Introduction
Experimental
Results
Discussion

H&E staining of a wound area (E: epiderm, D: derm, B: the basal layer of the epidermis, C: collagen, F: fibroblast, N: neutrophils, and V: vessels) (40X)

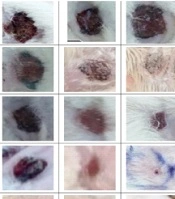
H&E staining of a wound area on days 3. A: Control, B: Control of diabetes, C: nanofiber-Chitosan/Polyvinyl alcohol, D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, and E: film-Chitosan/Polyvinyl alcohol, and F: film-Chitosan/Polyvinyl alcohol/Doxycycline (4X).

H&E staining of a wound area on days 7. A: Control, B: Control of diabetes, C: nanofiber-Chitosan/Polyvinyl alcohol, D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, and E: film-Chitosan/Polyvinyl alcohol, and F: film-Chitosan/Polyvinyl alcohol/Doxycycline (4X)

H&E staining of a wound area on days 14. A: Control, B: Control of diabetes, C: nanofiber-Chitosan/Polyvinyl alcohol, D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, and E: film-Chitosan/Polyvinyl alcohol, and F: film-Chitosan/Polyvinyl alcohol/Doxycycline (4X)

The bar chart Analysis. (A) Percentage reduction of the wound surface, (B) Volume of the epidermis, (C) Volume of dermis and (D) Volume of collagen from the studied groups on days 3, 7 and 14. C: Control, CD: Control of diabetes, n-C/P: nanofiber-Chitosan/Polyvinyl alcohol, n-C/P/D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, f-C/P: film-Chitosan/Polyvinyl alcohol, and f-C/P/D: film-Chitosan/Polyvinyl alcohol/Doxycycline. Significance only showed between dressing and CD groups (*: P < 0.05), (**: P < 0.01), (***: P < 0.001), and (****: P < 0.0001)

The bar chart Analysis. (A) Number of neutrophils,(B) Number of fibroblasts, (C) Number of the basal layer of the epidermis, and (D) Length of vessels from the studied groups on days 3, 7 and 14. C: Control, CD: Control of diabetes, n-C/P: nanofiber-Chitosan/Polyvinyl alcohol, n-C/P/D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, f-C/P: film-Chitosan/Polyvinyl alcohol, and f-C/P/D: film-Chitosan/Polyvinyl alcohol/Doxycycline. Significance only showed between dressing and CD groups (*: P < 0.05), (**: P < 0.01), (***: P < 0.001), and (****: P < 0.0001)

The bar chart Analysis (ELISA). A: IL-1 β, B: TNF-α, C: IL-10 from the studied groups on days 3, 7 and 14. C: Control, CD: Control of diabetes, n-C/P: nanofiber-Chitosan/Polyvinyl alcohol, n-C/P/D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, f-C/P: film-Chitosan/Polyvinyl alcohol, and f-C/P/D: film-Chitosan/Polyvinyl alcohol/Doxycycline. Significance only showed between dressing and CD groups (*: P < 0.05), (**: P < 0.01), and (***: P < 0.001)

The bar chart Analysis (ELISA). A: TIMP-1 and B: MMP-2 from the studied groups on days 3, 7 and 14. C: Control, CD: Control of diabetes, n-C/P: nanofiber-Chitosan/Polyvinyl alcohol, n-C/P/D: nanofiber-Chitosan/Polyvinyl alcohol/Doxycycline, f-C/P: film-Chitosan/Polyvinyl alcohol, and f-C/P/D: film-Chitosan/Polyvinyl alcohol/Doxycycline. Significance only showed between dressing and CD groups (*: P < 0.05)