1. Background
Threatened abortion (TA) is identified when an individual experiences vaginal bleeding, with or without accompanying abdominal pain during pregnancy under 20 weeks (1). The clinical diagnosis is based on spotting or vaginal bleeding with a closed cervix in the first trimester of pregnancy (2). It could be a common complication of pregnancy, occurring in approximately 20% of pregnant women. Nearly half of these cases result in a complete abortion (3). In a study, the number of all types of abortions in 2021 worldwide was estimated at 23 million (4), and TA affects about 7 to 24 percent of the population (5). Factors involved with TA include changing lifestyles and eating habits, increasing severe environmental pollution, increasing job and work stress among women and elderly pregnant women, and reducing the quality of oocytes (6). Evidence indicates that approximately 17% of women with TA encounter various complications in the later stages of pregnancy (7). other various factors contribute to TA, including chromosomal abnormalities, gynecologic disorders, unhealthy lifestyle choices, and occupational stress (8).
Bleeding associated with TA can induce maternal anxiety, thereby elevating the risk of adverse fetal/maternal outcomes (9). Various studies have associated TA with an elevated risk of complications, such as preterm delivery, placenta previa, hypertension/preeclampsia, fetal growth restriction, and the need for neonatal intensive care unit (NICU) support (10, 11). Abortion is also a distressing experience that can affect a woman's emotional state and potentially lead to psychological disorders, such as depression (12). In a study carried out by Zhu et al., it was found that the incidence of major depression and anxiety symptoms was significantly higher in women experiencing TA compared to those with a stable pregnancy (13). In another study in Singapore, they reported that depression and anxiety were higher in women who were at risk of abortion, and TA may be a risk factor for antenatal depression (14). Steinberg et al. study on psychosocial and pre-abortion factors and mental health that the importance of stigma. Perceived abortion stigma appeared to explain the most additional variance in depression, anxiety, and stress symptoms. The relationship between the stigma of abortion and symptoms of depression, anxiety, and stress before abortion was strong and highly significant (15).
Psychotherapy can indeed serve as an effective intervention in managing the traumatic experience associated with TA. Evidently, providing psychological support is crucial for women undergoing this ordeal (16, 17). While numerous studies highlight the impact of psychotherapy on enhancing the mental well-being of women post-abortion (18, 19) there are limited reports on its impact on patients facing TA. A qualitative study conducted in South Africa on pregnant women at risk of abortion revealed that counseling, raising awareness among these women, timely psychotherapy, and early diagnosis can contribute to improved childbirth outcomes (20). A study that examined the effectiveness of a happiness counseling program on depression, anxiety, and stress in pregnant women with a history of abortion showed that this non-pharmacological intervention improves the cognitive and emotional state of the patients and allows them to have a more positive attitude towards their abortion (21).
In recent decades, internet-based treatments have been employed to address a range of psychiatric disorders during pregnancy and the postpartum period, including depression and anxiety (22), as well as psychological issues arising postpartum (23). Numerous articles have confirmed the accessibility, feasibility, and acceptability of internet-based treatments for managing various disorders, even during pregnancy (24, 25). The advantages of internet-based cognitive behavioral therapy (iCBT) include easy and round-the-clock access to treatment, evasion of the stigma associated with in-person therapist meetings (26), preservation of privacy (27), increased adherence to therapeutic tasks (28), cost-effectiveness, elimination of geographical limitations (29), and patient anonymity (30). In Kheirkhah et al.'s study, it was found that ICBT is feasible and available for providing treatment to infertile patients. Also, this study confirmed that both ICBT and face-to-face CBT are equally effective in reducing patients' depression and anxiety (25).
The unified protocol (UP) is a transdiagnostic CBT approach that targets common psychopathological trauma related to emotional disorders and has a special emphasis on emotion regulation (31). The objective of integrated transdiagnostic treatment is to impart new adaptive strategies for emotion regulation, enabling patients to better tolerate intense emotions and enhance their quality of life, irrespective of their definitive diagnosis (32).
Despite the high prevalence of mental disorders, such as depression and anxiety, in women facing TA and the reported effectiveness of iCBT and internet-based UP (iUP) psychotherapies in various populations, the efficacy of these two models has not been compared in pregnant women. To the leading of our knowledge, this is the primary study to evaluate the feasibility and acceptability of iCBT-Specific and iUP psychotherapies in women with TA, encountering depression and anxiety disorders.
2. Objectives
Our objectives were threefold: (1) to assess the acceptability and feasibility and evaluate the effectiveness of iCBT-Specific and iUP psychotherapies in women with TA, experiencing depression or anxiety disorders; (2) To compare the effectiveness of iCBT-Specific and iUP psychotherapies in improving depression and anxiety symptoms in women with TA.
3. Methods
This study was conducted in two stages. In the initial phase, we developed two treatment programs, including a transdiagnostic program and a specific iCBT program, for women with TA diagnosed with anxiety and depression. In the subsequent phase, we evaluated the effectiveness of these programs through a semi-experimental study.
3.1. Phase 1: Design of the Treatment Plan
The content of both iCBT-Specific treatment and iUP programs received approval from the Department of Psychiatry and Psychology at Babol University of Medical Sciences, Iran. Also, both programs were uploaded to a website (www.peacefulmindme.com).
3.1.1. iCBT-Specific Treatment
The standard iCBT-Specific treatment for depression and anxiety was grounded in the methodologies proposed by Beck and Beck (33) and Wright et al. (34), with a particular emphasis on psych education related to TA (including signs of TA and ways to control it, teaching the thought cycle and defining thought-feeling and behavior and rumination, identifying common cognitive distortions and their impact on the pregnancy process and the challenges ahead- Behavioral activation and coping behavior training and self-care).
The specific computer-based therapy was structured into eight sessions, each lasting 50 minutes. Each session was composed of multiple steps, which included videos featuring a mental health specialist. This specialist guided the patient and discussed various self-help strategies. Additionally, videos featuring a fictional character grappling with anxiety and depression were developed. These videos were designed to help patients recognize their issues, work towards improving their condition, and understand that they are not alone in their struggle. The therapy sessions incorporated photos, texts, and educational PowerPoint presentations as tools to enhance understanding. During the sessions, we engaged the patients by asking questions about the content, aiming to focus their attention on it. Through exercises and assignments, the patients were encouraged to apply these strategies to their own problems. The treatment was guided weekly for 20 minutes over the phone by the first author.
3.1.2. Unified Protocol
The transdiagnostic treatment comprised of eight sessions, each lasting 50 minutes. This approach was adopted from the treatment protocol outlined by Barlow and colleagues, as presented in a book titled “Integrated Protocol for Transdiagnostic Treatment of Emotional Disorders (Therapist’s Guide)” (35). Generally, the UP for the transdiagnostic treatment of emotional disorders is an intervention rooted in emotion-focused CBT. It is structured into five modules or “core” components, each of which is grounded in the elements of CBT with proven efficacy. These components are specifically designed to address negative emotions and adverse reactions to these emotions (36). The structure of the meetings is presented in Appendix 1. (skill of observing emotional experiences- Fostering awareness to recognize thought patterns- articulating the reciprocal relationship between cognition and emotion - execution of physical confrontation exercises appropriate for expectant mothers,…). The treatment was administered by the first author, who provided guidance over the phone for a duration of 20 minutes each week.
3.2. Phase 2: Conducting a Pilot Study to Determine the Effectiveness of Treatments
We carried out a semi-experimental investigation at Rohani Hospital (an inpatient hospital) and at two private outpatient obstetrics and gynecology clinics in Babol, a city in northern Iran. The study spanned from April to October 2023, encompassing 80 eligible participants, all of whom were diagnosed with depression and anxiety disorders and were included in the iCBT-Specific and transdiagnostic online UP programs.
3.3. Participants
Pregnant patients, both inpatient and outpatient, were chosen from a public hospital and two private obstetrics and gynecology clinics in Babol. The inclusion criteria were being over 18 years of age, having a gestational age of 5 - 12 weeks, and a diagnosis of anxiety disorders and depression based on the Mini-International Neuropsychiatric Interview (MINI) (37). Other inclusion criteria were access to a computer and the internet and an education level above elementary school. The exclusion criteria were severe mental disorders (e.g., bipolar disorders and schizophrenia), risk of suicide at the time of evaluation, drug use in the last three months, and experiencing psychotherapy or taking drug for the treatment of anxiety/depression in the last six months. Patients with serious mental disorders were referred to the specialized psychiatric clinics of the hospital for appropriate treatment.
G*Power software was used to determine the sample size taking into account the findings of a study by Shafierizi et al. (38). With an effect size of 0.14, an error level assumption of 0.05, and a power of 80%, the minimum required sample size for each group was estimated to be 40 individuals. Factoring in a 10% attrition rate, a total of 88 individuals were included in the study.
In total, the psychologist interviewed 192 pregnant women at risk of abortion. Out of these women, 104 did not meet the inclusion criteria (94 did not have disorders, six had severe psychiatric disorders, and four were receiving treatment at other medical centers). Consequently, 88 women were admitted into the treatment process. However, four participants from each group were later excluded from the analysis due to discontinuation of the sessions and failure to complete the post-test.
Following the interview, eligible women filled out the informed consent form. Participants from both groups then completed the Brief Symptom Inventory-18 (BSI-18) prior to the commencement of treatment, allowing for the assessment of depression and anxiety symptoms. After completing an eight-week course of 50-minute internet-based treatment sessions, the participants filled out the BSI-18 again, along with the Client Satisfaction Questionnaire (CSQ-8) and the System Usability Scale (SUS).
3.4. Measures
We used the Mini-International Neuropsychiatric Interview (MINI) to select patient TA with depression and anxiety disorder to participate in the study. The three instruments including, BSI-18, SUS, and CSQ-8 was used to assess the outcomes.
3.4.1. The Mini-International Neuropsychiatric Interview
It is a brief structured psychiatric interview designed as a diagnostic tool to identify psychiatric disorders according to DSM-5. Mini-international neuropsychiatric interview (M.I.N.I) can be done in less than 15 minutes. and has similar reliability and validity to similar longer instruments. Clinicians/researchers intending to use the M.I.N.I undergo special training before using the tool to ensure that the quality standard is maintained (37). According to NejatiSafa et al.'s study, the Persian version of M.I.N.I is an applicable, reliable, and valid tool for diagnosing some mental disorders. Test-retest reliability was very good (phi = 2, Cramer's V = 0.89, P < 0.0001) (39).
3.4.2. Brief Symptom Inventory
The shortened form of BSI-53 contains 18 items from BSI-53. This test includes three subscales: Somatization, depression, and anxiety. Its total score is (maximum = 72). Higher scores indicate more severe psychiatric symptoms. The scoring of questions is based on a five-point Likert Scale (0 = not at all, 1 = slightly, 2 = moderately, 3 = slightly, 4 = severely). The BSI-18ʹs psychometric properties have been utilized in numerous countries and languages (40). The Persian version of BSI-18 exhibits good validity and reliability. The test-retest reliability of Persian BSI-18 was reported as 0.81 (41).
3.4.3. Client Satisfaction Questionnaire
The CSQ-8 was developed by Lasern et al. (42). Client Satisfaction Questionnaire is the short form of a 31-item instrument that measures general satisfaction. This tool includes 8 Likert-type items with scores from 1 to 4 (1 indicates the lowest degree of satisfaction and 4 the highest).
3.4.4. System Usability Scale
The SUS, developed by Brooke, is a simple self-report scale to assess perceived ease of use (43). It consists of 10 items with a 5-point Likert Scale, from strongly agree to strongly disagree. To calculate the SUS score, the score of odd-numbered –is subtracted by 1, and the score of even-numbered -is calculated by subtracting the score from 5. By multiplying the total scores by 2.5, the overall is obtained. The total score can range from 0 (very poor usability) to 100 (excellent usability). We used the validated Persian SUS (44). The computed Cronbach’s alpha for the Persian version of SUS was 0.79.
3.5. Statistical Analysis
SPSS software (SPSS 21, SPSS Inc., Chicago, IL, USA) was used for data analysis. Descriptive statistics were also used to check the frequency distribution and mean and standard errors of the mean. A paired t-test was also used within a group of psychotherapies. Analysis of covariance (ANCOVA) was used to compare changes in the outcomes in two groups of specific iCBTs versus iUP participation. T-tests were used to compare the satisfaction and feasibility of the treatment between iCBTs and iUP. A P-value < 0.05 was considered to be statistically significant.
4. Results
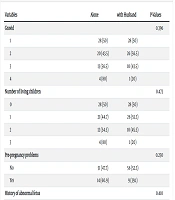
The demographic characteristics of the studied population are shown in Table 1. There was no significant difference between the iCBT-Specific and transdiagnostic iUP groups in terms of age (32.22 ± 6.28 vs. 30.47 ± 5.77 P = 0.199) and other demographic variables. The average age of the participants in this study is 31.35 ± 6.06 years old. Approximately 64% of the participants had an education level below a high school diploma, while 36% had a university education. The number of pregnancies did not significantly differ between the two groups (P = 0.357). The average gestational age was eight weeks, and there was no significant difference between (8.30 ± 1.97 vs. 9.02 ± 2.32 P = 0.137).
Table 1.Characteristics of the Study Population a
| Variables | Specific-iCBTs | iUnified Protocol | Overall (n = 80) | P-Value |
|---|---|---|---|---|
| Age | 32.22 ± 6.28 | 30.47 ± 5.77 | 31.35 ± 6.06 | 0.199 |
| Education | 0.329 | |||
| Primary school | 28 (70) | 23 (57.5) | 51 (63.75) | |
| ≥ High School | 12 (30) | 17 (42.5) | 29 (36.25) | |
| Gravid | 0.357 | |||
| 1 | 13 (32.5) | 17 (42.5) | 30 (37.4) | |
| 2 | 15 (37.5) | 12 (30) | 27 (33.8) | |
| ≥ 3 | 12 (29) | 11 (27.5) | 23 (28.8) | |
| Gestational age weeks | 8.30 ± 1.97 | 9.02 ± 2.32 | 8.66 ± 2.17 | 0.137 |
Abbreviations: Specific-iCBTs: cognitive behavioral therapy; iUP, unified protocol.
a Values are expressed as mean ± SD or No. (%).
Table 2 provides a comparison of the acceptability and feasibility of the two treatment methods. The data indicated that both the iUP and iCBT-Specific models had high average acceptability scores (25.25 and 25.35 out of a total score of 32, respectively). Furthermore, the average feasibility of treatment was above average for both models (58.93 and 53.56 out of a total score of 100, respectively). The results of the t-test showed that there is no significant difference between the two treatment models in terms of acceptability and feasibility (P > 0.05).
Table 2.Acceptability and Feasibility of the iUnified Protocol vs Specific-iCBTs a
| Acceptability | Specific-iCBTs Mean (SD) | iUnified Protocol | P-Value |
|---|---|---|---|
| 1. Quality of service | 3.07 (0.26) | 3 (00) | 0.083 |
| 2. Kind of service wanted | 3 (0.32) | 3 (00) | 1 |
| 3. Needs met | 3.07 (0.34) | 3.12 (0.33) | 0.516 |
| 4. Would recommend to friend | 3.07 (0.26) | 3 (00) | 0.083 |
| 5. Satisfaction with help received | 3.25 (0.43) | 3.15 (0.36) | 0.269 |
| 6. Dealt with problems | 3.42 (0.50) | 3.52 (0.50) | 0.377 |
| 7. Overall satisfaction | 3.20 (0.40) | 3.22 (0.42) | 0.788 |
| 8. Would return to program | 3.25 (0.43) | 3.22 (0.42) | 0.796 |
| Total score (range 8 - 32) | 25.35 (1.91) | 25.25 (1.17) | 0.779 |
| Feasibility | 0.063 | ||
| Total score (range 1 - 100) | 53.56 (11.69) | 58.93 (13.72) |
Abbreviations: Specific-iCBTs, cognitive behavioral therapy; iUP, unified protocol.
a Range of scores: Acceptability, 1 - 4, total 8 - 32; feasibility 1 - 100%.
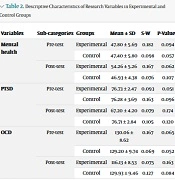
Table 3 provides a comparison of intra- and inter-group treatment outcomes for the two treatment methods. The results of the paired t-test and ANCOVA revealed that the iUP treatment significantly reduced depression (95% CI: 2.42 to 5.32) by 3.87, with an effect size of 0.370. It also reduced anxiety (95% CI: 3.32 to 5.47) by 4.40, with an effect size of 0.536, thereby significantly reducing TA in women. Similarly, the iCBT-Specific treatment significantly reduced depression by 2.42 (95% CI: 1.22 to 3.62) with an effect size of 0.370 and anxiety (95% CI: 1.91 to 4.28) by 3.10 with an effect size of 0.536 in women with TA.
In terms of the somatization sub-component, the iUP treatment was able to reduce somatization symptoms by 1.87 (95% CI: 0.83 to 2.91), while the iCBT-Specific treatment reduced them by 3.07 (95% CI: 1.96 to 4.18). As for the sum of sub-components, or total BSI, the iUP treatment significantly reduced psychological distress in women with TA by 8.39 (95% CI: 7.46 to 12.83), and the iCBT-Specific treatment reduced it by 8.60 (95% CI: 5.76 to 11.43). The ANCOVA comparison of the two treatment groups revealed no significant difference in the effectiveness of iUP and iCBT-Specific treatments in terms of improving depression (P = 0.146) or anxiety (P = 0.221).
Table 3.Comparison of the Effectiveness of Unified Protocol vs. Specific-iCBTs on the Improvement of Depressive and Anxiety Symptoms in Women with Threatened Abortion
| Measure Group | Intervention, Mean (SD) | Pre-post Test | Within-Group Mean Diff (CI95%) | Eta Effect Size for Time | Between-Group P-Value | Between-Group Eta Effect Size |
|---|---|---|---|---|---|---|
| Depression | 0.370 | 0.146 | 0.027 | |||
| iUnified protoco | 6.45 (5.35) | 2.57 (2.92) | 3.87 (2.42-5.32) | |||
| Specific iCBTs | 5.52 (4.32) | 3.10 (2.77) | 2.42 (1.22-3.62) | |||
| Anxiety | 0.536 | 0.221 | 0.019 | |||
| iUnified protocol | 7.85 (4.17) | 3.45 (3.28) | 4.40 (3.32-5.47) | |||
| Specific iCBTs | 6.87 (3.99) | 3.77 (3.22) | 3.10 (1.91-4.28) | |||
| Somatization | 0.357 | 0.254 | 0.017 | |||
| iUnified protocol | 5.05 (3.35) | 3.17 (2.38) | 1.87 (0.83-2.91) | |||
| Specific iCBTs | 5.90 (3.56) | 2.82 (2.43) | 3.07 (1.96-4.18) | |||
| Total BSI | 0.548 | 0.874 | 0.0003 | |||
| iUnified protocol | 19.35 (10.81) | 9.20 (7.38) | 8.39 (7.46-12.83) | |||
| Specific iCBTs | 18.30 (9.39) | 9.70 (7.26) | 8.60 (5.76-11.43) |
Abbreviations: Specific-iCBTs, cognitive behavioral therapy; iUP, unified protocol.
5. Discussion
This study investigated the effectiveness, acceptability, and feasibility of two treatments, including a transdiagnostic and a diagnosis-specific method, aimed at alleviating depression and anxiety in women with TA. Both the iUP and iCBT-Specific models demonstrated high acceptability. Furthermore, the feasibility of both treatment models was found to be above average. However, when comparing the two models in terms of acceptability and feasibility among women with TA, neither model proved to be superior.
Given the lack of studies comparing the acceptability and feasibility of iUP and iCBT-Specific treatments, reference has been made to a study that reported on one of these treatments. In the research conducted by Shariatpanahi et al., emotional iCBT was utilized to treat anxiety in pregnant women and their spouses. The results of this study echoed our findings, indicating the high acceptability and feasibility of this treatment among both pregnant women and their spouses (mean CSQ-8 = 24.2, SD = 4.9) (P = 0.008) (24). Additionally, our findings align with those of another study implementing iCBT. This study also reported mean CSQ-8 scores of 25.06 with a standard deviation (SD) of 4.18 (25). Conversely, a different study investigating the use of online CBT for treating coronary artery disease reported a lower level of treatment acceptance compared to our study (45).
Quantitative and qualitative data from another study suggest that Web-based therapy is generally useful, although it has important advantages and disadvantages. In web-based treatments, participants enjoyed access, anonymity, and weekly reminders, as well as an introduction to the principles of CBT and mindfulness. However, this treatment was not sufficiently user-friendly, long-lasting, and compatible with smartphones. Parts of the content were not always relevant or appropriate. Participants felt that it could be improved by having it in the form of a smartphone app and by making the content more concise and including different parenting styles (46).
In our study, the average feasibility scores were 53.56 (SD = 11.69) for the iCBT-Specific group and 58.93 (SD = 13.72) for the transdiagnostic iUP group. These scores are lower than those reported in another study, which had an average feasibility score of 67.07 (SD = 17.23) (25). It appears that in our study, due to the threat of abortion, the participants prioritized concerns related to their physical health and pregnancy over their mental distress. However, given the unique circumstances of these pregnancies (i.e., TA) and the necessity for complete rest, it seems that such online treatments could offer greater benefits for the patients. To substantiate this point, we can cite the study by Hantsoo et al., examining pregnant women, non-pregnant women, and men. Their results indicated that approximately one-third of the pregnant women selected some form of computer-based therapy as their preferred choice (47).
Several assumptions have been made to account for the high treatment satisfaction observed in our study. Firstly, the treatments provided in this study were delivered online with the support of a therapist. Prior research has demonstrated that internet-based treatments with therapist support tend to yield higher satisfaction levels compared to those without therapist support (48). Secondly, the task-oriented nature of the treatments in this study likely contributes to their high acceptability and effectiveness. There is substantial evidence suggesting that homework assignments are crucial to the success of CBT across a range of psychiatric conditions. Specifically, in the context of depression treatment with CBT, the adaptation of homework has been linked to significant clinical improvements and has been shown to predict a reduction in depressive symptoms (49).
Another observation from this study was that both iUP and iCBT-Specific programs were effective in reducing depression and anxiety in women facing TA, with effect sizes of 0.027 and 0.019, respectively. Furthermore, neither iUP nor iCBT-Specific treatment demonstrated superiority over the other in terms of alleviating depression and anxiety symptoms. A study conducted in Iran by Khairkhah et al., which focused on infertile women and was published on the PeacefulMind website, found that iCBT was not less effective than traditional face-to-face CBT in terms of enhancing all outcome variables (25). Numerous systematic reviews and meta-analyses have drawn comparisons between the effectiveness of traditional face-to-face CBT and online CBT (both therapist-guided and self-guided) programs. They found that all three modalities demonstrated comparable effectiveness (27, 50).
Another study was conducted to investigate whether a UP remains equivalent to single disorder protocols (SDPs) in the treatment of anxiety disorders at 12-month follow-up. The results showed that the conditions of UP and SDP remained the same according to the degree of severity of the doctor's initial diagnosis in the 12-month follow-up. Furthermore, there were no significant differences between conditions in secondary outcomes at 12-month follow-up. The effect estimates of UP versus SDPs from baseline to 12-month follow-up was 0.13 (95% CI, -0.37 to 0.62) (51).
Additionally, a study conducted in Iran in 2022, titled “The Effectiveness of Online Integrated Transdiagnostic Treatment on Psychological Distress, Mindfulness, Hyper-Excitement, and Mental Capacity of Pregnant Women”, found that the online integrated transdiagnostic treatment was effective in reducing psychological distress and negative meta-emotion. It also helped promote positive meta-emotion and psychological empowerment among the subjects. However, it did not have a significant impact on mindfulness (52).
While all of the aforementioned studies, including our own, used different measures of anxiety and depression, it is important to note that there is no clear correlation between the number of treatment sessions, the interval between sessions, and the change in symptom scores. A meta-analysis examining the dose-response relationship in standard psychotherapy revealed that patients with less severe symptoms tended to respond to treatment more rapidly (53).
This study has certain limitations. Being a semi-experimental study, it necessitates further randomized controlled trials to validate the effectiveness and feasibility of online treatments. The limited sample size and absence of follow-up studies also constrain the scope of our findings. Also, the therapist’s involvement in this study could have potentially influenced the results, suggesting the need for future studies to explore the efficacy of internet-only treatments without therapist support.
This study suggests potential applications. It indicated the possibility of substituting traditional psychological treatments with transdiagnostic treatments beyond diagnosis, thereby addressing a broad spectrum of mental disorders with high comorbidity rates. Furthermore, it underscores the advantages of online treatments, particularly for high-risk pregnant women.
5.1. Conclusions
The findings of our research suggest that online transdiagnostic treatment is comparably effective to specific diagnostic treatments, with satisfactory acceptability and accessibility. Given the significant benefits of UP treatment, our results support the use of iUP by psychiatrists and gynecologists as a reliable alternative to iCBT-Specific psychotherapies. This could potentially enhance the treatment of depression and anxiety in women at risk of miscarriage.