We hypothesized that exposure to antineoplastic drugs leads to increased toxicity in blood lymphocytes in the hospital nurses or staff occupationally exposed to anticancer drugs. Through observation and biochemical experiments, our study results proved that toxicity parameters increased in blood lymphocytes of exposed group compared to those of unexposed nurses. Through different studies show that surface contamination, and accordingly the potential for occupational exposure to antineoplastic drugs, occurs at every stage of the hospital medication system (
2). Those job categories most likely in risk of exposure are nurse, pharmacy technician, pharmacy receiver, and pharmacist. Over 11 job categories (not including housekeeping) per site are potentially at risk of exposure. Several studies have shown that exposure to antineoplastic drugs can cause toxic effects (
2). Dermal exposure has been suggested to be the main route of exposure (
29). In a recently study, was assessed dermal exposure to cyclophosphamide. Surprisingly, exposure levels detected on the hands during nursing tasks were higher than those measured in the hospital pharmacy during preparation of cyclophosphamide. The positive urine samples with detectable cyclophosphamide and other anti-neoplastic drugs were observed in hospital personals (
29). Also studies show that the prevalence of needle stick injury (NSI) in Iranian nurses is high that likelihood exposure to anti-neoplastic drugs has increased (
30).
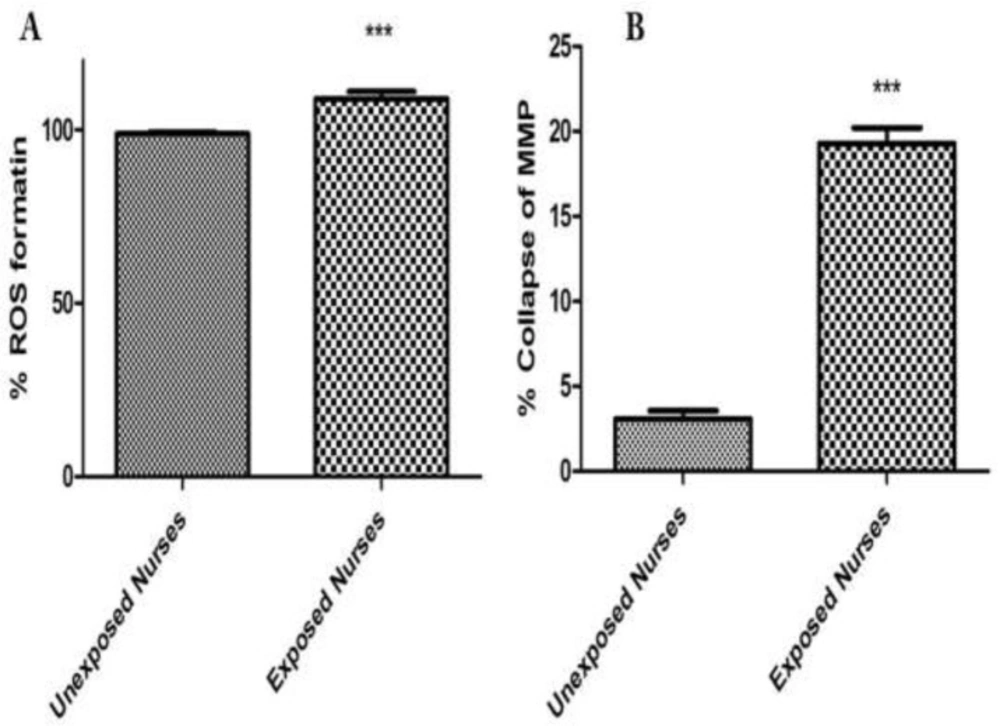
ROS formation was compared between occupationally exposed nurseꞌs lymphocytes and unexposed. Referring to the results of ROS formation status in the present study, it was shown that cellular and mitochondrial ROS formation was significantly increased in the lymphocytes of occupationally exposed group, compared to those of unexposed control (
P < 0.05) (
Figure 1A). Neoplastic disease studies revealed that treatment with anti-neoplastic drugs increases ROS and reduces plasma levels of vitamins C and E as well as of glutathione peroxidase (
31). Consumption of variety of anti-cancer drugs have been associated with oxidative stress. For example, cisplatin induces formation of reactive oxygen species (ROS) in renal proximal tubular cell mitochondria, eliciting oxidative alterations in lipids, proteins, and DNA of this organelle (
32), while doxorubicin induced cytotoxicity has been associated with ROS production and in particular to presence of the superoxide anion radical and of hydrogen peroxide in cardiomyocytes (
33). This drug is also able to produce reactive nitrogen species. The oxidant RNS such as peroxynitrite is known to induce protein oxidation and nitration in the absence of GSH, eliciting mitochondrial dysfunction and eventually leading to irreversible damage and severe loss of cellular ATP (
34). A recent study has also indicated that exposed nurses to antineoplastic drug suffer from oxidative stress compared to unexposed nurses (
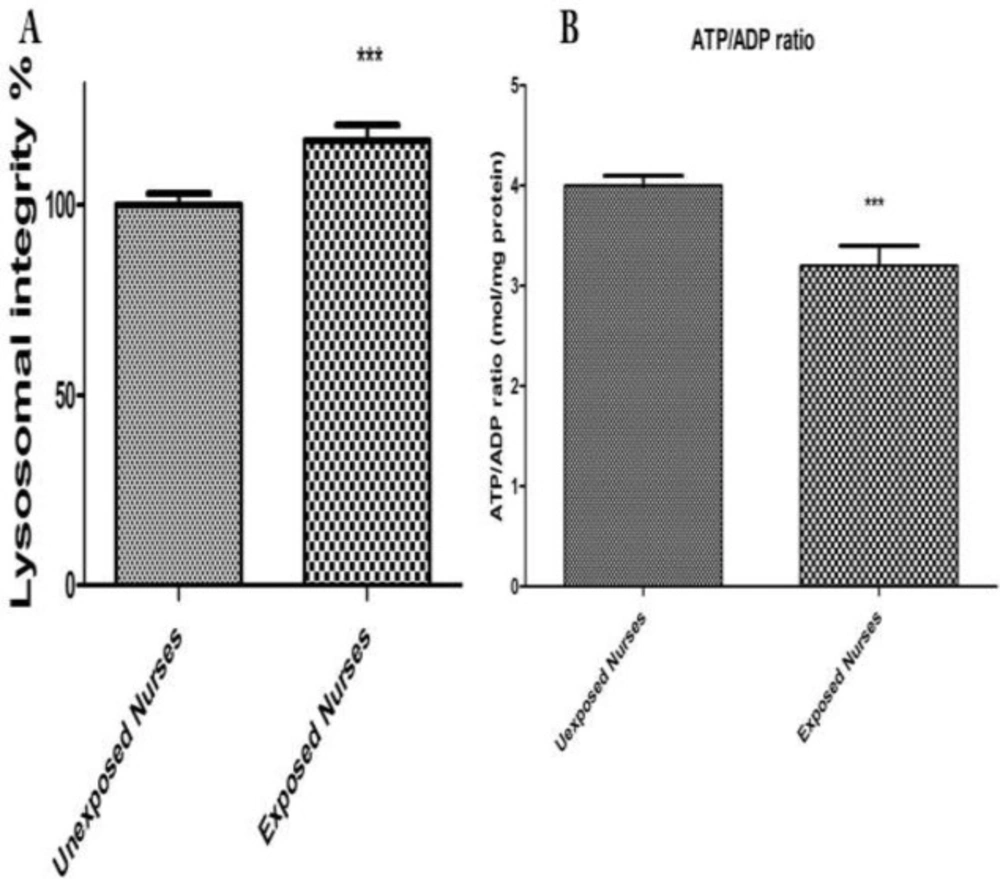
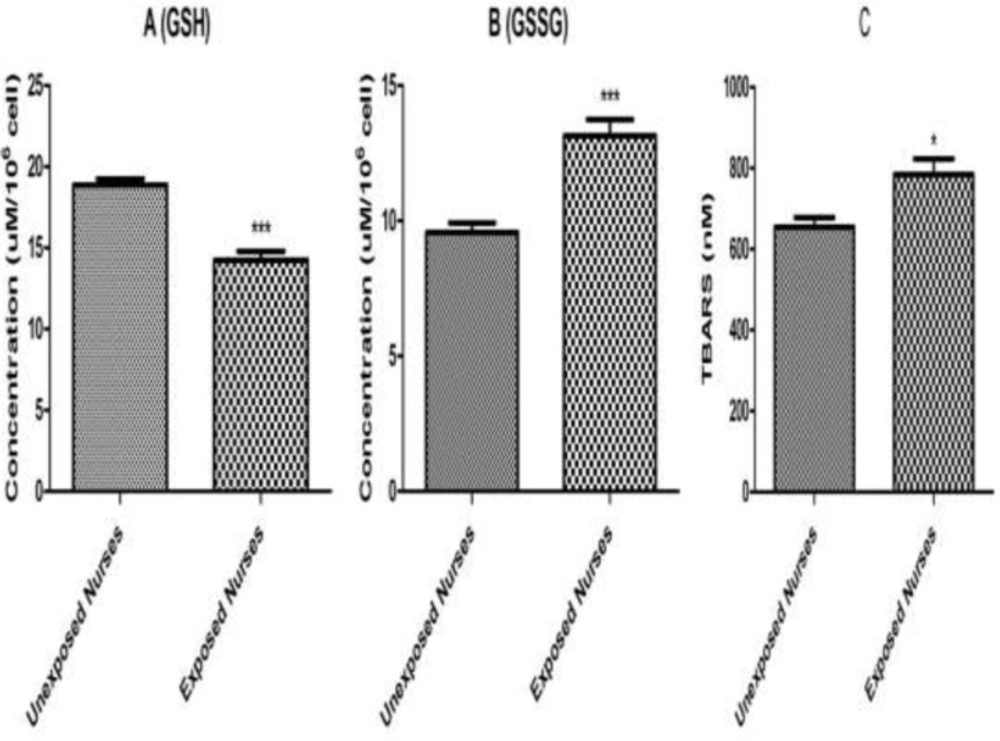
35). It is worth noting that both drugs are prepared, handled, and administered by nursing personnel in hospitals. Our results proved that content of glutathione and ATP has decreased in occupationally exposed nurses lymphocytes in comparison to unexposed nurses (
Figure 3 and
Figure 2B). The decreases in lipid peroxidation level found in our study may be explained by an increase in ROS formation produced by anti-neoplastic drugs in occupationally exposed nurseꞌs lymphocytes, such as superoxide anion and hydrogen peroxide, which are known to attach to membrane lipids, initiating lipid peroxidation. Similarly, increased ROS formation may directly oxidize the prosthetic protein group or else reacts directly with the peptide chain, leading to conformational and functional changes in cellular organelles such as mitochondria and lysosomes (
36-
38). The results of this study also showed occurrence of mitochondrial and lysosomal damages in occupationally exposed nurseꞌs lymphocytes, compared to the control group (
P < 0.05) (
Figure 1B and
Figure 2A).
Previous studies indicated an increased risk of a prolonged time to pregnancy among nurses with relatively high exposure to antineoplastic agents compared with referent nurses (
39). In addition to the toxicity to reproduction system, antineoplastic drugs have been found to have carcinogenic potential. Nine antineoplastic drugs have been classified by IARC to be carcinogenic to humans. The leukemia risk of an oncology nurse after 40 years of dermal exposure to cyclophosphamide was estimated to be on average of 0.27 (range = 0 - 40) extra cases per million oncology nurses (
40).
Mitochondria perform significant roles in cellular energy metabolism, free radicals generation, control of cell death, growth, development, integration of signals from mitochondria to nucleus and nucleus to mitochondria, and various metabolic pathways (
41,
42). Introduction of mtDNA mutations in transformed cells has been associated with increased ROS production and tumor growth. Studies revealed that increased and altered mtDNA plays a role in the development of cancer (
43). Mitochondrial alterations have been identified in several cancers (
44). An increase in mtDNA copy number was observed in patients with a higher risk for breast cancer (
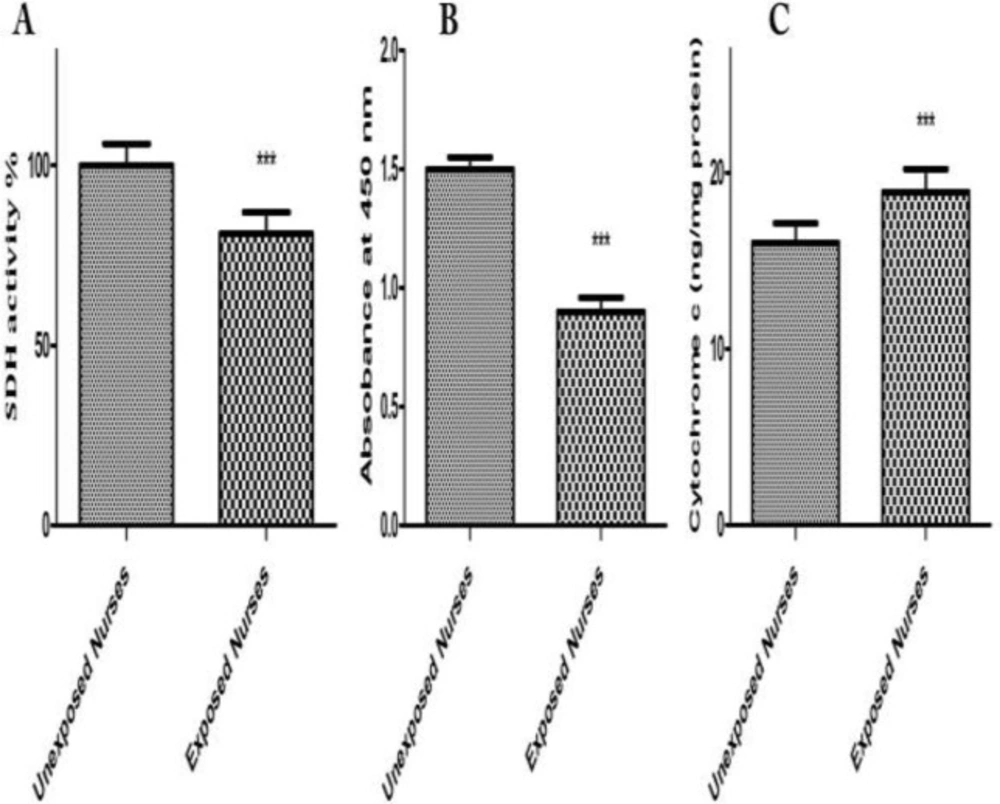
45). Our results on isolated mitochondria obtained from occupationally exposed nurseꞌs lymphocytes showed significant mitochondrial toxic changes such as mitochondrial swelling, inhibition of SDH and cytochrome C release (
Figure 4). Mitochondrial alterations have been associated with some forms of cancer and an increased risk of certain age-related disorders such as heart disease, Alzheimer disease, Parkinson disease and immunotoxicity (
46). Additionally, our results suggest that the gradual and progressive occurrence of these alterations in exposed oncology drugs may play a role in progression of mentioned diseases.
Our results showed that occupationally exposed nurseꞌs lymphocytes were more susceptible to oxidative stress than unexposed nurses. Finally, isolated mitochondria from lymphocytes could be a biomarker for determination people at risk of oxidative diseases such as cancer and aging.