
Introduction
Experimental
Results
Discussion
| Study | Study design | Number of participants | Population | Intervention | Follow up | Thrombolytic administration | finding |
|---|---|---|---|---|---|---|---|
| Kiser TH et al., 2018 | cohort | 3768 | PTEa without mention of risk category | Compare 50 mg RTPAb versus full-dose 100 mg | No mention | No mention | Same efficacy, hospital mortality and major bleeding; however, patients receiving half-dose of RTPA were more likely to need further escalation in care for the management of their acute PTE. |
| Yilmazel UE et al., 2018 | cohort | 117 | Massive and Submassive c | Compare 50 mg of RTPA versus full-dose (100 mg) | 3 months | 50 mg administrated within 2 hours, 100 mg infused as intravenous bolus of 10 mg, followed by 90 mg within 2 h | Same benefit, hospital mortality and major bleeding. |
| Sharifi M et al., 2013 | RCT d | 121 | Moderate e PTE | Compare reduced dose of RTPA versus anticoagulant alone (enoxaparin) | 28 months | Bolus of 10 mg within 1 minute followed by 40 mg infused over 2 h. | Reduced dose of RTPA showed efficacy in care of patients with PE with a considerable decline in the pulmonary artery pressure that occurred within follow up of 28 months. |
| Mi YH et al., 2013 | cohort | 136 | Submissive pulmonary embolismf | Compare reduced dose of RTPA versus anticoagulant alone (heparin or enoxaparin) | 12 months | 50 mg RTPA administrated over 2 h | Short- and long-term an outcome was more improved in RTPA reduced dose compared with enoxaparin without increasing major bleeding events. |
| Wang C et al., 2010 | RCT | 118 | Hemodynamic instability, Massive PTE g | Compare reduced dose of rt-PA, 50 mg versus full-dose 100 mg | 14 days | 50 mg and 100 mg of RTPA administrated within 2 h | The dose of 50 mg showed similar efficacy, lower total bleedings, and mortality in compare with the dose of 100 mg. |
| Berghaus TM et al., 2010 | cohort | 202 | Intermediate hPTE | Compare 100 mg of RTPA versus anticoagulant alone | 100 mg of RTPA administrated within 2 h | More minor bleedings, same major bleeding and efficacy with shorter hospital stay was seen with RTPA | |
| Konstantinides S et al., 2002 | RCT | 256 | Intermediate PTE | Compare 100 mg of RTPA versus anticoagulant alone (heparin) | 30 days | 100 mg of RTPA administrated within 2 h | Both groups showed very low rate of death and bleedings. Clinical course improvement was seen with RTPA. |
| Goldhaber SZ et al., 1994 | RCT | 90 | Hemodynamically stable | Compare reduced dose of 50 mg versus 100 mg of RTPA | 14 days | 50 mg was given over 15 min and 100 mg of rt-PA administrated within 2 h | Similar efficacy, bleedings and mortality were seen in both groups. A high number of adverse events happened. |
| Sors H et al., 1994 | RCT | 53 | Massive PTE (Hemodynamically unstable) | Compare reduced bolus dose of RTPA, versus 100 mg of RTPA | - | 50 mg infused over 15 min and 100 mg RTPA infused within 2 h | The reduced bolus dose of RTPA showed similar efficacy versus 100 mg RTPA. |
| Goldhaber SZ et al., 1993 | RCT | 101 | Hemodynamically stable | Compare 100 mg of RTPA versus anticoagulant alone (heparin) | 14 days | 100 mg of RTPA infused within 2 h | The RTPA group showed lower rate of mortality and recurrent PE and medical embolectomy |
| Dalla Volta S et al., 1992 | RCT | 20 | Hemodynamically stable i | Compare 100 mg of RTPA versus anticoagulant alone (heparin) | - | 100 mg infused as bolus of 10 mg, followed by 90 mg over 2 h | The RTPA group showed high bleeding rate and faster and greater improvement in angiographic and hemodynamic parameters. |
| PIOPED Investigator, 1990 | RCT | 13 | Hemodynamically stable | Compare 40 to 80 mg of RTPA versus anticoagulant alone (heparin) | 7 days | The RTPA was infused at a rate of 1 mg/min. | The RTPA group showed a high bleeding rate and greater improvement in hemodynamic parameters but not in angiographic variables. |
| Levine M et al., 1990 | RCT | 58 | Hemodynamically stable | Compare a dose of 0.6 mg/kg RTPA versus anticoagulant alone (heparin) | 10 days | RTPA administrated as a 2-minute infusion of | The RTPA group showed greater improvement in perfusion defect with high rate of minor bleeding. |
| RCTs | Cohorts | |||
|---|---|---|---|---|
| n | Pooled RR (CI95%) | n | Pooled RR (CI95%) | |
| Total Bleeding | ||||
| Alteplase standard vs. low dose | 3 | 1.91 (1.16 – 3.15) | 2 | 0.96 (0.51 – 1.81) |
| Alteplase standard dose vs. heparin | 3 | 1.11 (0.31 – 3.99) | 1 | 21 (1.22 – 362.73)* |
| Alteplase low dose vs. heparin | 2 | 5.69 (0.83–39.27) | 1 | 3.61 (0.43 – 30.05)* |
| Major Bleeding | ||||
| Alteplase standard vs. low dose | 3 | 1.92 (0.66 – 5.59) | 2 | 1.04 (0.49 – 2.19) |
| Alteplase standard dose vs. heparin | 3 | 0.60 (0.19 – 1.87) | 1 | 7 (0.34 – 143.95)* |
| Alteplase low dose vs. heparin | 1 | 1.50 (0.07–30.59)* | 0 | - |
| Minor Bleeding | ||||
| Alteplase standard vs. low dose | 3 | 1.91 (0.68 – 5.34) | 1 | 0.72 (0.22 – 2.29)* |
| Alteplase standard dose vs. heparin | 3 | 0.50 (0.17 – 1.49) | 1 | 15.40 (0.86–274.79)* |
| Alteplase low dose vs. heparin | 1 | 1.50 (0.07–30.59)* | 1 | 3.61 (0.43–30.05)* |
| Recurrence of PTE | ||||
| Alteplase standard vs. low dose | 2 | 2.25 (0.51 -9.98) | 1 | 4.10 (0.55 – 30.77)* |
| Alteplase standard dose vs. heparin | 1 | 1.17 (0.30 – 4.57)* | 1 | 1.44 (0.13 – 15.53)* |
| Alteplase low dose vs. heparin | 2 | 0.44 (0.08 – 2.52) | 0 | - |
| Mortality | ||||
| Alteplase standard vs. low dose | 2 | 1.13 (0.30 – 4.29) | 2 | 1.15 (0.87 – 1.53) |
| Alteplase standard dose vs. heparin | 3 | 1.08 (0.37 – 3.18) | 1 | 0.13 (0.02 – 0.97)* |
| Alteplase low dose vs. heparin | 3 | 0.45 (0.13 – 1.63) | 0 | - |
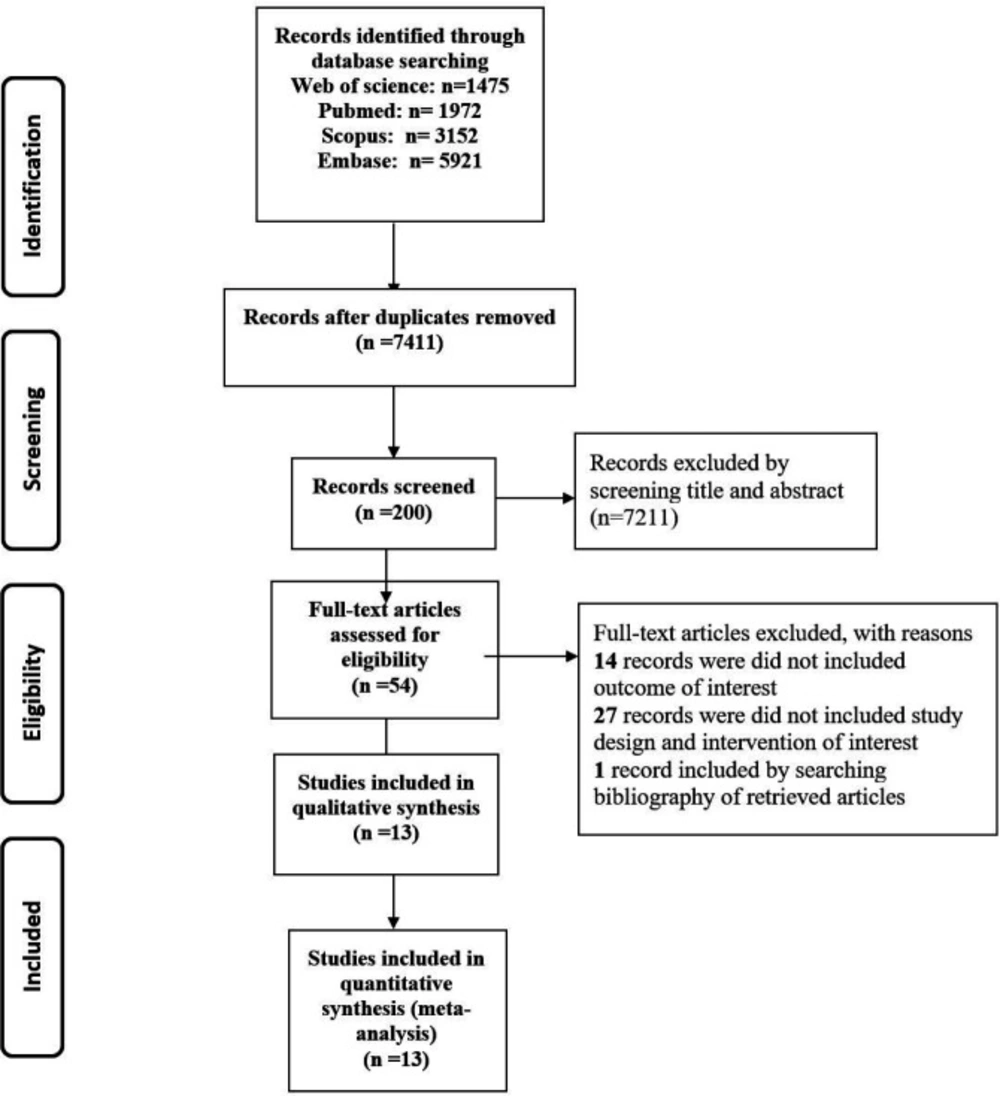
Study flow diagram
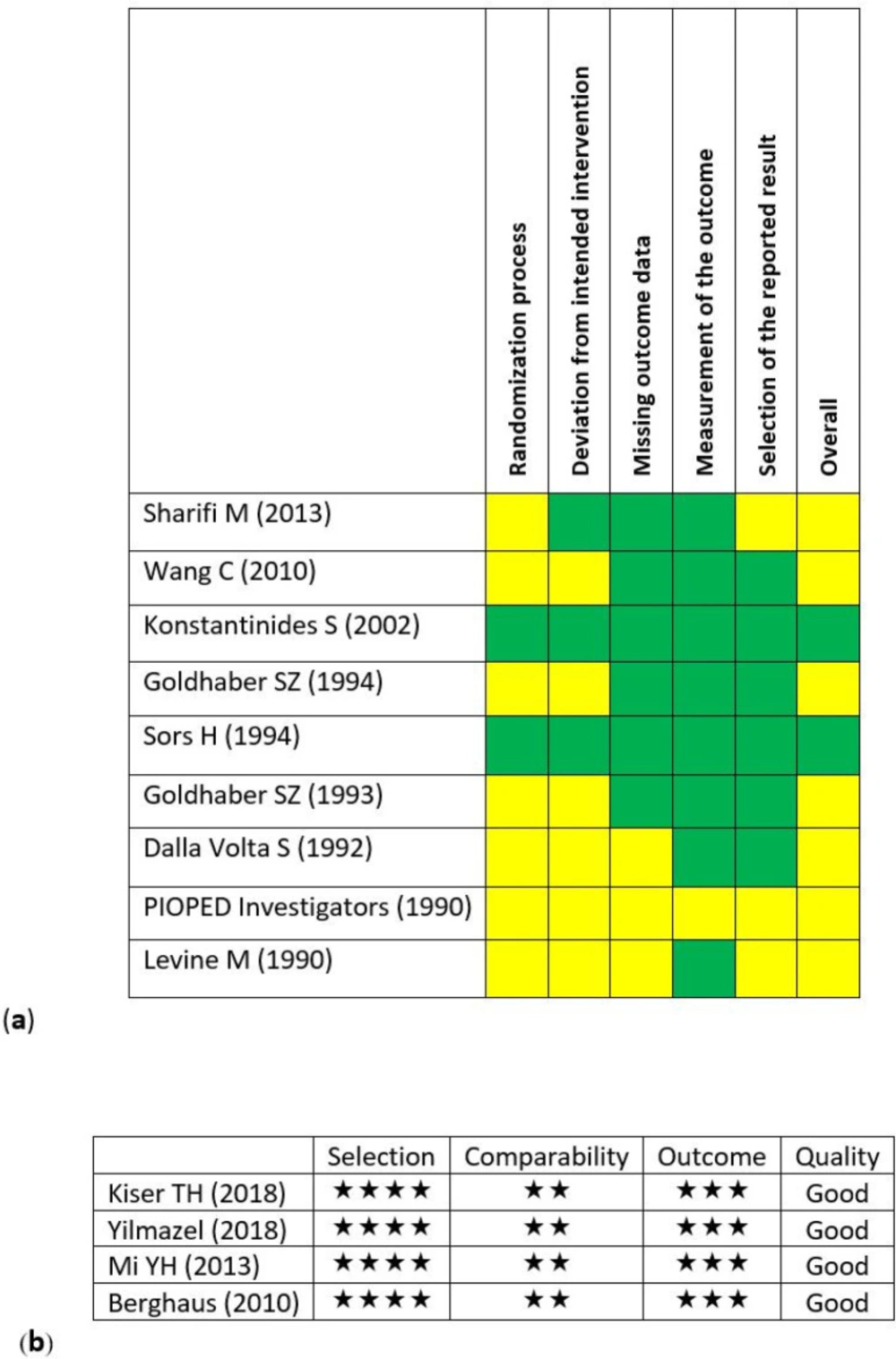
Assessment of the risk of bias in the primary studies. (a) Clinical trials (by using Cochran’s risk of bias (RoB2) tool). (Green: low risk, yellow: some concerns and red: high risk) (b) Cohort studies (by using Newcastle-Ottawa assessment scale (NOS)).
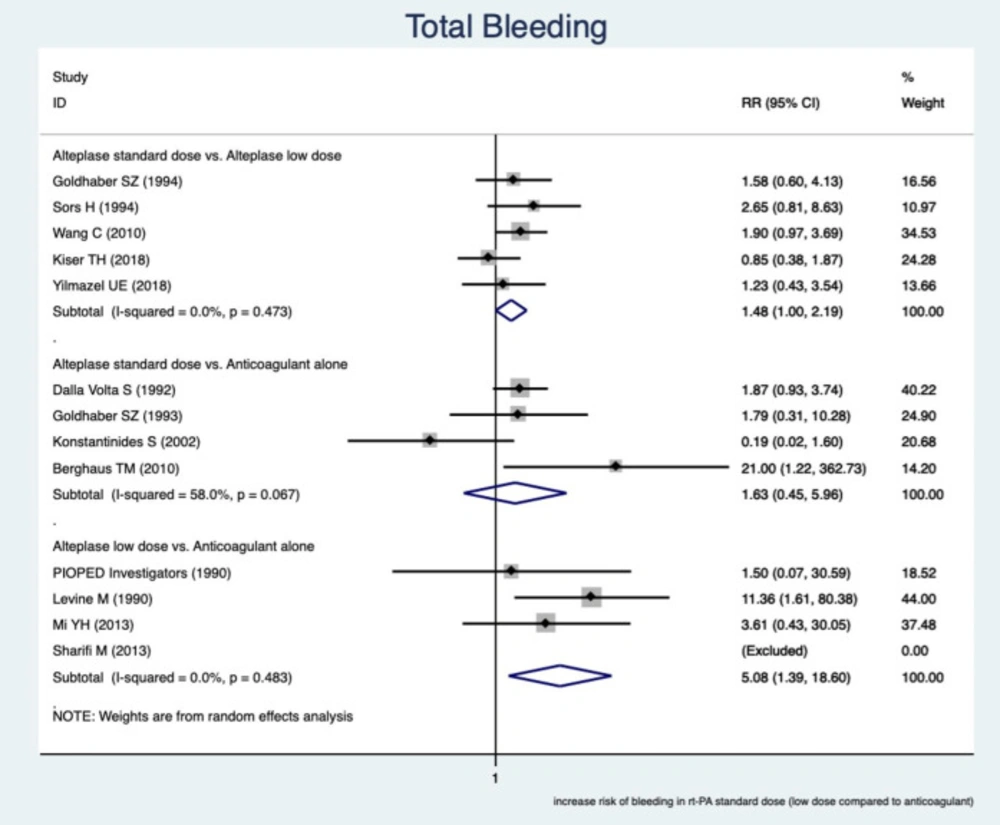
Forest plot of pooled estimate relative risk (RR) to evaluate the association between different subgroups and bleeding
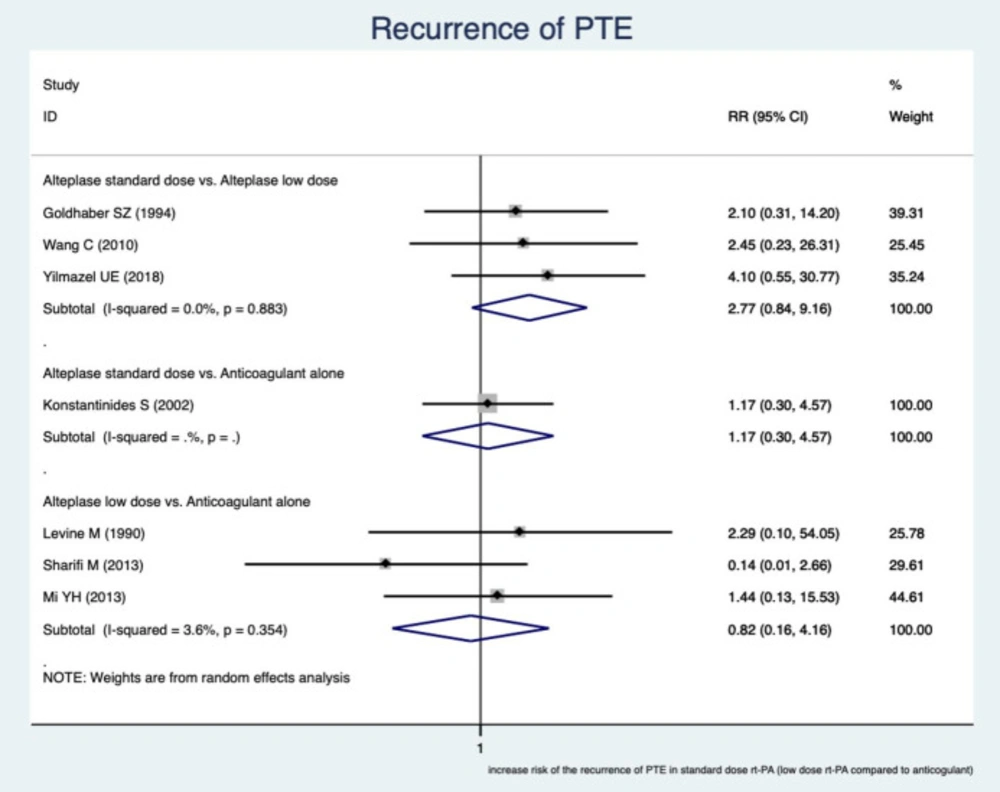
Forest plot of pooled estimate relative risk (RR) to evaluate the association between different subgroups and recurrent pulmonary embolism
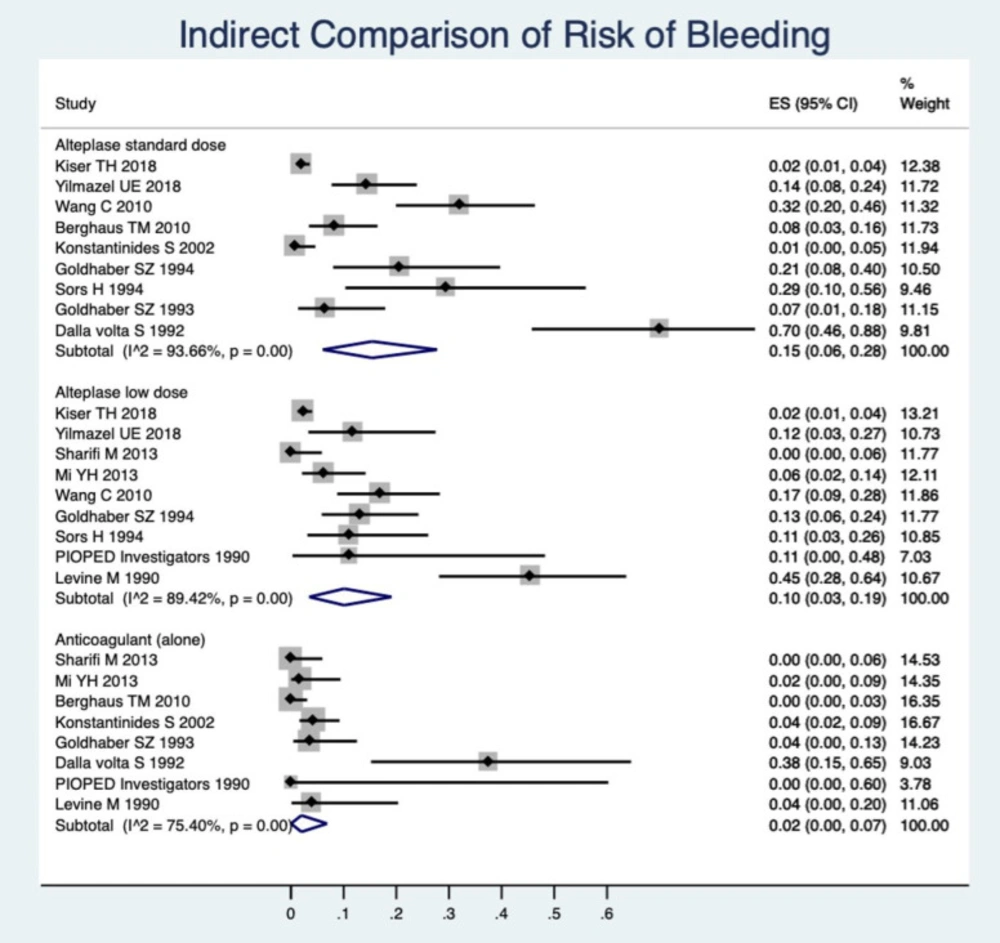
Indirect comparison of the pooled estimate of incidence rates of total bleeding between the anticoagulation drugs
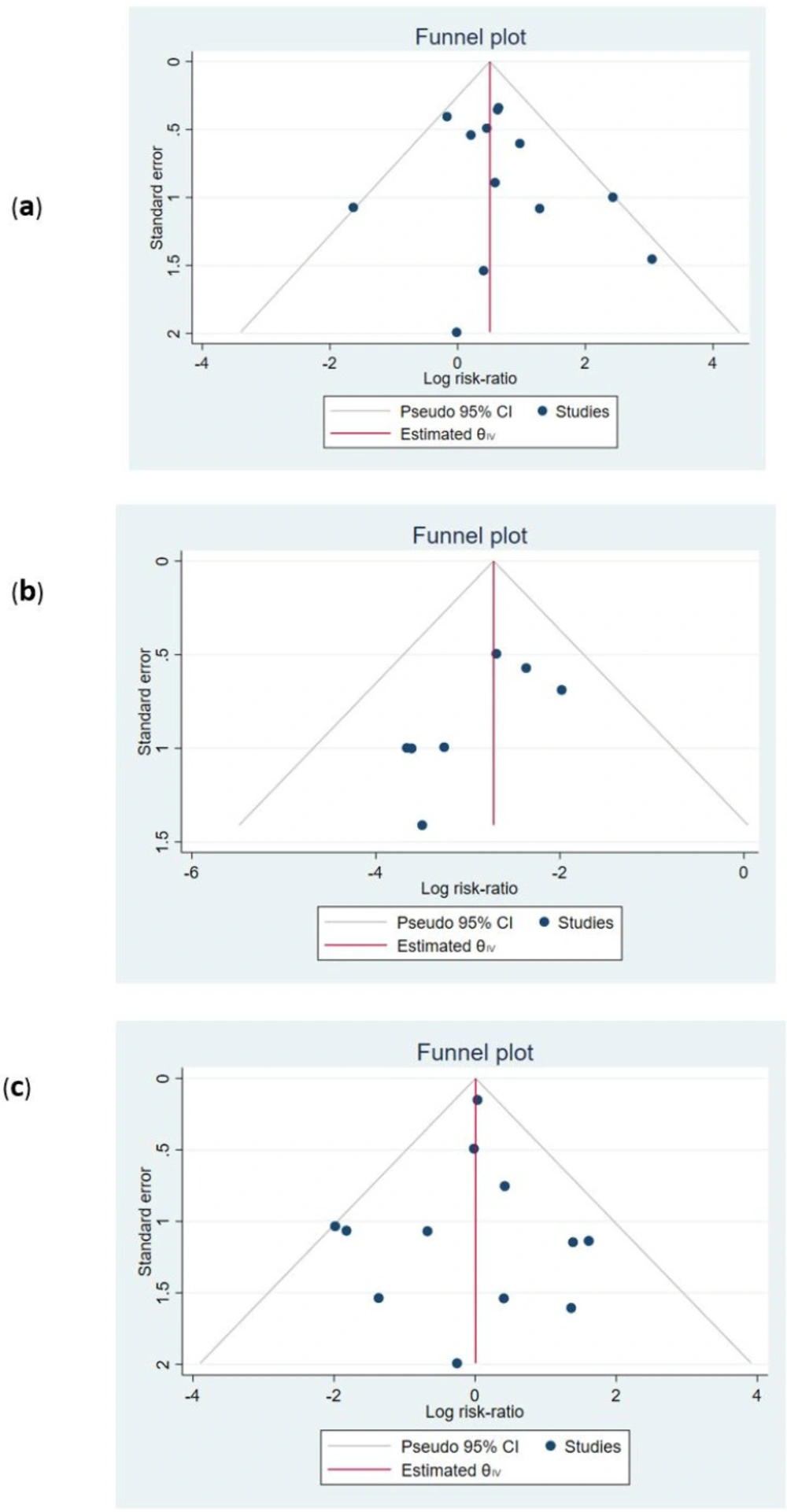
Funnel plot for the assessment of publication bias. (a) total bleeding; p-value for Egger test: 0.417. (b) Recurrence of pulmonary thrombo-emboli; Egger test p-value: 0.175. (c) Mortality; Egger test p-value: 0.720


