This study was carried out to evaluate the beneficial effects of TMZ on vascular miRNAs, lipid profile, inflammation, and hypotension in the alloxan-induced diabetic animals. In line with previous studies, the present study also observed decreased miR-24, miR-126, blood pressure and increased inflammatory cytokines, oxidative stress and dyslipidemia in the diabetic rats. Furthermore, this study found that decreased TG, TC, inflammatory cytokines and oxidative stress with TMZ treatment significantly improved these alterations in vascular miRNAs in the diabetic rats. Collectively, these findings demonstrated an important role of vascular miRNAs in mediating vascular disorders in diabetes.
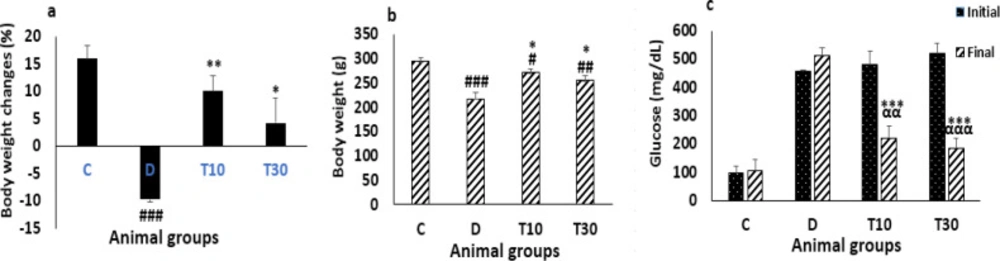
After administration of TMZ for eight weeks in the diabetic rats, blood glucose was improved in our investigation. One of the main mechanisms of TMZ treatment might be blood glucose improvement by reducing insulin-resistance. Researchers have also found that insulin-resistance reduction resulted from TMZ treatment is associated with the alleviated insulin signaling pathway phosphatidylinositol 3-kinase (PI3-K)/Akt (
28). This pathway is an important factor in the insulin signal transduction and plays a key role in the metabolism of lipid and glucose. In addition, TMZ could increase translocation of GLUT4 to the sarcolemma in skeletal muscle cells (
29). A previous study has demonstrated that activated AMP-activated protein kinase (AMPK) pathway is associated with TMZ administration. The AMPK pathway plays an important role in increasing uptake of glucose and fatty acids, glycolysis, as well as fatty acid oxidation (
30). In addition, in diabetic rats treated with TMZ, increased insulin effect and glucose utilization have been demonstrated (
31,
32).
In the present study, reduced body weight gain was observed in the diabetic rats. Body weight reduction may result from dehydration or metabolism impairment, or both (
33). Therefore, decreased blood glucose may cause increased body weight.
Hyperglycemia and dyslipidemia are associated with macrovascular complications and are linked to an enhanced risk of atherosclerosis (
34,
35).
Increased TC, TG, LDL-c, VLDL-c, and reduced HDL-c that contribute to atherosclerosis have been observed in the diabetic rats, which is consistent with a previous study (
34). However, treatment with TMZ markedly improved the increase in TC, TG, and VLDL-c, suggesting the effect of TMZ treatment on dyslipidemia. On the other hand, reduction of free fatty acid levels in plasma has been demonstrated to cause TMZ treatment in diabetic rats (
36). Thus, these findings showed an important role of TMZ treatment in reducing dyslipidemia induced by diabetes. Collectively, these results propose that improved blood glucose and lipid profile may act simultaneously to contribute to the improvement of body weight in the diabetic rats treated with TMZ.
Oxidative stress and inflammation are associated with diabetes and are linked to atherosclerosis (
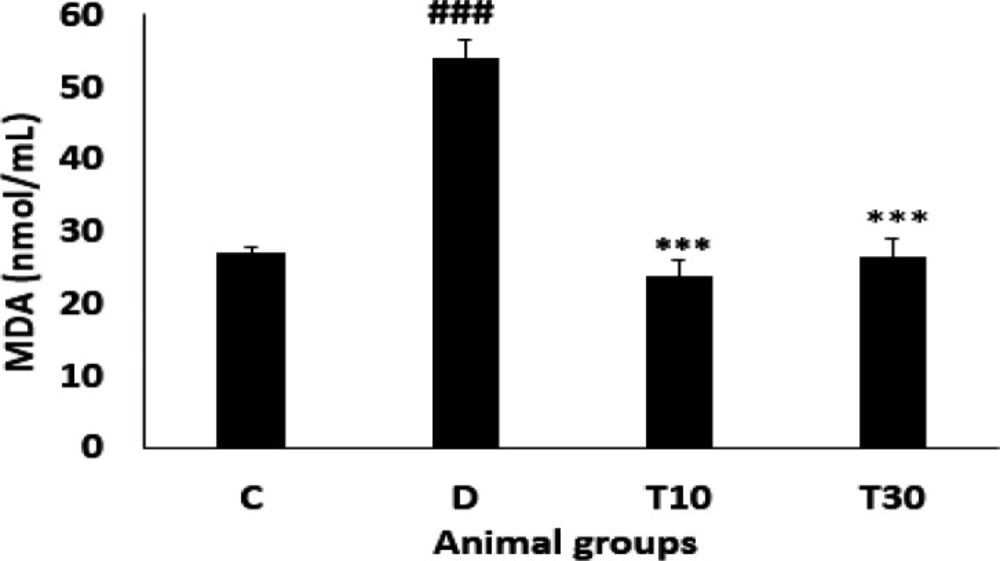
37). In the present study, increased MDA level was found in the diabetic rats, which was improved by TMZ treatment. Similarly, decreased MDA level by TMZ administration has been indicated in animals subjected to myocardial ischemia-reperfusion (
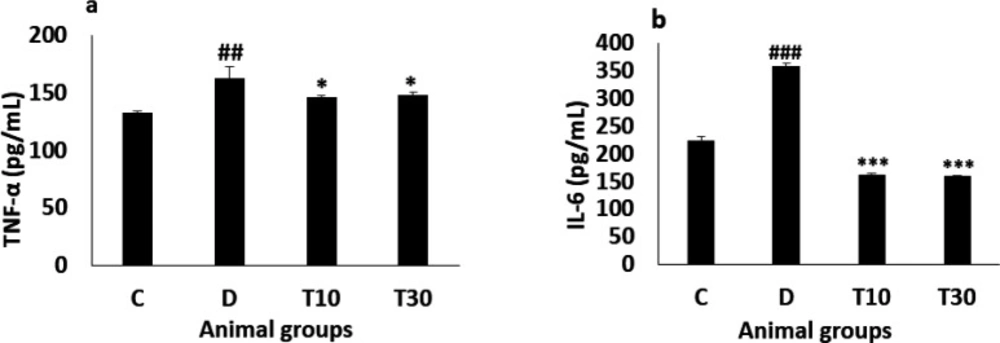
38). Inflammatory cytokines, including TNF-α and IL-6 are associated with diabetes and are linked to increased macro-vascular disorders. In the diabetic animals, we observed increased TNF-α and IL-6 levels, and these alterations were improved with TMZ administration, which is coherent with a previous study in patients with stable coronary artery disease. (
1,
39).
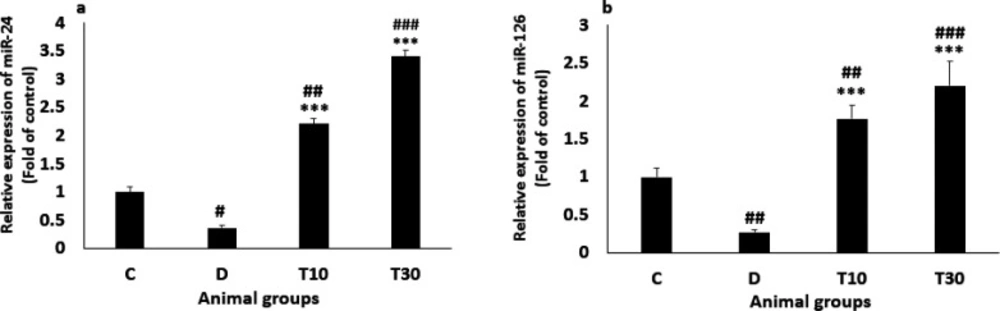
Consistent with previous investigations (
12,
40), we demonstrated that diabetes significantly reduced plasma miR-24 and miR-126 levels compared to the control animals. However, the diabetic rats treated with TMZ significantly increased the levels of both microRNAs, proven that are effective regulators of vascular integrity and angiogenic signaling in the vascular system (
41). A previous study has presented that decreased plasma miR-126 in type 2 diabetic patients may cause increase β cells injury in the pancreas and high blood glucose (
42). Hyperglycemia increased ROS, TNF-α and IL-6, and reduced miR-24 and miR-126 levels in plasma. Decreasing miR-24 and miR-126 levels increased the ROS and inflammatory markers induced by diabetes. Both miRNAs negatively regulated ROS, IL-6, and TNF-α (
43,
11). In addition, decreased miR-126 expression by inflammatory cytokines and increased miR-126 level by anti-inflammatory agents have been reported in endothelial cells and colonic myofibroblasts (
44,
45). The decreased plasma miR-24 level that contributes to endothelial dysfunction has been observed in the diabetic rats, which is coherent with a previous study in diabetic mice (
46). In summary, our results propose that increased plasma miR-24 and miR-126 levels may reduce oxidative stress and inflammation by TMZ treatment in the diabetic rats. Therefore, reducing oxidative stress and inflammation by TMZ treatment may play a key role in decreasing cardiovascular complications in diabetes.
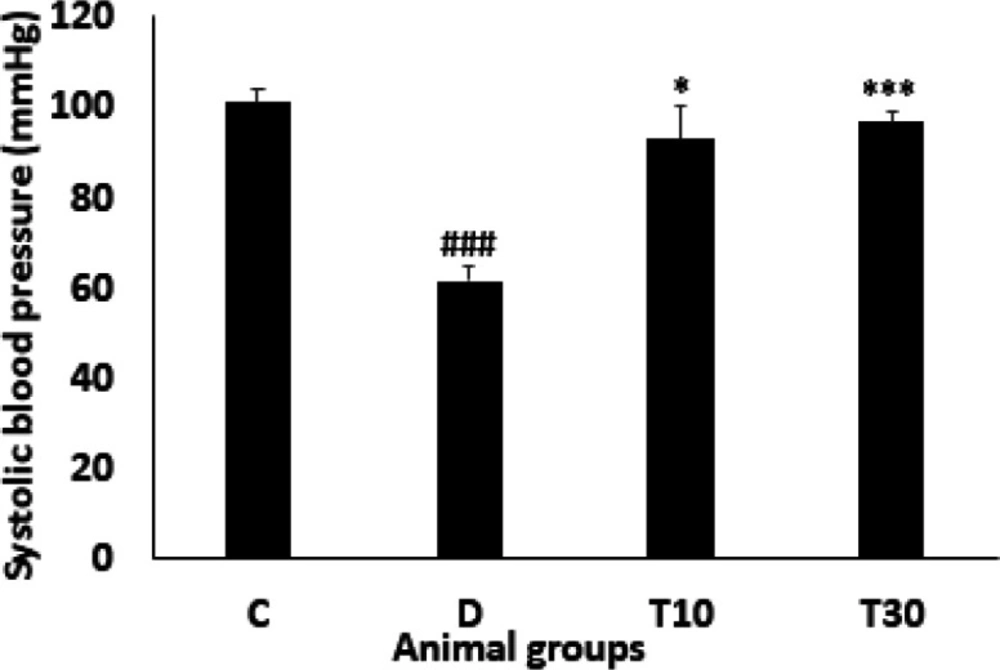
In the diabetic rats, we observed a decrease in blood pressure. The reason for the hypotension may result from reduced cardiac output, impaired cardiac autonomic and elevated plasma nitric oxide in the diabetic rats (
47,
48). Nevertheless, TMZ administration significantly improved the hypotension in the diabetic rats, which may be attributed to the improvement of oxidant/anti-oxidant ratio and glucose metabolism and/or ventricular contractility that have been indicated to contribute to hypotension in diabetes (
47,
49). In addition, miR-24, by regulating VSMCs function, has likewise been reported to play an important role in vascular resistance (
50). Therefore, miR-24 may be involved in decreased hypotension in the diabetic rats, treated with TMZ, and it may require further studies.
| Groups | C | D | T10 | T30 |
|---|
| TC (mg/dL)TG (mg/dL)HDL-c (mg/dL)LDL-c (mg/dL)VLDL-c (mg/dL) | 46.22 ± 1.3736.33 ± 5.5235 ± 0.5324.44 ± 0.57.26 ± 1.10 | 61.75 ± 2.32##52.87 ± 4.78#28.80 ± 2.39#26.75 ± 0.7010.57 ± 0.94# | 48.12 ± 2.43**24.62 ± 2.59**26.87 ± 1.6325.1 ± 1.384.92 ± 0.51** | 45.90 ± 3.93***30.10 ± 4.99**31 ± 0.7124 ± 0.616.02 ± 0.99** |
Body weight changes percent (a), body weight (b) and blood glucose level (c) (mean ± SEM, n = 8) in control (C), diabetic (D), diabetic treated with TMZ at 10 and 30 mg/kg (T10 and T30, respectively). ααP < 0.01, αααP < 0.001 final vs. initial. #P < 0.05, ##P < 0.01, ###P < 0.001 vs. final control group. *P<0.05, **P<0.01, ***P < 0.001 vs. untreated diabetic group, one-way ANOVA followed by LSD post hoc test
Plasma MDA level (mean ± SEM, n = 8) in control (C), diabetic (D), diabetic treated with TMZ at 10 and 30 mg/kg (T10 and T30, respectively). ###P < 0.001 vs. control group, ***P < 0.01 vs. untreated diabetic group, one-way ANOVA followed by LSD post hoc test
Plasma TNF-α (a) and IL-6 (b) values (mean ± SEM, n = 8) in control (C), diabetic (D), diabetic treated with TMZ at 10 and 30 mg/kg (T10 and T30, respectively). ##P < 0.01, ###P < 0.001, vs. control group, *P < 0.05, ***P < 0.001 vs. untreated diabetic group, one-way ANOVA followed by LSD post hoc test
Plasma miR-24 (a) and miR-126 (b) values (mean ± SEM, n = 8) in control (C), diabetic (D), diabetic treated with TMZ at 10 and 30 mg/kg (T10 and T30, respectively). #P < 0.05, ##P < 0.01, ###P < 0.001, vs. control group, ***P < 0.001 vs. untreated diabetic group, one-way ANOVA followed by LSD post hoc test
Systolic blood pressure (mean ± SEM, n = 8) in control (C), diabetic (D), diabetic treated with TMZ at 10 and 30 mg/kg (T10 and T30, respectively). ###P < 0.001 vs. control group, *P < 0.05, ***P < 0.001 vs. untreated diabetic group, one-way ANOVA followed by LSD post hoc test