-anxious | Anxious | ||
| Mother | |||
| Child sex | |||
| Boy | |||
| dmft b | 2.67 ± 2.82 | 2.25 ± 2.49 | 0.182 |
| DMFT b | 1.30 ± 1.45 | 0.94 ± 1.32 | 0.065 |
| dmft + DMFT b | 3.97 ± 2.91 | 3.20 ± 2.50 | 0.049 |
| Girl | |||
| dmft b | 2.97 ± 2.40 | 3.22 ± 2.69 | 0.287 |
| DMFT b | 0.48 ± 0.86 | 0.54 ± 1.04 | 0.353 |
| dmft + DMFT b | 3.45 ± 2.52 | 3.76 ± 2.88 | 0.253 |
| Age of child | |||
| Younger than 9 | |||
| dmft b | 3.99 ± 2.46 | 4.43 ± 2.58 | 0.164 |
| DMFT b | 0.52 ± 0.83 | 0.31 ± 0.68 | 0.058 |
| dmft + DMFT b | 4.51 ± 2.75 | 4.74 ± 2.68 | 0.318 |
| 9 and older | |||
| dmft b | 1.49 ± 2.06 | 1.57 ± 1.95 | 0.409 |
| DMFT b | 1.24 ± 1.49 | 1.05 ± 1.38 | 0.215 |
| dmft + DMFT b | 2.73 ± 2.34 | 2.62 ± 2.36 | 0.388 |
| History of referral to dental clinic | |||
| None | |||
| dmft b | 3.16 ± 2.24 | 2.36 ± 2.63 | 0.094 |
| DMFT b | 0.5 ± 0.88 | 0.55 ± 0.1 | 0.405 |
| dmft + DMFT b | 3.65 ± 2.63 | 2.92 ± 2.72 | 0.130 |
| During toothache | |||
| dmft b | 3.08 ± 2.58 | 2.81 ± 2.45 | 0.267 |
| DMFT b | 0.80 ± 1.28 | 0.74 ± 1.11 | 0.383 |
| dmft + DMFT b | 3.88 ± 2.67 | 3.55 ± 2.52 | 0.230 |
| Sometimes | |||
| dmft b | 2.55 ± 2.73 | 3.10 ±3.18 | 0.520 |
| DMFT b | 0.87 ± 1.12 | 0.75 ± 1.29 | 0.382 |
| dmft + DMFT b | 3.42 ± 2.87 | 3.85 ± 3.23 | 0.634 |
| Every year | |||
| dmft b | 2 ± 3.70 | 2.86 ± 2.61 | 0.213 |
| DMFT b | 1.86 ± 1.34 | 1.71 ± 2.36 | 0.417 |
| dmft + DMFT b | 3.86 ± 3.72 | 4.57 ± 2.57 | 0.342 |
| Age | |||
| Younger than 38 | |||
| dmft b | 3.24 ± 2.61 | 3.50 ± 2.82 | 0.304 |
| DMFT b | 0.95 ± 1.26 | 0.52 ± 0.98 | 0.027 |
| dmft + DMFT b | 4.19 ± 2.82 | 4.02 ± 2.95 | 0.380 |
| 38 and older | |||
| dmft b | 2.40 ± 2.53 | 2.25 ± 2.40 | 0.353 |
| DMFT b | 0.76 ± 1.20 | 0.89 ± 1.31 | 0.253 |
| dmft + DMFT b | 3.16 ± 2.50 | 3.14 ± 2.49 | 0.486 |
| Father | |||
| Child sex | |||
| Boy | |||
| dmft b | 2.40 ± 2.74 | 2.65 ± 2.32 | 0.448 |
| DMFT b | 1.26 ± 1.47 | 0.59 ± 0.87 | 0.029 |
| dmft + DMFT b | 3.66 ± 2.76 | 3.24 ± 2.63 | 0.512 |
| Girl | |||
| dmft b | 2.96 ± 2.44 | 3.55 ± 2.83 | 0.364 |
| DMFT b | 0.49 ± 0.91 | 0.59 ± 1.05 | 0.703 |
| dmft + DMFT b | 3.45 ± 2.60 | 4.15 ± 2.94 | 0.252 |
| Age of child | |||
| Younger than 9 | |||
| dmft b | 4.04 ± 2.57 | 4.77 ± 2.14 | 0.106 |
| DMFT b | 0.41± 0.73 | 0.59 ± 1.01 | 0.617 |
| dmft + DMFT b | 4.45 ± 2.76 | 5.36 ± 2.34 | 0.075 |
| 9 and older | |||
| dmft b | 1.39 ± 1.89 | 2 ± 2.28 | 0.060 |
| DMFT b | 1.30 ± 1.52 | 0.58 ± 0.92 | < 0.001 |
| dmft + DMFT b | 2.70 ± 2.29 | 2.59 ± 2.54 | 0.407 |
| History of referral to dental clinic | |||
| None | |||
| dmft b | 2.60 ± 2.25 | 3.20 ± 3.19 | 0.658 |
| DMFT b | 0.60 ± 1.02 | 0.27 ± 0.46 | 0.400 |
| dmft + DMFT b | 3.21 ± 2.45 | 3.47 ± 3.48 | 0.911 |
| During toothache | |||
| dmft b | 2.82 ± 2.54 | 3.37 ± 2.41 | 0.141 |
| DMFT b | 0.80 ± 1.22 | 0.69 ± 1.12 | 0.328 |
| dmft + DMFT b | 3.62 ± 2.59 | 4.06 ± 2.60 | 0.201 |
| Sometimes | |||
| dmft b | 2.91 ± 3 | 1.86 ± 2.03 | 0.189 |
| DMFT b | 0.82 ± 1.22 | 0.86 ± 0.90 | 0.468 |
| dmft + DMFT b | 3.73 ± 3.09 | 2.71 ± 2.29 | 0.206 |
| Age | |||
| Younger than 41 | |||
| dmft b | 3.23 ± 2.59 | 3.71 ± 2.47 | 0.216 |
| DMFT b | 0.83 ± 1.34 | 0.48 ± 1.12 | 0.188 |
| dmft + DMFT b | 4.06 ± 2.68 | 4.19 ± 2.56 | 0.418 |
| 41 and older | |||
| dmft b | 2.07 ± 2.49 | 2.71 ± 2.63 | 0.096 |
| DMFT b | 0.91 ± 1.20 | 0.66 ± 0.84 | 0.124 |
| dmft + DMFT b | 2.98 ± 2.57 | 3.37 ± 2.92 | 0.227 |
The DMFT/dmft/ DMFT + dmft Scores Based on the Different Variables a
The results revealed a significant difference between paternal dental anxiety and the DMFT Index (the number of teeth with caries experience) (P = 0.029), with boys having anxious fathers exhibiting a lower mean DMFT score (Table 2). Conversely, boys with anxious mothers showed a statistically significant lower DMFT + dmft score compared to those with non-anxious mothers (P = 0.049).
In children aged nine and older, those with anxious fathers exhibited significantly lower DMFT scores compared to their counterparts with non-anxious fathers (P < 0.001). However, there was no significant difference in DMFT scores for children younger than nine, where the scores were higher in those with anxious fathers (P = 0.617). No statistically significant difference was observed in DMFT/dmft concerning maternal dental anxiety based on the age of the children. Findings also indicated no significant difference between parental dental anxiety and the number of teeth with caries experienced by children based on their history of referral to a dental clinic.
The association between paternal dental anxiety and the DMFT/dmft Index of children did not show statistical significance based on the age of the fathers. However, a significant difference was noted in the relationship between maternal dental anxiety in those younger than 38 and the DMFT Index (P = 0.027), with anxious mothers having lower DMFT scores. Boys with anxious fathers demonstrated significantly lower DMFT scores compared to boys with non-anxious fathers (P = 0.029). Conversely, girls with anxious fathers exhibited higher DMFT scores than girls with non-anxious fathers (P = 0.703) (Table 2).
Linear regression analysis assessed various potential factors, revealing significant effects on children's dental anxiety: The DMFT Index (P = 0.023), the child's gender (P = 0.007), the history of referral to a dental clinic (P = 0.045), and maternal dental anxiety (P = 0.043). Boys exhibited higher dental anxiety than girls, and dental anxiety in children increased with higher DMFT levels and maternal dental anxiety. Moreover, it was indicated that children's dental anxiety decreased when they had a history of referral to a dental clinic.
None of the independent variables significantly influenced paternal dental anxiety. However, the child's age (P < 0.001), the child's dental anxiety (P = 0.040), and the history of referral to a dental clinic (P = 0.024) demonstrated a significant effect on maternal dental anxiety. Maternal dental anxiety exhibited a significant relation with the child's age and dental anxiety and an inverse relationship with the history of referral to a dental clinic (Table 3).
| Variables | B | S.E. | Beta | Sig. |
|---|---|---|---|---|
| Childhood dental anxiety | ||||
| Child age | -0.16 | 0.20 | -0.07 | 0.434 |
| dmft | 0.06 | 0.11 | 0.03 | 0.600 |
| DMFT | 0.50 | 0.22 | 0.14 | 0.023 |
| Child Sex | -1.64 | 0.60 | -0.19 | 0.007 |
| History of referral to dental clinic | -0.54 | 0.27 | -0.12 | 0.045 |
| Maternal dental anxiety | 0.11 | 0.05 | 0.12 | 0.043 |
| Paternal dental anxiety | 0.08 | 0.07 | 0.07 | 0.221 |
| Maternal age | -0.01 | 0.07 | -0.01 | 0.881 |
| Paternal age | 0.04 | 0.07 | 0.05 | 0.521 |
| Maternal education | -0.03 | 0.25 | -0.01 | 0.903 |
| Paternal education | -0.25 | 0.33 | -0.06 | 0.447 |
| Family income | -1.14 | 0.61 | -0.13 | 0.064 |
| Fathers dental anxiety | ||||
| Child age | 0.08 | 0.17 | 0.04 | 0.612 |
| Child MCDAS | 0.08 | 0.05 | 0.10 | 0.104 |
| dmft | 0.09 | 0.09 | 0.07 | 0.332 |
| DMFT | -0.21 | 0.19 | -0.07 | 0.270 |
| Child sex | -0.28 | 0.50 | -0.04 | 0.581 |
| History of referral to dental clinic | -0.13 | 0.23 | -0.03 | 0.550 |
| Paternal age | 0.09 | 0.05 | 0.12 | 0.061 |
| Paternal education | -0.21 | 0.24 | 0.06 | 0.370 |
| Family income | 0.77 | 0.49 | -0.11 | 0.119 |
| Mothers dental anxiety | ||||
| Child age | 0.84 | 0.21 | 0.32 | < 0.001 |
| Child MCDAS | 0.14 | 0.06 | 0.12 | 0.040 |
| dmft | 0.11 | 0.12 | 0.06 | 0.373 |
| DMFT | -0.23 | 0.25 | -0.05 | 0.356 |
| Child sex | 0.26 | 0.68 | 0.02 | 0.697 |
| History of referral to dental clinic | -0.68 | 0.30 | -0.14 | 0.024 |
| Maternal age | 0.04 | 0.07 | 0.04 | 0.507 |
| Maternal education | 0.23 | 0.25 | 0.06 | 0.343 |
| Family income | -0.67 | 0.46 | -0.09 | 0.149 |
The Linear Regression Analysis Assessing the Effect of Independent Variables on Childhood and Parental Dental Anxiety
5. Discussion
Fear and anxiety are considered natural aspects of human development. However, if their intensity surpasses the expected level and hinders normal daily life, intervention may become necessary (13). In the context of children, dental anxiety can result in avoidance of dental visits and non-cooperation during treatment. Identifying a child's anxiety allows the dentist to employ various behavior modification techniques, explaining treatment stages and familiarizing the patient with dental instruments to reduce or eliminate anxiety (14). Our findings indicated a significant relationship between maternal dental anxiety and DMFT + dmft scores in boys. Additionally, the study revealed that the number of teeth with caries, the child's sex, history of dental clinic visits, and maternal dental anxiety significantly influenced the child's dental anxiety.
In this study, the mean score of anxiety in children was 11.89 ± 4.21, and the frequency of anxious children was 12.4%. Alsadat et al. reported the frequency of anxious cases as 23.5% (15). The variations in dental anxiety figures stem from diverse social and cultural factors that differ across countries. Another contributing factor is the inadequacy of educational plans and programs for dental students in dealing with children's dental anxiety in practical settings, particularly in developing countries compared to developed ones.
According to the results of this study, the sex of children exerted a significant influence on dental anxiety, with boys exhibiting higher anxiety levels than girls. In contrast, Kol and Çelenk found higher anxiety scores for girls, while Folayan et al. did not observe a significant difference in anxiety between girls and boys (16, 17). Javadinejad et al. also reported no significant difference between dental anxiety and the sex of children aged 6 - 8 years (12). These variations in results may occur due to distinct behavioral patterns, social and cultural beliefs, and potential differences in the perception and expression of fear and anxiety between the two genders.
In the current study, the mean score for dental anxiety of mothers and fathers was 11.41 ± 4.77 and 8.44 ± 3.51, respectively. The frequency of anxious cases among mothers and fathers was 47.73% and 20.4%, respectively. Consistently, Alhareky et al. demonstrated that 92% of mothers were anxious (18). These similar results can be attributed to the effect of parental sex on this issue. We also found a significant difference between the dental anxiety of mothers and children, with dental anxiety being higher in children with anxious mothers. In line with the present study, previous investigations have found a significant relationship between the dental anxiety of children and mothers (16, 19). Considering that mothers tend to experience higher anxiety than fathers, the significance of this result becomes evident. It indicates that mothers exert a considerable influence on the dental anxiety of their children and can potentially transmit this anxiety, creating a more challenging dental situation. This intergenerational transmission of dental anxiety may lead to resistance to seeking dental care, adversely impacting the dental health of children.
Significantly, it was indicated that the DMFT + dmft Index of children with anxious mothers was lower than that of children with non-anxious mothers. Furthermore, among mothers younger than 38, the DMFT score for children with anxious mothers was significantly lower than the DMFT score for children with non-anxious mothers. This result is consistent with other studies that found a significant difference between maternal dental anxiety and the dmft Index (18, 20). However, some studies observed inconsistent results and did not find any significant difference between maternal dental anxiety and the dmft Index (21, 22). The diversity in results could be due to various factors such as education or parents’ behavior affecting lower caries incidence.
It was demonstrated that as paternal dental anxiety increases, the DMFT scores in boys decrease. Moreover, the DMFT among children older than nine was significantly lower for those with anxious fathers. In contrast, Kol and Çelenk found no significant difference between paternal dental anxiety and the DMFT + dmft scores of the children (16). In this study, it was observed that anxious parents are more likely to have children with lower DMFT scores. This observation could be interpreted as indicating that parents, having undergone unpleasant dental treatments themselves, may wish to protect their children from similar experiences. Therefore, they exhibit greater attention and concern for their children’s dental health.
It was indicated that there is a significant difference between dental anxiety and a history of referral to a dental clinic; the more children visit a dental clinic, the less anxiety they have toward it. In line with this outcome, Alshoraim et al. and Rath et al. reported that dental anxiety was lower among children with a history of referral to a dental clinic, and frequent dental visits also decreased anxiety (14, 23). This underscores the significance of initiating primary dental visits for children at the age of one. Early visits facilitate the prompt diagnosis of dental caries and other oral disorders, contributing to lower dental anxiety in later stages of development.
A significant difference was seen in the relationship between the dental anxiety of children and the DMFT Index; children with higher DMFT scores showed higher dental anxiety scores. Kol and Çelenk also found a significant difference between the dental anxiety of children and the DMFT + dmft Index (16). This suggests that dental anxiety could serve as a warning sign, prompting the need for dental care and resulting in an elevated DMFT Index for permanent teeth, potentially leading to permanent tooth loss.
Based on the results, the age of the children, the dental anxiety of the children, and a history of referral to a dental clinic were found to have significant effects on the dental anxiety of mothers. Specifically, the age and dental anxiety of the children exhibited a positive effect on the dental anxiety of the mothers, whereas a history of referral to a dental clinic showed an inverse relationship. Similarly, Khawja et al. found that the age of the children significantly affects the dental anxiety of the mothers, but in a negative direction (19).
5.1. Strengths and Limitations
Our study underscores the importance of early dental visits and emphasizes the dentist's responsibility to alleviate stress and fear in patients. To address this, comprehensive plans and programs for both dentists and mothers should be given increased consideration to alleviate dental anxiety in society. Despite these findings, the study had some limitations, including non-cooperation from some schools, parents, and children, leading to incomplete questionnaires and restricted dentist visits. Future research with larger sample sizes and broader environments is recommended for more accurate results. Additionally, using different caries indices and dental anxiety questionnaires would enhance the comprehensiveness of such studies.
5.2. Conclusions
The results highlight the considerable influence of mothers on their children's dental anxiety. While it might be assumed that anxious mothers pass on their anxiety to their children, discouraging them from visiting the dentist, the data contradicts this notion. Children with anxious mothers exhibited lower DMFT scores than those with non-anxious mothers. This suggests that anxious mothers, perhaps driven by their dental anxiety, are more cautious about their children's dental health, thereby resulting in lower DMFT + dmft scores. This attention to dental caries also extends to fathers, as anxious fathers were likely to have boys with lower DMFT scores. However, given that the dental anxiety scores for mothers were higher than those for fathers, it can be inferred that mothers play a more significant role and are more concerned about their children's dental health. Additionally, a history of dental clinic visits had a positive impact, reducing the dental anxiety of both mothers and children. This underscores the importance of early dental visits and emphasizes the dentist's responsibility to alleviate stress and fear in patients.
