
Fulltext
Pediatric tuberculosis (TB) includes asymptomatic primary infection, progressive pulmonary TB and extra-pulmonary disease. Skeletal TB occurs in 1-6% of the extra-pulmonary cases commonly involving spine (50-65%), hip and knee joints[1]. Primary TB involving sternum is uncommon often causing a delay in clinical suspicion and diagnosis[2,3]. We report a 5 year-old with primary sternal tuberculous osteomyelitis presenting late with discharging sinus.
A 5-year-old girl from poor socio-economic status presented with increasing dull-aching pain and discharge from a non-traumatic ulceration on the anterior chest wall over the body of sternum for the last 3 months along with low grade fever and reduced appetite. She had been previously treated as pyogenic osteomyelitis but the swelling progressed to ulcerate. She had contact with her neighbor having sputum positive pulmonary TB on anti-tubercular drugs for the last 4 months.
Examination revealed her weight (12 kg) and height (117 cm) were both below 5th centiles. In the upper third of the body of the sternum, there was a tender, discharging ulcer 7cm × 9 cm, surrounded by indurated, erythematous skin with serous, odorless discharge oozing from its sinus which extended up to the bone (Fig. 1). Other than mild pallor, her clinical examination was unremarkable. Scar of BCG vaccination was present.
Her hemogram showed hemoglobin 8.7 mg/dL (microcytic, hypochromic anemia) with total leukocyte count of 10,000/cu mm and differential of 72% lymphocytes. ESR was 80 mm in 1st hour.

Fig.1: Discharging ulcer 7cm × 9 cm, surrounded by indurated, erythematous skin with oozing serous discharge in the upper part of body of the sternum
ELISA test for HIV I and HIV II antibody was negative. Serum IgA level was within normal limit – 120 mg/dl (reference: 80-170mg/dl). Chest X-ray (lateral view) showed cortical breach, erosion of upper third of sternal body with retrosternal soft tissue calcification (Fig. 2). Chest X Ray (PA view) did not show any evidence of pulmonary tuberculosis. Tuberculin test with 5 TU was positive with an induration of 15 mm × 17
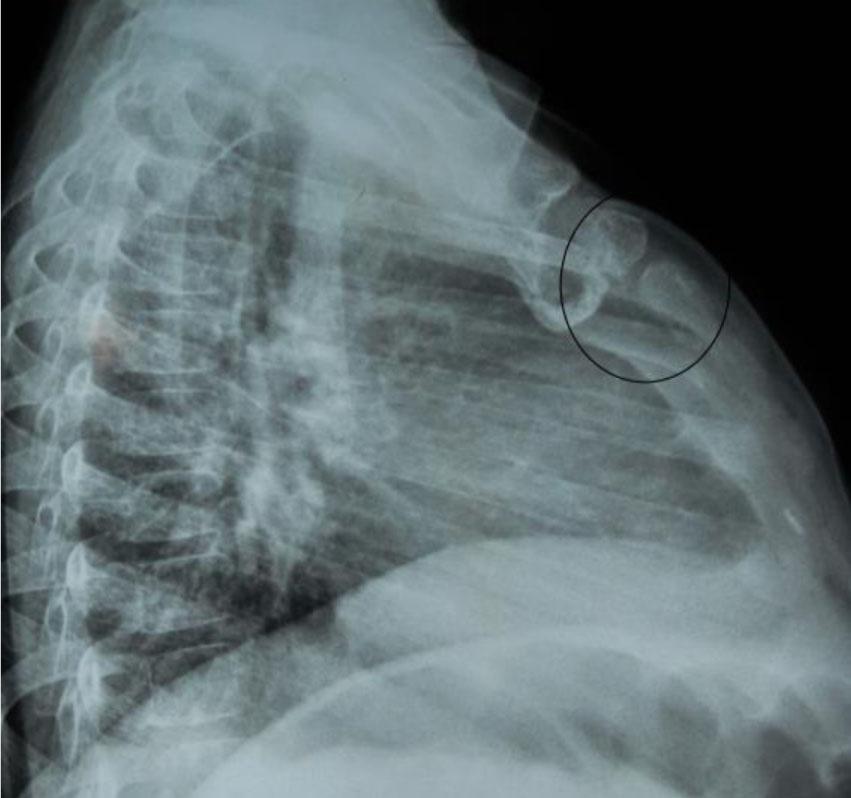
Fig. 2: Chest X-ray (lateral view) showing cortical breach and erosion of upper third of sternal body
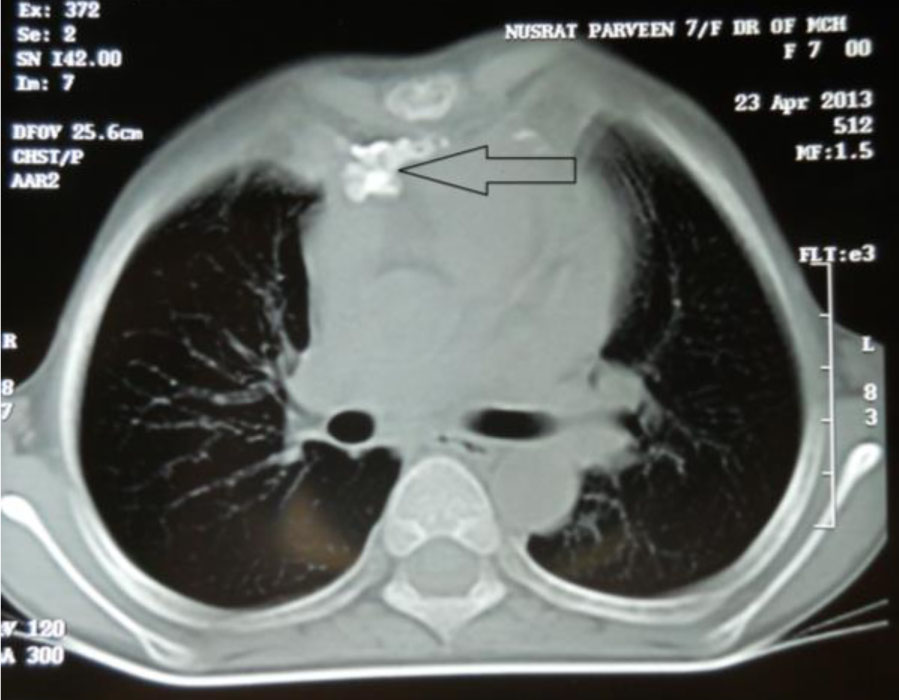
Fig. 3: CT Scan demonstrating defect in the upper part of the sternum with retrosternal soft tissue calcification, hilar and paratracheal lymphadenopathy.
mm after 72 hours. Chest contrast enhanced computerized tomography demonstrated a defect in the upper part of the sternum with retrosternal soft tissue calcification, hilar and paratracheal lymphadenopathy (Fig. 3). Excision biopsy revealed acid fast bacilli on Ziehl-Neelsen staining and histological examination showed caseous necrosis with an accumulation of epithelioid cells and Langhan’s giant cells. TB culture did not show any growth after 6 weeks of incubation. A diagnosis of TB was made on the basis of characteristic tuberculous histopathology and a positive smear for acid-fast bacilli.
The patient was started on antitubercular therapy (ATT) with 4 drug regimen - isoniazid, rifampicin, ethambutol and pyrazinamide - for 2 months and rifampicin and isoniazid for next 7 months. The wound healed without any complications after 3 months leaving only a scar at the site. Follow up of the patient monthly till 12 months until now did not reveal any further problem.
Less than 35 similar cases have been reported in the world literature[4-6] predominantly in adult patients[2]. Only 20% of pediatric TB have skeletal involvement[7] mainly involving the spine. McLellan reviewed 20 cases of sternal osteomyelitis and only 2 cases were found to be from the pediatric age group[8].
Sternal osteomyelitis of tuberculous origin is generally caused by reactivation of latent foci of primary TB or direct extension from contiguous mediastinal lymph nodes[2]. Concomitant extrasternal TB was found in 40% cases reviewed by McLellan et al[8].
The gold standard for diagnosis is culture of Mycobacterium tuberculosis from bone tissue. Surgical exploration is preferred because positive culture yield in needle aspiration is less[8].
The optimal treatment of sternal TB is debated. While some believe that medical treatment with ATT alone is effective, the others believe in medical treatment with aggressive debridement. Current recommendations for the treatment of osseous tuberculosis include a 2-month initial phase of isoniazid, rifampicin, pyrazinamide, and ethambutol followed by a 6 to 12 month regimen of isoniazid and rifampicin[6]. In our case we treated the patient successfully with multidrug therapy after excision biopsy similar to Khan et al[7]. Surgical excision with primary closure is recommended for patients who fail to improve after 3-4 weeks of ATD or have deformed bone structure with sinus formation[8]. Therefore, tuberculous osteomyelitis should be excluded in children with undiagnosed bone lesions. The lack of suspicion of tuberculosis may lead to a delay in the diagnosis with subsequent spread of the disease.