1. Background
Violent acts are patterns of behavior internalized by new generations through the socialization process and transmitted to other generations (1). Domestic violence is one of the most common forms of violence against women, which can occur in any intimate relationship. Domestic violence is mainly perpetrated by men against women. Due to the high frequency and severity of this type of violence, it has become a significant public health issue (2). Intimate partner violence (IPV), often referred to as domestic violence, can take many forms. Non-physical violence is classified into four types of emotional, psychological, social, and economic violence. Meanwhile, physical and sexual violence against women refers to acts of physical aggression against women (3, 4). National surveys of family violence around the world show that women are six times more likely to be harmed than men and that 10 - 50% of them have been beaten or physically assaulted by an intimate partner at some point in their lives.
Each year, four million women are assaulted by a domestic partner. According to some statistics, one-third of women are victims of domestic violence during their lifetime (5). Pregnancy and childbirth can be a period of vulnerability to violence due to changes in women’s physical, emotional, social, and economic needs. Pregnancy alone imposes significant mental and physical pressure on women (6). Therefore, when it is combined with other stressful factors, such as violence, it can negatively affect the health of the mother and child. Violence against a pregnant woman and an unborn fetus, either directly or indirectly, can have severe consequences for their physical and mental health (7). Recently, based on a review of 86 studies, the prevalence of IPV against women was estimated at 1.5 - 66.9% during pregnancy and 2 - 58% during the postpartum period (8). In a systematic meta-analysis conducted in 2022 in Iran, the overall prevalence of IPV was reported to be 51.5% (9).
According to previous research, focusing on the social determinants of health in discussions about violence against women can help us to better understand this issue (10). Over the past two decades, the public health community has paid increasing attention to the social determinants of health. Apart from medical care, social factors can strongly influence a person’s health status, either independently or through interactions with other factors (11). The World Health Organization (WHO) Commission on Social Determinants of Health has proposed three general categories of health determinants, including social, economic, and political factors (e.g., government, political institutions, economic processes, culture, and performance of the social system). The structural factors creating social classes include education, employment status, income, sex, and ethnicity (race). The intermediary factors include psychosocial circumstances, behavioral circumstances, and health systems. These intermediary factors can be categorized into material conditions (e.g., living and working conditions, residence status, and access to food and health services), psychosocial factors (e.g., stress, anxiety, depression, and social support), behavioral and biological factors (e.g., smoking, alcohol consumption, nutrition, and physical activity), and health system (state of healthcare and access to health services) (12, 13).
Studies have shown that several individual and social factors, such as age, level of education, employment status of women and their partners, social insurance, immigration status, place of living, age of marriage, year of women’s marriage, monthly income, and family and cultural differences, are effective in the occurrence of violence against women (14, 15). Several risk factors have been identified for domestic violence against pregnant women, such as being single, having a low education level, low socioeconomic status, and unwanted pregnancy (16). Overall, the high level of violence in different societies suggests that it is a multidimensional social issue, which is probably exacerbated by structural factors (17).
Most studies have focused on violence against women in the general population. For this reason, it is essential to fully understand this issue during pregnancy and analyze its various aspects. Considering the variations in the cultural background of different study populations, the prevalence of IPV may be higher in certain groups. For instance, women who experience critical life events, such as motherhood, may face an increased risk of IPV due to the intersection of these events with existing risk factors. Therefore, it is important to address the predisposing factors for violence against women, especially during pregnancy. Nevertheless, studies on the relationship between domestic violence and predisposing factors of violence in pregnancy are still scarce.
Violence against women during pregnancy poses a threat to the physical and mental health of both the mother and fetus and, ultimately, to public health. Therefore, the present study aimed to investigate the social determinants of domestic violence in pregnant women and to determine their association with domestic violence among Iranian pregnant women.
2. Objectives
This study aimed to determine the relationship between the structural determinants of health and domestic violence against pregnant women based on the WHO model. According to the WHO model, the social determinants of health were considered to be structural socioeconomic factors, such as income, education, and employment. Individual and gynecologic factors, such as age and history of pregnancy and delivery, were also investigated.
3. Methods
3.1. Study Type and Sampling Criteria
The final sample size was calculated according to the outcomes with the lowest prevalence rate (P = 0.001 - 0.002%) (18). Considering an attrition rate of 10 - 15%, the final sample size was calculated at 560:
Additionally, the sample size was determined with respect to each goal of the study. The sample size for evaluating the relationship between SDH and domestic violence was 303 with respect to a prevalence rate of (P = 0.05, d = 27%) (19).
In addition, with regard to the sampling method (cluster sampling) and design effect of 2, the sample size was measured at 500. Since the sample size for the main purpose of the study, it was larger than the target sample size, a larger population was considered as the main sample size (n = 560). Finally, a total of 560 eligible pregnant women, who were referred to selected health centers in Tehran, Iran, were recruited. This study was conducted from November 2020 (11/20/2020) until September 2021 (8/23/2021). Sampling was carried out after obtaining permission from the Council of Shahid Beheshti University of Medical Sciences (SBUMS), as well as a license and code of ethics (IR.SBMU.PHARMACY.REC.1401.115), and obtaining permission from the officials of the hospital and selected clinics. Moreover, the research objectives were explained to the participants, and written informed consent was obtained for completing the questionnaires. Besides, the confidentiality of their information and rights of withdrawal was ensured.
3.2. Inclusion and Exclusion Criteria
The inclusion criteria were being literate and able to read and write in the Persian language, gestational age of 28 - 35 weeks, absence of known medical problems preventing participation in the study, and willingness to participate in the study. On the other hand, the exclusion criteria were incomplete questionnaire items and medical or obstetric disorders in the mother (e.g., pregnancy-induced hypertension, chronic hypertension, overt diabetes, and gestational diabetes).
3.3. Sampling
A multistage cluster sampling method was used to select participants among the attendees of health centers affiliated with SBUMS in Tehran, Iran. First, the city of Tehran was divided into four regions (north, south, west, and east), and then, a governmental hospital was randomly selected in each region. A quota was allocated to each hospital based on the statistics of monthly visits of pregnant women to pregnancy care clinics. All eligible women with a gestational age of 28 - 35 weeks were included in the study. After obtaining written consent from the participants, data were collected using different tools. Due to the COVID-19 pandemic in Iran coinciding with the research, part of the sampling was done by designing electronic forms and sending them to pregnant mothers on social networks. To encourage participation in the study, the research units were given the flexibility to complete the questionnaires at their convenience, both in terms of time and location. The participants were also informed that they could discuss any questions related to reproductive health with the researcher. Besides, if desired, the participants could access the educational materials provided by the researcher in a virtual educational group (on WhatsApp) on topics such as maternal and child health, breastfeeding counseling, vaccination, and the COVID-19 pandemic, to address their questions. The necessary follow-up was done by the researcher.
3.4. Data Collection Tools
Three questionnaires were used in this study to collect data, including a Demographic/Obstetric Questionnaire, the socioeconomic status (SES) Short-Form Questionnaire, and the Domestic Violence Questionnaire (DVQ).
3.4.1. Demographic/Obstetric Questionnaire
This questionnaire contained 35 questions on factors such as pregnant women’s age, spouse’s age, marital status, ethnicity, gestational age, number of pregnancies, the interval between pregnancies, type of pregnancy (wanted or unwanted), and use of supplements. This questionnaire was based on the study of authentic scientific books and articles and was in line with the research objectives. To determine its validity, pregnant mothers from the target group commented on the items of the questionnaire in terms of the level of difficulty, appropriateness, and ambiguity, and all the items were confirmed. Also, its validity was confirmed while making the necessary revisions by 10 specialists, including 8 faculty members of Shahid Beheshti University of Medical Sciences (social determinants of health, reproductive health) and 2 instrument making and psychometrics specialists.,
3.4.2. Socioeconomic Status Short-Form Questionnaire
The socioeconomic status questionnaire used in this study was the SES questionnaire by Ghodratnama (2013), which contains four components, including income, economic class, education, and housing status (20). Out of 10 questions in this questionnaire, eight questions (related to income adequacy, economic class, level of parents’ education, housing cost, financial ability to buy housing, income adequacy, financial concerns, and satisfaction with the transportation vehicle) were rated on a five-point Likert scale. Two separate questions were used to evaluate the size of the house and the number of people living in the household. The questions in the SES questionnaire use a five-point measurement scale, with scores ranging from 1 (very low) to 5 (very high); the range of scores is 7 - 40. A score of 7 - 17 represents a low socioeconomic status, a score of 18 - 28 represents an average socioeconomic status, and a score of 29 - 40 represents a high socioeconomic status. Eslami et al. confirmed the face and content validity of this questionnaire (21). Also, the reliability of this tool was evaluated in our study using Cronbach's alpha test (0.83).
3.4.3. Domestic Violence Questionnaire
This questionnaire, developed by the WHO, evaluates physical, sexual, and emotional violence of the sexual partner during pregnancy on a five-point Likert scale. One positive response to the questionnaire items indicates the presence of violence against the pregnant woman. The validity of this questionnaire has been confirmed in multiple Iranian studies, and its Cronbach's alpha coefficient was measured to be 0.92, 0.89, and 0.88 for the physical, emotional, and sexual domains, respectively (22).
3.5. Statistical Analysis
Data were analyzed using descriptive (mean, standard deviation, frequency, and percentage) and inferential (chi-square test and logistic regression analysis) methods in SPSS version 24. A P-value less than 0.05 was considered statistically significant.
4. Results
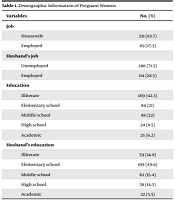
In this study, 600 questionnaires were distributed among the participants. With a response rate of 93%, a total of 560 questionnaires were completed and analyzed. The average age of women and their spouses was 27.02 ± 4.340 and 32.34 ± 5.540 years, respectively. The results did not indicate a significant relationship between domestic violence and the age of women or their spouses (P > 0.05). Most of the participants (32.9%) had secondary school education. Women and their spouses with elementary school education showed the highest average score of domestic violence compared to other educational groups (P = 0.000).
In this study, the majority of women (n = 427, 76.25%) had a wanted pregnancy. The highest average score of domestic violence was reported in women with an unwanted pregnancy. Most of the mothers (n = 233, 41.6%) were housewives, and 330 (58.9%) of their spouses were employed. In terms of occupational status, a significant relationship was observed between the average domestic violence scores of women and their spouses (P = 0.000); the highest average score of domestic violence was reported by working mothers. Also, the results showed that mothers whose spouses were employed had experienced minor violence (4.17%), while women with unemployed spouses had experienced the highest level of violence (61.36%).
The highest average scores of domestic violence were reported in women with more pregnancies (≥ 4), and the difference was statistically significant (P = 0.000). The majority of women (n = 289, 51.6%) were married at the age of 29 - 35 years. The average scores of domestic violence in mothers who were married at a younger age (18 - 28 years) were lower than others. In this age group of women, the birth of the first child accounted for the highest average score of domestic violence, which was statistically significant (P = 0.000) (Table 1). The analysis of different dimensions of domestic violence against women showed that 10.2% of pregnant women had experienced physical violence, 9.0% had experienced sexual violence, and 66.3% had experienced emotional violence.
Table 1.
The Demographic and Obstetric Characteristics of Pregnant Women and Their Relationship with Domestic Violence
| Variables | No. (%) | Mean ± SD | Statistical Test (Sig) |
|---|---|---|---|
| Woman’s age (y) | χ2 = 2.38, Sig = 0.666 | ||
| 18 - 22 | 48 (8.75) | 8.04 ± 5.90 | |
| 23 - 27 | 248 (44.28) | 10.17 ± 10.55 | |
| 28 - 32 | 165 (29.46) | 9.55 ± 2.99 | |
| 33 - 37 | 87 (16) | 16.02 ± 5.62 | |
| < 37 | 12 (2) | 4.83 ± 2.66 | |
| Spouse’s age (y) | χ2 = 8.75, Sig = 0.133 | ||
| 18 - 22 | 90 (16.1) | 7.67 ± 2.34 | |
| 23 - 27 | 100 (17.8) | 11.21 ± 3.74 | |
| 28 - 32 | 158 (28.2) | 13.34 ± 4.11 | |
| 33 - 37 | 171 (30.5) | 15.24 ± 3.97 | |
| < 37 | 41 (7.3) | 10.25 ± 5.12 | |
| Woman’s education | χ2 = 56.62, Sig = 0.000 | ||
| Elementary school | 171 (30.5) | 55.09 ± 17.74 | |
| Secondary school | 184 (32.9) | 10.78 ± 4.23 | |
| Middle school | 182 (32.5) | 8.74 ± 3.32 | |
| High school | 23 (4.1) | 6.43 ± 2.78 | |
| Spouse’s education | χ2 = 165.39, Sig = 0.000 | ||
| Elementary school | 101 (18) | 24.02 ± 0.14 | |
| Secondary school | 143 (25.5) | 14.81 ± 4.01 | |
| Middle school | 265 (47.3) | 5.11 ± 2.12 | |
| High school | 51 (9.1) | 1.96 ± 0.36 | |
| Wanted pregnancy | Z = 12.47, Sig = 0.000 | ||
| Yes | 427 (76.25) | 3.53 ± 1.51 | |
| No | 133 (25.75) | 13.20 ± 2.73 | |
| Woman’s occupation | χ2 = 39.99, Sig = 0.000 | ||
| Housewife | 233 (41.6) | 8.96 ± 2.84 | |
| Self-employed | 31 (5.5) | 1.33 ± 0.94 | |
| Government employee | 185 (33) | 12.52 ± 3.09 | |
| Private sector employee | 111 (19.8) | 13.56 ± 5.01 | |
| Spouse’s occupation | χ2 = 224.88, Sig = 0.000 | ||
| Unemployed | 11 (2) | 61.36 ± 5.92 | |
| Self-employed | 118 (21.1) | 21.30 ± 5.64 | |
| Government employee | 330 (58.9) | 4.17 ± 2.19 | |
| Private employee | 101 (18) | 13.71 ± 3.63 | |
| Number of pregnancies | χ2 = 297.051, Sig = 0.000 | ||
| 1 | 300 (53.6) | 12.07 ± 5.86 | |
| 2 | 161 (28.8) | 3.83 ± 1.49 | |
| 3 | 88 (15.7) | 21.98 ± 1.23 | |
| ≤ 4 | 11 (2) | 36.36 ± 5.92 | |
| Age at marriage (y) | χ2 = 304.243, Sig = 0.000 | ||
| 18 - 28 | 50 (8.9) | 3.18 ± 1.27 | |
| 29 - 35 | 289 (51.6) | 4.05 ± 2.12 | |
| ≥ 35 | 221 (39.5) | 16.93 ± 6.02 | |
| Woman's age at birth of the first child (y) | χ2 = 46.334, Sig = 0.000 | ||
| 18 - 28 | 136 (24.3) | 13.65 ± 5.62 | |
| 29 - 35 | 238 (42.5) | 12.28 ± 4.44 | |
| ≥ 35 | 186 (33.2) | 7.95 ± 3.21 | |
| History of cesarean section | Z = 1.23, Sig = 0.11 | ||
| Yes | 166 (29.6) | 10.06 ± 2.97 | |
| No | 394 (70.4) | 10.85 ± 3.40 | |
| History of abortion | Z = 1.57, Sig = 0.091 | ||
| Yes | 119 (21.3) | 9.20 ± 4.72 | |
| No | 441 (78.8) | 11.00 ± 4.26 |
The results showed that 270 (48.2%) women had an average socioeconomic status. The majority of women (n = 206, 36.8%) had sufficient income. The lowest education levels of women's parents (father and mother) were secondary education and high school, respectively, while the highest frequency was attributed to middle school in both parents. Based on the findings, the average score of domestic violence in women whose parents had elementary school education was higher than that of other educational levels. Overall, a significant relationship was observed between the majority of socioeconomic status dimensions and the average scores of domestic violence in pregnant women (P < 0.005) (Table 2).
Table 2.
The Socioeconomic Characteristics of Pregnant Women and Their Relationships with Domestic Violence
| Variables | No. (%) | Mean ± SD | Statistical Test (Sig) |
|---|---|---|---|
| Income/financial ability to afford the costs of living | χ2 = 297.304, Sig = 0.020 | ||
| Totally inadequate | 60 (10.7) | 24.67 ± 3.12 | |
| Inadequate | 51 (0.9) | 24.02 ± 0.14 | |
| Somewhat enough (acceptable) | 78 (1.63) | 16.64 ± 2.75 | |
| Adequate | 206 (36.8) | 7.90 ± 3.88 | |
| Highly adequate | 165 (29.5) | 2.4121 ± 1.14 | |
| Family’s economic class (household income) | χ2 = 224.657, Sig = 0.000 | ||
| Very low | 60 (10.7) | 64.67 ± 2.12 | |
| Low | 10 (1.78) | 61.60 ± 3.27 | |
| Medium | 270 (48.2) | 18.38 ± 7.48 | |
| High | 112 (20) | 17.56 ± 4.04 | |
| Very high | 108 (19.3) | 4.056 ± 1.75 | |
| Parents’ education (father) | χ2 = 47.091, Sig = 0.000 | ||
| Elementary school | 107 (19.2) | 16.25 ± 3.765 | |
| Secondary school | 179 (32) | 11.54 ± 3.15 | |
| Middle school | 181 (32.3) | 9.23 ± 3.10 | |
| High school | 93 (16.6) | 8.41 ± 2.73 | |
| Parents’ education (mother) | χ2 = 8.573, Sig = 0.036 | ||
| Elementary school | 181 (32.3) | 18.01 ± 5.32 | |
| Secondary school | 63 (11.2) | 12.21 ± 2.85 | |
| Middle school | 228 (40.7) | 10.24 ± 2.96 | |
| High school | 86 (15.3) | 7.35 ± 1.56 | |
| Housing cost | χ2 = 156.96, Sig = 0.10 | ||
| Very low | 99 (24.5) | 61.53 ± 5.013 | |
| Low | 104 (25.7) | 31.60 ± 6.27 | |
| Medium | 123 (30.4) | 18.97 ± 7.48 | |
| High | 63 (15.6) | 9.56 ± 4.54 | |
| Very high | 15 (3.1) | 8.08 ± 2.75 | |
| Ability to buy housing | χ2 = 17.623, Sig = 0.065 | ||
| Very low | 62 (39.7) | 61.53 ± 5.013 | |
| Low | 56 (35.9) | 31.60 ± 6.27 | |
| Medium | 15 (9.6) | 18.97 ± 7.48 | |
| High | 14 (9) | 9.56 ± 4.54 | |
| Very high | 9 (5.8) | 8.08 ± 2.75 | |
| Having money for independent spending | χ2 = 25.221, Sig = 0.066 | ||
| Highly sufficient | 161 (28.75) | 4.94 ± 2.53 | |
| Sufficient | 93 (16.6) | 6.62 ± 2.25 | |
| Somewhat enough (acceptable) | 99 (17.68) | 10.13 ± 4.21 | |
| Low amount | 156 (27.8) | 17.46 ± 5.53 | |
| Insufficient | 51 (9.1) | 24.04 ± 9.28 | |
| Financial concerns | χ2 = 212.283, Sig = 0.000 | ||
| Always | 89 (1.9) | 12.29 ± 5.53 | |
| Mostly | 120 (21.4) | 11.87 ± 5.03 | |
| Sometimes | 100 (17.8) | 10.32 ± 3.51 | |
| Rarely | 142 (25.3) | 9.83 ± 4.89 | |
| Never | 109 (19.5) | 9.23 ± 4.15 | |
| Satisfaction with the transportation vehicle | χ2 = 276.003, Sig = 0.200 | ||
| Very satisfied | 110 (23.6) | 13.99 ± 1.56 | |
| Satisfied | 51 (10.9) | 6.10 ± 5.272 | |
| Neither satisfied nor dissatisfied | 68 (14.6) | 24.02 ± 5.18 | |
| Dissatisfied | 238 (51) | 32.57 ± 10.54 | |
| Living area (m2) | χ2 = 106.629, Sig = 0.000 | ||
| < 60 | 110 (19.6) | 18.71 ± 4.83 | |
| 60 - 70 | 79 (14.1) | 12.56 ± 6.57 | |
| 71 - 80 | 187 (33.4) | 8.98 ± 3.48 | |
| 81 - 90 | 123 (22) | 7.26 ± 3.54 | |
| ≥ 91 | 61 (10.9) | 4.52 ± 2.75 | |
| Family size | χ2 = 276.003, Sig = 0.000 | ||
| ≤ 2 | 261 (46.6) | 4.19 ± 1.06 | |
| 3 | 112 (20) | 10.10 ± 5.21 | |
| 4 | 119 (21.3) | 14.02 ± 4.18 | |
| ≥ 5 | 68 (12.1) | 22.57 ± 9.04 |
According to the logistic regression model (Table 3), changes in the dependent variable of domestic violence against pregnant women could predict eight significant and independent demographic/obstetric variables at a 73% confidence level. Also, socioeconomic status with 7 significant independent components could predict domestic violence against pregnant women at an 85.3% confidence level (P < 0.005).
Table 3.
| Observed | Predicted | ||
|---|---|---|---|
| Domestic Violence | Percentage Corrected | ||
| No | Yes | ||
| Demographic and obstetric characteristics | |||
| Domestic violence | |||
| No | 0 | 151 | 0.0 |
| Yes | 0 | 409 | 100.0 |
| Overall percentage | 73.0 | ||
| Socioeconomic status | |||
| Domestic violence | |||
| No | 0 | 151 | 0.0 |
| Yes | 0 | 409 | 100.0 |
| Overall percentage | 85.3 | ||
a Constant is included in the model.
b The cut value is 0.500.
The results of binary logistic regression analysis (Tables 4 and 5) revealed that the education level of women and their spouses was influential in domestic violence. The analysis of the relationship between women’s education and domestic violence showed that the probability of domestic violence was reduced by 69%, 51%, and 37% in women with high, middle, and secondary education, respectively, compared to primary education as the reference group (a positive effect). It was also found that women whose spouses had higher education levels were about 50% less likely to experience domestic violence by their spouses compared to the reference group (with primary education) (CI: 0.48 - 0.543; OR = 0.512).
Table 4.
Simultaneous Modeling of Demographic Characteristics on Domestic Violence in Pregnant Women
| Variables | B | SE | Wald | EXP b | 95% CI for EXP b | Sig | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Woman’s education | |||||||
| Elementary school (Ref.) | 3.199 | 0.003 | |||||
| Secondary school | -0.460 | 0.348 | 1.752 | 0.631 | 0.319 | 1.247 | 0.332 |
| Middle school | -0.716 | 0.453 | 2.498 | 0.488 | 0.201 | 1.188 | 0.100 |
| High school | -0.731 | 0.077 | 90.127 | 0.310 | 0.159 | 0.461 | 0.031 |
| Spouse’s education | |||||||
| Elementary school (Ref.) | 1.270 | 0.000 | |||||
| Secondary school | 0.035 | 0.376 | 0.009 | 1.036 | 0.496 | 2.163 | 0.666 |
| Middle school | -0.370 | 0.385 | 0.926 | 0.690 | 0.446 | 1.940 | 0.847 |
| High school | -0.127 | 0.016 | 63.004 | 0.512 | 0.481 | 0.543 | 0.004 |
| Wanted pregnancy | -0.710 | 0.139 | 26.091 | 0.338 | 0.166 | 0.610 | 0.000 |
| Woman’s occupation | |||||||
| Housewife (Ref.) | 2.829 | 0.007 | |||||
| Self-employed | 0.111 | 0.918 | 0.15 | 1.118 | 0.185 | 6.754 | 0.447 |
| Government employee | 0.182 | 0.780 | 0.055 | 1.200 | 0.071 | 0.682 | 0.009 |
| Private employee | 0.980 | 0.129 | 57.713 | 1.255 | 1.102 | 2.208 | 0.002 |
| Spouse’s occupation | |||||||
| Unemployed (Ref.) | 1.788 | 0.0409 | |||||
| Self-employed | -0.735 | 0.570 | 1.663 | 0.480 | 1.267 | 2.354 | 0.001 |
| Government employee | -1.527 | 0.672 | 5.163 | 0.217 | 0.058 | 0.811 | 0.004 |
| Private employee | -0.811 | 0.667 | 1.480 | 0.444 | 1.010 | 1.052 | 0.028 |
| Number of pregnancies | |||||||
| 1 (Ref.) | 19.386 | 0.000 | |||||
| 2 | -0.133 | 0.318 | 0.174 | 0.876 | 0.470 | 1.634 | 0.677 |
| 3 | 0.110 | 0.051 | 4.652 | 1.226 | 1.126 | 1.326 | 0.000 |
| ≥ 4 | 0.248 | 0.412 | 0.363 | 1.282 | 0.009 | 0.921 | 0.042 |
| Age at marriage (y) | 0.524 | 0.115 | 20.762 | 1.307 | 1.082 | 1.532 | 0.001 |
| Mother's age at birth of the first child (y) | -0.191 | 0.042 | 20.681 | 0.425 | 0.343 | 0.507 | 0.033 |
Table 5.
Simultaneous Modeling of Socioeconomic Characteristics and Domestic Violence in Pregnant Women
| Variables | B | SE | Wald | EXP b | 95% CI for EXP b | Sig | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Income/financial ability to afford the costs of living | |||||||
| Totally inadequate (Ref.) | 26.112 | 0.000 | |||||
| Insufficient | 1.510 | 0.490 | 9.517 | 4.528 | 1.735 | 11.822 | 0.002 |
| Somewhat enough (acceptable) | 0.795 | 0.508 | 2.448 | 2.215 | 0.818 | 6.000 | 0.118 |
| Enough | -0.14 | 0.023 | 37.051 | 0.869 | 0.017 | 1.945 | 0.159 |
| Highly adequate | -0.550 | 0.377 | 2.125 | 0.577 | 0.002 | 0.793 | 0.035 |
| Family’s economic class (household income) | |||||||
| Very low (Ref.) | 109.499 | 0.000 | |||||
| Low | -0.094 | 0.02 | 22.090 | 0.912 | 0.271 | 1.116 | 0.098 |
| Medium | -0.941 | 0.843 | 1.247 | 0.390 | 0.060 | 0.455 | 0.001 |
| High | -1.030 | 0.969 | 1.130 | 0.357 | 0.105 | 0.838 | 0.022 |
| Very high | -1.367 | 0.874 | 2.448 | 0.255 | 0.243 | 0.866 | 0.016 |
| Education of parents (father) | -0.248 | 0.035 | 50.207 | 0.785 | 0.716 | 0.854 | 0.015 |
| Parents’ education (mother) | -0.046 | 0.016 | 8.266 | 0.655 | 0.624 | 0.686 | 0.000 |
| Family size | |||||||
| ≤ 2 (Ref.) | 20.449 | 0.000 | |||||
| 3 | 0.121 | 0.867 | 0.019 | 1.128 | 0.206 | 6.168 | 0.889 |
| 4 | 1.451 | 0.321 | 20.449 | 4.268 | 2.276 | 8.006 | 0.000 |
| ≥ 5 | 1.562 | 0.291 | 28.771 | 4.770 | 2.695 | 8.442 | 0.000 |
| Financial concerns | |||||||
| Always (Ref.) | 8.222 | 0.044 | |||||
| Mostly | -0.535 | 0.325 | 2.714 | 0.586 | 0.310 | 1.107 | 0.099 |
| Sometimes | -0.205 | 0.347 | 0.351 | 0.814 | 0.413 | 1.607 | 0.554 |
| Rarely | -0.029 | 0.329 | 0.008 | 0.972 | 0.510 | 1.852 | 0.931 |
| Never | -0.679 | 0.328 | 4.296 | 0.507 | 0.267 | 0.964 | 0.038 |
| Living area, m2 | |||||||
| < 60 (Ref.) | 2.149 | 0.034 | |||||
| 60 - 70 | -0.133 | 0.318 | 0.174 | 0.876 | 0.470 | 1.634 | 0.677 |
| 71 - 80 | -0.383 | 0.612 | 0.392 | 0.682 | 0.205 | 2.263 | 0.531 |
| 81 - 90 | -0.455 | 1.056 | 0.186 | 0.634 | 0.195 | 0.564 | 0.000 |
| ≥ 91 | -1.811 | 1.235 | 2.149 | 0.164 | 10.000 | 15.249 | 0.020 |
In the case of a planned pregnancy, the likelihood of domestic violence was 67% lower in pregnant women (CI: 1.116 - 0.610; OR = 0.338). The analysis of the relationship between women's occupation and domestic violence showed that women working in the private sector were more likely to experience domestic violence during pregnancy compared to housewives (reference group) or self-employed and government employees (CI: 1.102 - 0.208; OR, 1.255). Also, women with working spouses in the government or private sector (respectively) were 79% (CI: 0.058 - 0.811; OR, 0.217) and 55% (CI: 1.010 - 1.052; OR, 0.444) less likely to experience domestic violence compared to the reference group (unemployed men). The OR for the variable of women's age at marriage showed that with an increase of one unit in women's age at marriage, provided that other variables were constant, the probability of domestic violence increased by 1.30 (30%), on average (CI: 1.0182 - 1.532; OR = 1.307). Also, for every unit (year) increase in women's age at the time of the first child’s birth, the probability of domestic violence decreased by 58%, on average (CI: 0.343 - 0.507; OR = 0.425).
Table 5 demonstrates the results of the simultaneous modeling of socioeconomic status and domestic violence using a logistic regression model. The examination of the relationship between the household economic class and domestic violence indicated an inverse association; in other words, with an increase of one unit in the family's economic class, the probability of domestic violence decreased significantly by 74% among pregnant women (CI: 0.046 - 1.413; OR = 0.255). Moreover, analysis of the relationship between the household dimension and domestic violence showed that households with five or more members (reference group size < 5) were more likely to experience domestic violence against women (CI: 0.276 - 8.006; OR = 4.268). Other details of this model are presented in Table 5.
5. Discussion
Violence is a complex multidimensional phenomenon that occurs at both the family and community levels and is rooted in cultural, social, and structural issues (23). This study investigated the relationship between the structural social determinants of health and domestic violence against pregnant women. The prevalence of emotional, physical, and sexual domestic violence against pregnant women referred to selected pregnancy care clinics in Tehran, Iran, were 66.3%, 10.2%, and 9%, respectively.
According to UNESCO (2015), 85% of violence against women is committed by their male partners. The prevalence of domestic violence against younger women (15 - 24 years old) ranges from 29.4% to 31.6%, while the corresponding rate among older women (> 24 years old) ranges from 15.1% to 31.6% (24). Since research on violence during pregnancy currently accounts for 20% of all peer-reviewed nursing research, the prevalence estimates vary. In a systematic review and meta-analysis in 2021, the global prevalence of physical, emotional, and sexual violence was estimated at 9.2%, 18.7%, and 5.5%, respectively. According to recent comprehensive reviews, while some hospital- and clinic-based studies have suggested an increased risk of domestic violence, national and international population-based studies have shown that pregnant women are not at a higher risk of IPV than non-pregnant women; they may even be at lower risk (25). Although the prevalence of IPV in pregnancy varies in different countries, one-quarter of mothers are at risk worldwide, on average (26). Clearly, differences in the type of domestic violence in different studies may be due to differences in the definitions of violence, the mothers' understanding of domestic violence, the tools used, sample sizes, and sociocultural and environmental characteristics of the participants.
Various studies have confirmed the effects of socioeconomic and cultural factors on domestic violence. For instance, age, education, women's employment status, economic class, ethnicity, and place of residence affect a woman’s sense of security toward an intimate partner and influence the risk of domestic violence (27, 28). In the present research, the individual/obstetric factors, including the education and occupation of women and their spouses, ethnicity, women's age at the time of marriage and birth of the first child, type of pregnancy (wanted or unwanted), and the number of pregnancies, had significant associations with domestic violence in pregnant women. In this regard, Bahmani et al., in a meta-analysis of 28 studies, showed that the low education level of the mother, the unemployment of the mother, and the number of children were important factors in the increase of domestic violence during pregnancy (29), which is in line with the findings of the present study.
In developing countries, domestic violence against women is caused by gender inequality, patriarchy, cultural poverty, socialization, and lack of legal and social protection (30). However, the relationship between domestic violence and women's employment status is not clear. The findings of the present study indicated the highest rate of domestic violence in working women compared to housewives or self-employed women. Meanwhile, in a study by Abramsky et al., women with an independent income were exposed to a lower risk of physical IPV in the past year. In this study, a higher income was associated with several potential solutions to reduce IPV, such as improvement of female empowerment, reduction of family conflicts, settlement of arguments over the partner's inability to provide for the family, and improvement of couple communication dynamics (31). The reason for this discrepancy may be variations in the characteristics of the studied samples. Overall, mood changes and needs of pregnant women in the workplace compared to non-pregnant women make them more irritable due to job stress and fatigue. Besides, job and family responsibilities impose an increased burden on these women. Also, women's participation in earning can increase the risk of competition between partners and weaken the man's role as the family's breadwinner; this issue can harm their understanding and empathy and lead to violence against women (32).
The findings of the present study showed a significant relationship between domestic violence and the education level of women and their spouses. Overall, women with academic education (69%) experienced less domestic violence compared to those with elementary education. The findings of a cross-sectional study by Inal et al. in Turkey also showed that women without formal education and those with only elementary education were four and two times more likely to experience physical violence compared to women with higher education levels, respectively. Apparently, as the education level of each parent increases, their awareness and knowledge of coping with conflicts in relationships is also increased. Moreover, increased education of women familiarizes them with their social rights and enhances their skills and socioeconomic status; consequently, the average rate of domestic violence decreases. It is possible that mothers with more children may tolerate and hide violence due to maternal feelings and love for their children, which could result in the repetition of this behavior by their partners (33).
Socioeconomic status is one of the critical determinants of health and mortality. Some believe that the SES index involves a combination of education or training, social class (occupation), and income (34). In the present study, women with working spouses were subjected to domestic violence to a lesser extent than women with unemployed or self-employed spouses (78% and 55%, respectively). Also, for individuals with high or very high-income levels, the likelihood of experiencing domestic violence was 64% and 74% lower than for individuals with very low income, respectively.
Slabbert, in qualitative research on abused low-income women, found that poverty and low family income made them more vulnerable to domestic violence due to limited options and resources, as poverty can act as an inciting factor for this type of conflict (35). Almost 3 out of every 4 women in the Manisa province of Turkey are unemployed and have no independent income. It can be claimed that women have a lower social status than men in terms of education and employment (36). Generally, income is one of the most important structural factors related to domestic violence. The woman’s inadequate income and unemployment can increase marital disputes due to financial problems and cause adverse psychological effects. Meanwhile, occupation, financial independence, and optimal economic status are protective factors against all types of violence (37).
Concerning the relationship between household size and domestic violence, it was found that the probability of domestic violence increases with an increase in household size. Chowdhury et al. showed a significant relationship between the number of family members, marital age, wealth index, and domestic violence in urban slum women of Bangladesh (38). Evidently, the family structure varies around the world. There is a global trend toward continuous changes in family structure, with a shift toward nuclear families. The findings of some studies have shown that a higher number of family members (extended and non-nuclear families) is associated with a high rate of IPV (39). In contrast, the results of some studies have revealed that with an increase in family size, the amount of domestic violence decreases (40). The contradictory findings of these studies require further research to investigate how extended families affect domestic violence by an intimate partner. Given the universality of IPV, it is important to investigate this phenomenon across different relationship and family structures, as well as cultural contexts (41).
In previous studies, differences in the type and number of independent variables are significant in reporting the predictive power of desired outcomes. In the present study, the independent demographic/obstetric and economic/social variables could separately predict more than 50% of changes in the functional variable (domestic violence). Moreover, a quantitative survey by Talebpour showed that in Ardabil province, Iran, eight independent variables explained more than 50% of the variance in the dependent variable of spousal abuse (42). So far, several studies have confirmed the importance of violence against pregnant women (43). Therefore, health-promoting behaviors can be used to maintain and improve maternal health. The behavior and adaptation of pregnant women to different life situations, as well as their impact on maternal and neonatal outcomes, cannot be ignored. Effective measures are necessary for this period, such as physical and mental self-care, healthy behaviors, attention to changes and needs of pregnancy based on socioeconomic and cultural factors, use of stress control methods, having social interactions, and seeking social support (44).
5.1. Strengths and Limitations
Since healthy behaviors during pregnancy have positive effects on maternal and neonatal outcomes, it is necessary to analyze relevant information among pregnant women in different populations. To the best of our knowledge, there is no comprehensive information available on this phenomenon. Accordingly, the present study aimed to accurately identify the risk factors for domestic violence and to determine the relationship between domestic violence and structural determinants of health (demographic/obstetric and economic/social factors), specifically among pregnant women. The most important strengths of this study were the use of a standard domestic violence tool designed by the WHO and the examination of pregnant women’s views in different weeks of pregnancy regarding violent domestic behaviors. Additionally, most mothers benefited from phone and online services during the COVID-19 outbreak.
The present study attempted to determine the relationship between structural factors and domestic violence based on a review of the literature. While there may be some influencing factors that have not been identified yet, such as genetic factors, it can be difficult or even impossible to measure and study them; this may be considered a limitation of the current research. Also, the uncertainty of the participants' responses due to factors such as fear of retaliation or revenge by their partners and reluctance to involve judicial authorities might have affected the accuracy of investigations into the actual frequency of violent behaviors against them. We tried to eliminate these obstacles to a large extent by ensuring mothers the confidentiality of their information. Although the participants were selected from different areas of Tehran, the findings cannot be generalized for reasons such as cultural and ethnic differences in Iran and differences in measurement methods, and cannot be extended to the entire population of the country. Besides, the spouses of these women were unavailable, and it was not possible to investigate them. It is important to note that this study was conducted during the COVID-19 pandemic, and the negative and widespread psychological effects of this disease on individuals and their families, particularly partners, cannot be ignored.
The conclusions of this research and the proposed solutions are based on the obtained results. It is suggested to conduct further studies in other provinces of Iran regarding the relationship between the structural determinants of health and acts of domestic violence during pregnancy and also to evaluate this relationship in men. It is also recommended to conduct a comparative study of the relationship between structural factors affecting violence in pregnant women with or suspected of COVID-19 and non-pregnant women.
5.2. Conclusions
This study indicated the importance of understanding the prominent role of individual/obstetric and economic/social factors as social structural determinants of health in domestic violence. The high prevalence of domestic violence in pregnancy in the target population suggests that domestic violence is a common problem related to the structural social determinants of health. Screening is the first step in solving this problem. Considering the negative consequences of unhealthy behaviors on the mother and fetus, it is necessary to evaluate the risk factors for domestic violence during pregnancy and to specifically identify pregnant women who are at risk of violence or those who have experienced it.