



1. Background
Medical radiation constitutes 96% of radiation of which pediatric radiology with 300 million studies per year, makes up 10% of them. Conventional radiography is frequently performed in pediatric wards and despite technological advances, it has maintained its role in medicine (1). Although radiography is an essential part of medicine, it harbors some hazards. Lack of knowledge of radiation safety is the main cause of inadequate protection in some centers (2).
There are some researches which have measured radiation dose in patients in pediatric hospitals during their hospital stay and made useful suggestions. However, our knowledge of radiation safety in our hospital is limited as there has not been any study in this respect so far. Additionally, there are some differences in results between different studies which justifies designing a new study to determine whether our protocols of radiography meet the standard regulations.
2. Objectives
In this study, we aimed to measure exposure dose which patients usually receive directly from X-ray machine as well as the scattered radiation produced around them which can be absorbed unwantedly by other patients. This measurements enable us to make a comparison with the standard recommended doses and can be of great use in modifying our protocol and guidelines to minimize the radiation dose.
3. Methods
This descriptive, analytical study was conducted in our hospital in 2017. First, ethical approval was issued by ethical committee of Tehran University of Medical Sciences. The sample size was calculated as 84 patients at a margin of error of 5% at 95% confidence level (P = 0.5; Z = 1.96). We selected patients from four units including NICU, NICU-OPEN, CICU, and PICU. We explained to the parents of patients that the study is measuring the amount of radiation received by their children during their hospital stay and that there was no extra X-ray exposition. We also clarified the details of the study and that they were free to participate in the study or to leave when they wanted. All patients for whom a radiography was requested and their parents agreed to enter the study were included and otherwise excluded. The entrance surface dose (ESD) received directly by the patients and scattered radiation at one and two-meter distances from the X-ray tube have been measured.
We selected and divided the patients into three groups. The first group consisted of 24 patients, six from each unit, in whom thermoluminescent dosimetry was performed. In this group, 24 Termoluminescent dosimeters (TLDs) (100 PTW) were placed on the sternum, while one TLD was located in the operating room.
The second and third groups each consisted of 30 cases (seven or eight from each unit). The Geiger-Muller dosimeters (ND-3000) were used to measure scattered radiation at one-meter distances from the X-ray tube for the second group and two-meter distance for the third group. All radiography conditions, including milliampere-seconds (mAs), kilovoltage (kV), radiation field, and the tube-cassette distance, depended on the operator’s decision, and we did not interfere with the selected conditions. The focal length and radiation field were constant in all radiographs, therefore are excluded in our study. The exposure conditions were determined based on the patient’s weight in the anteroposterior and supine positions. After sampling, TLDs were sent to the Physics Laboratory of Tehran University for reading, and Geiger-Muller dosimeters were read during radiography. The collected data were analyzed in SPSS version 16.
4. Results
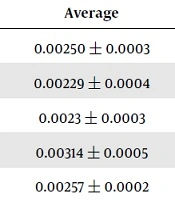
The average ESD was 0.3873, 0.3867, 0.3700, and 0.4033 millisievert (mSv) in U1 to U4 respectively, whereas the scattered radiation doses measured as 0.00986, 0.00750, 0.01250, 0.1014 at one-meter and 0.00250, 0.00220, 0.00238, 0.00314 mSv at two-meter distances. There was no significant difference in radiation dose between those units (P > 0.05) (Tables 1-3).
There was no significant difference between hospital units (Tables 4-6). The ESD depends more on mAs than kV. The scattered dose at one-meter distance depended on weight, not mAs or kV. At two-meter distances, factors including kV and weight had significant relationships with radiation dosage.
| Unit | Milliampere Seconds | Kilovoltage | Entrance Surface Dose (mGy) |
|---|---|---|---|
| U1 | 3.2 | 55 | 0.43 |
| U1 | 3.2 | 55 | 0.4 |
| U1 | 2 | 48 | 0.36 |
| U1 | 2 | 54 | 0.28 |
| U1 | 2 | 64 | 0.39 |
| U1 | 2.8 | 58 | 0.41 |
| U2 | 2.5 | 45 | 0.44 |
| U2 | 4.5 | 50 | 0.41 |
| U2 | 2.5 | 47 | 0.44 |
| U2 | 1.8 | 50 | 0.34 |
| U2 | 1.8 | 49 | 0.33 |
| U2 | 2 | 50 | 0.36 |
| U3 | 3.2 | 55 | 0.4 |
| U3 | 3 | 53 | 0.4 |
| U3 | 3.2 | 50 | 0.45 |
| U3 | 1.8 | 50 | 0.27 |
| U3 | 2.8 | 50 | 0.31 |
| U3 | 2.8 | 55 | 0.39 |
| U4 | 3.2 | 57 | 0.42 |
| U4 | 3.2 | 58 | 0.42 |
| U4 | 2.8 | 53 | 0.4 |
| U4 | 2.8 | 49 | 0.37 |
| U4 | 2.8 | 50 | 0.31 |
| U4 | 4.5 | 55 | 0.5 |
| Unit | Weight (kg) | mAs | Kv | Dose (mSV) |
|---|---|---|---|---|
| U1 | 8 | 8 | 55 | 0.009 |
| U1 | 12 | 2 | 58 | 0.01 |
| U1 | 4 | 2 | 53 | 0.005 |
| U1 | 4 | 1.8 | 57 | 0.006 |
| U1 | 14 | 2 | 58 | 0.02 |
| U1 | 12 | 2 | 54 | 0.012 |
| U1 | 5 | 1.8 | 53 | 0.007 |
| U2 | 4 | 1.8 | 48 | 0.004 |
| U2 | 5 | 1.8 | 50 | 0.005 |
| U2 | 3 | 1.8 | 48 | 0.003 |
| U2 | 5 | 2 | 55 | 0.006 |
| U2 | 8 | 2.5 | 57 | 0.008 |
| U2 | 10 | 2.5 | 58 | 0.012 |
| U2 | 12 | 2 | 56 | 0.01 |
| U2 | 6 | 2 | 56 | 0.012 |
| U3 | 5 | 2 | 55 | 0.008 |
| U3 | 12 | 2 | 58 | 0.01 |
| U3 | 10 | 2.5 | 55 | 0.012 |
| U3 | 12 | 2 | 58 | 0.021 |
| U3 | 14 | 2 | 60 | 0.02 |
| U3 | 7 | 2.5 | 55 | 0.009 |
| U3 | 8 | 2.5 | 58 | 0.013 |
| U4 | 5 | 1.8 | 50 | 0.007 |
| U4 | 6 | 1.8 | 53 | 0.008 |
| U4 | 9 | 1.8 | 55 | 0.01 |
| U4 | 5 | 2 | 55 | 0.008 |
| U4 | 8 | 1.8 | 57 | 0.012 |
| U4 | 9 | 2 | 57 | 0.01 |
| U4 | 13 | 1.8 | 58 | 0.016 |
| U4 | 5 | 1.8 | 52 | 0.007 |
| Unit | Weight (kg) | mAs | Kv | Dose (mSV) |
|---|---|---|---|---|
| U1 | 10 | 2 | 50 | 0.002 |
| U1 | 8 | 1.8 | 46 | 0.002 |
| U1 | 11 | 2 | 50 | 0.003 |
| U1 | 7 | 1.8 | 48 | 0.001 |
| U1 | 10 | 1.8 | 55 | 0.003 |
| U1 | 12 | 2 | 55 | 0.004 |
| U1 | 8 | 2 | 50 | 0.002 |
| U1 | 12 | 2 | 50 | 0.003 |
| U2 | 14 | 2 | 55 | 0.003 |
| U2 | 7 | 1.8 | 47 | 0.001 |
| U2 | 10 | 1.8 | 48 | 0.002 |
| U2 | 12 | 2 | 50 | 0.003 |
| U2 | 14 | 2 | 55 | 0.004 |
| U2 | 5 | 1.8 | 48 | 0.002 |
| U2 | 4 | 1.8 | 48 | 0.001 |
| U3 | 12 | 2 | 52 | 0.004 |
| U3 | 11 | 2 | 55 | 0.003 |
| U3 | 12 | 2 | 56 | 0.003 |
| U3 | 8 | 2 | 48 | 0.002 |
| U3 | 6 | 1.8 | 46 | 0.001 |
| U3 | 7 | 1.8 | 50 | 0.002 |
| U3 | 14 | 2 | 55 | 0.003 |
| U3 | 7 | 1.8 | 46 | 0.001 |
| U4 | 9 | 1.8 | 55 | 0.003 |
| U4 | 10 | 2 | 57 | 0.003 |
| U4 | 7 | 2 | 50 | 0.002 |
| U4 | 5 | 1.8 | 48 | 0.001 |
| U4 | 10 | 2 | 55 | 0.004 |
| U4 | 9 | 1.8 | 58 | 0.004 |
| U4 | 12 | 2 | 57 | 0.005 |
| Unit | Number | Average |
|---|---|---|
| NICU | 6 | 0.3783 ± 0.21 |
| NICU-OPEN | 6 | 0.3867 ± 0.20 |
| CICU | 6 | 0.3700 ± 0.02 |
| PICU | 6 | 0.4033 ± 0.02 |
| Total | 24 | 0.3846 ± 0.01 |
| Unit | Number | Average |
|---|---|---|
| NICU | 7 | 0.00986 ± 0.0019 |
| NICU-OPEN Heart | 8 | 0.00750 ± 0.0012 |
| CICU | 8 | 0.01250 ± 0.0018 |
| PICU | 7 | 0.01014 ± 0.0011 |
| Total | 30 | 0.01000 ± 0.0008 |
| Unit | Number | Average |
|---|---|---|
| NICU | 8 | 0.00250 ± 0.0003 |
| NICU-OPEN Heart | 7 | 0.00229 ± 0.0004 |
| CICU | 8 | 0.0023 ± 0.0003 |
| PICU | 7 | 0.00314 ± 0.0005 |
| Total | 30 | 0.00257 ± 0.0002 |
5. Discussion
Pediatric radiology constitutes about 10% of all radiological studies. About 1% of neonates in North America are premature, and many of them need radiological examinations. Likewise, the frequency of congenital heart disease is 0.5% to 0.8% among term and 2% in immature neonates which increases demand for radiography. Radiography is essential for lower respiratory infections and may obviate the need for antibiotic therapy. In some hospitals, nearly half of radiology examinations, especially chest X-rays, are performed by portable machines (3). Apart from radiation absorbed directly by patients, other patients near the portable machine are also exposed.
Children are more susceptible to radiation than adults. The risk of cancer, genetic effects, and other significant disorders is two to three times higher among children than adults due to their higher cellular proliferation rate and smaller body size which exposes them to higher radiation (4). Age is an important factor. In childhood, cells with a high proliferation rate are susceptible to cancer because when mutation in DNA occurs, damaged cells continue to proliferate, and cause cancers. As with Hiroshima and Nagasaki survivors, patients younger than 10 years who had a radiotherapy, are more prone to thyroid, bone marrow, and breast cancers. Radiography normally exposes most parts of the neonate’s body due to its small size. This non-target exposure result in an increased risk of malignancy. There are two types of radiation effects. First, primary or early effects like skin redness, cell necrosis, and growth retardation after epiphyseal exposure which occur inevitably and are dose-dependent (5). The second type of these effects which depends on chance includes cancer, leukemia, and short life-span, which are the late effects of radiation. These effects do not have a certain threshold and may occur even with the lowest radiation dose. When X-ray passes through tissues, it produces high-speed electrons and secondary radiation. High-speed electrons cause ionization and destruction of atomic structures, leading to biological errors. These electrons are produced by photoelectric effects, Compton scattering, and pair production. On the other hand, secondary radiation includes scattered radiation, characteristic radiation, and annihilation radiation.
Radiography dose depends on some factors, such as kilovoltage (KV), milliampere (mA), time of exposure, and inverse square of the distance to the X-ray tube (1). There are different types of dosimeters. Thermo luminescent dosimeters (TLDs), which are commonly used in radiology centers, offer the advantages of simplicity, high spatial resolution, and recording of radiation exposure beyond any time limitations (6). The second type of dosimeter, which is used in research, is the Geiger-Muller dosimeter - a highly sensitive dosimeter for measuring scattered radiation (6).
Careful measurement of pediatric radiation is important, as radiography is being increasingly performed in children. Therefore, it is crucial to measure radiation doses and make comparisons with the standards. Our goal was to measure the radiation dose a patient receives during his or her stay in our hospital and also scattered radiation created at one and two-meters distances from the radiation source to find a safe distance where there is no major radiation. The average doses for a patient, om the distance of one and two-meters were 0.3846, 0.0100, and 0.0026 respectively. In a study by Bahreyni Toossi et al, ESD was measured in 195 neonates. The absorbed dosage was nearly 0.76 mSv for each radiographic examination (7), while in our study, the absorbed dosage was 0.38, which is lower than their results. Also, Abdelhalim at a center in Saudi Arabia showed that radiation can be decreased by reducing mAs. They also stated that radiographers do not justify the focal length and radiation field (8). Pediatric radiology is challenging for specialists, as there are different limits for radiation doses in different institutions. The International Commission on Radiological Protection (ICRP) has established a reference dose for diagnostic examinations. The National Council on Radiation Protection and Measurements (NCRP) and the International Atomic Energy Agency (IAEA) have developed some regulations for pediatric radiology. The permitted radiation dose in a particular period should not exceed 1 mSv. Also, it is recommended that the radiation dosage should not exceed 0.1 mSv per each radiograph for children and 0.08 for neonates. At our center, the average hospital stay was two weeks, and 15 to 20 portable radiographies were done every day. Each patient underwent three radiographs and received scattered radiation three to five times during hospitalization. In our hospital, ESD ranged from 0.3 to 0.5 mSv for each radiographic exam, which is three to four times higher than the recommended level of 0.1 mSv.
We measured the radiation dose and found that it is far higher than its standards, but it was the first step. We took a limited sample which could be higher than that. We also could implement the protective measures and make a comparison, but we did not. Therefore, we recommend that the next study considers all these downfalls and designs to evaluate the efficacy of protective methods.
5.1. Conclusion
We can conclude that the radiation received by our patients usually exceeds the maximum recommended dose.
As the reduction of mAs can decrease radiation, we emphasize on the training of radiographers to justify the conditions of exposure. If radiographers adjust the focal length and radiation field appropriately, radiation will be minimized. Additionally, physicians should be encouraged to limit the requests for X-ray as much as possible. Appropriate shielding and a three-meter distance from the tube are also recommended to avoid scattered radiation. We believe that there is a need for dosimetry in CT studies to measure the radiation dose and find a way of controlling its hazards.
