
Fulltext
Pulmonary hypoplasia and pulmonary artery hypoplasia are two congenital malformations of the respiratory system which are rarely observed in the clinic[1,2]. The difference in patterns and the extent of this congenital malformation result in a great variability in clinical manifestations, usually leading to misdiagnoses. We herein for the first time report a case of a boy who presented with dyspnea, cough, cyanosis and fever, and was initially diagnosed as pulmonary atelectasis. Later on, through a series of computed tomography angiography (CTA), color Doppler ultrasono-graphy and fiberoptic bronchoscopy procedures, he was found to have malformations of the lung and digestive system, atrial septal defect and
spina bifida.
A 16 month-old Han (Mongolian race) boy from the Sichuan Province was admitted to our hospital due to difficulty in breathing, cough, expectoration, cyanosis, and medium-high fever that were persistent for more than one month. He was marasmic with poor eating, passed loose yellow-green stools without blood three to four times per day. His mother suffered from colporrhagia and was administered with Chinese medicine during her first month of pregnancy. No history of radioactive, toxic material and pet exposure before and during pregnancy were found. This child had an anoplasty for congenital anal atresia, and had blue light treatment for jaundice during neonatal period. He also had recurrent upper respiratory tract infection previously.
There was no similar case in his family and his parents were not intermarriaged. Physical examination revealed normal vital signs. The boy was underweight without icterus in both his skin and sclera, short of breath, showed flaring of alae nasi, lip cyanosis, trachea deviation to the left, and marked with an inspiratory of three depressions. While his right thoracic cage was full and stable, his left side was collapsed, leaving uneven respiratory movement, no sense of pleural friction. In addition, exaggerated breath sounds were heard throughout the right lung, while breath sounds were diminished in the left lung; without dry or moist rales. Heart percussion was normal. The abdomen was slightly distended and venae epigastriae were visible. While the liver under the right rib cage was untouched, the 4 cm spleen was felt under the left rib edge. His liver function, blood, stool, urinalysis and other biochemical parameters were within normal ranges. Cytomegalovirus (CMV)-IgM was negative, CMV-IgG ++. Sputum was positive for Hemophilus parainfluenzae and Pseudomonas aeruginosa. Virus tests in nasopharyngeal secretion sample were all negative. Chest X-ray and CT scan suggested pneumonia, left-side pleurisy and agenesis of the left lung. Fiberoptic bronchoscopy showed luminal stenosis in the middle and lower part of the left main bronchial tube, and dead ends in the left superior and lower lobe bronchus.
To further investigate, we performed 64-slice chest and abdominal CT angiography. The results, summarized in Fig. 1, showed: 1) Absence of the left pulmonary artery, agenesis of the left lung and obstruction of the distal area of the left main bronchial tube. 2) Heart and mediastinum were displaced to the left, and a left hernia of the mediastinum. 3) Light interstitial inflammation in the right lung with pleura thickened on both sides. 4) A mass of irregular, tortuous blood vessels in the first hepatic hilar region, and varices of fundus of stomach with splenomegaly, which was consistent with the cavernous transformation of the portal vein (CTPV). 5) Spina bifida at the L3 level.
spina bifida.
A 16 month-old Han (Mongolian race) boy from the Sichuan Province was admitted to our hospital due to difficulty in breathing, cough, expectoration, cyanosis, and medium-high fever that were persistent for more than one month. He was marasmic with poor eating, passed loose yellow-green stools without blood three to four times per day. His mother suffered from colporrhagia and was administered with Chinese medicine during her first month of pregnancy. No history of radioactive, toxic material and pet exposure before and during pregnancy were found. This child had an anoplasty for congenital anal atresia, and had blue light treatment for jaundice during neonatal period. He also had recurrent upper respiratory tract infection previously.
There was no similar case in his family and his parents were not intermarriaged. Physical examination revealed normal vital signs. The boy was underweight without icterus in both his skin and sclera, short of breath, showed flaring of alae nasi, lip cyanosis, trachea deviation to the left, and marked with an inspiratory of three depressions. While his right thoracic cage was full and stable, his left side was collapsed, leaving uneven respiratory movement, no sense of pleural friction. In addition, exaggerated breath sounds were heard throughout the right lung, while breath sounds were diminished in the left lung; without dry or moist rales. Heart percussion was normal. The abdomen was slightly distended and venae epigastriae were visible. While the liver under the right rib cage was untouched, the 4 cm spleen was felt under the left rib edge. His liver function, blood, stool, urinalysis and other biochemical parameters were within normal ranges. Cytomegalovirus (CMV)-IgM was negative, CMV-IgG ++. Sputum was positive for Hemophilus parainfluenzae and Pseudomonas aeruginosa. Virus tests in nasopharyngeal secretion sample were all negative. Chest X-ray and CT scan suggested pneumonia, left-side pleurisy and agenesis of the left lung. Fiberoptic bronchoscopy showed luminal stenosis in the middle and lower part of the left main bronchial tube, and dead ends in the left superior and lower lobe bronchus.
To further investigate, we performed 64-slice chest and abdominal CT angiography. The results, summarized in Fig. 1, showed: 1) Absence of the left pulmonary artery, agenesis of the left lung and obstruction of the distal area of the left main bronchial tube. 2) Heart and mediastinum were displaced to the left, and a left hernia of the mediastinum. 3) Light interstitial inflammation in the right lung with pleura thickened on both sides. 4) A mass of irregular, tortuous blood vessels in the first hepatic hilar region, and varices of fundus of stomach with splenomegaly, which was consistent with the cavernous transformation of the portal vein (CTPV). 5) Spina bifida at the L3 level.
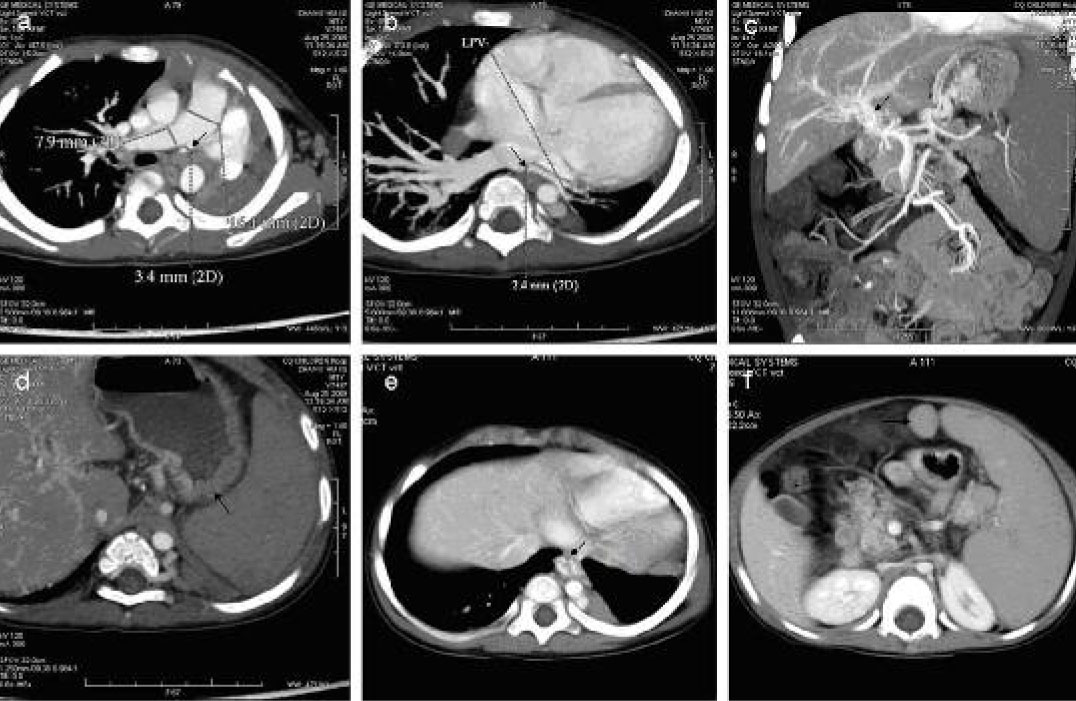
Fig 1. a-b. The left pulmonary artery and vein were thinned; diameters were 3.4 and 2.4 mm, respectively. c. The irregular vessels in the primary hepatic portal area. The venous plexus of the portal vein area was thick and varicose. d. Gastric varices. e. Esophageal and gastric varices. f. Accessory spleen.

Fig. 2: Ultrasonic appearance: The hepatic capsule was smooth and the echo of the liver parenchyma was slightly enhanced, but homogenous. The portal vein was tortuous with a thickened and echo enhanced wall. The inside diameter of PV was from 0.28 cm to 0.6 cm and the flow rate was 0.11m/s. The inside diameter of the splenic vein was 0.8 cm. The ultrasonic appearance of the pancreas, gallbladder and common bile duct were all normal.
The results of color Doppler ultrasonography, shown in Fig. 2, unveiled the following: 1) Absence of the pulmonary artery. 2) Enhancement of the liver parenchyma echo. This describes the thick wall of the portal vein and the enhanced echo of the wall. The vein was tortuous and the velocity of blood flow was slow, which was consistent with CTPV. 3) Splenomegaly associated with the widened splenic vein. 4) Atrial-septal defect (ASD, 5.7 mm) associated with light tricuspid regurgitation.
Based on patient history and physical and other tests, the following final diagnoses were made: 1) congenital left pulmonary hypoplasia associated with an absent left pulmonary artery, left mediastinum, and right emphysema; 2) primarily CTPV, portal hypertension and splenomegaly; 3) ASD, congenital anal atresia (after anoplasty), and spina bifida; 4) pneumonia and pleurisy; 5) secondary thrombocytopenia.
Unfortunately, the patient had no indication for major surgical procedures for his abnormalities. Cefapime was used for bacterial pneumonia and pleurisy. Symptomatic and supportive treatments, such as oxygen therapy, IVIG and oral drugs to facilitate expectoration and suppress his cough until the boy was discharged from hospital after his pneumonia and pleurisy were cured. No surgery was performed after his discharge. Unfortunately, the boy died due to uncontrollable massive hemorrhage of digestive tract after 6 months.
There were few cases regarding other congenital malformations being associated with pulmonary hypoplasia (estimated incidence of total pulmonary agenesis is 0.0034–0.0097%[3-5]). When treating patients with pulmonary atelectasis fails to respond to antibiotic therapy, physicians should think on the possibility of pulmonary hypoplasia, especially in children. Though highly improbable, pulmonary hypoplasia may be associated with multiple abnormalities. CT angiography and color Doppler ultrasonography will be helpful to diagnose accompanying malformations, such as CTPV, in patients with pulmonary hypoplasia. In addition, more studies are needed to better understand the etiology, occurrence and treatment of this rare abnormality.