Experimental animals
Adult female Wistar rats, weighing 170–200g were purchased from the Modern Veterinary Office for Laboratory Animals (Cairo, Egypt). Rats were housed in well ventilated opaque propylene cages with free access to commercial diet and tap water. Rats were maintained at 22 ± 2 °C under light and dark cycle and they were allowed to acclimatize for one week prior to the study. Handling of animals and animal care were done according to the guidelines of Beni-Suef Animal House approved by the Pharmacology and Toxicology Department, Faculty of Pharmacy, Beni-Suef University, which were based on the guidelines suggested by the recommendations of the National Institutes of Health (NIH) Guide for Care and Use of Laboratory Animals (Publication No. 85-23, revised 1985). All experimental protocols were approved by Research Ethics Committee at the Faculty of Pharmacy, Beni-Suef University (Egypt).
Drugs, chemicals and diagnostic kits
Losartan, prednisolone, and Complete Freund’s Adjuvant (CFA) were purchased from Sigma-Aldrich Chemical Company (St. Louis, MO, USA). Serum rheumatoid factor (RF) ELISA kit and erythrocyte sedimentation rate (ESR) kits were purchased from CliniLab Company (Cairo, Egypt). Serum TNF-α and IL-6 ELISA kits were obtained from Glory Science Company (St. Del Rio, USA). Serum high density lipoprotein (HDL), total cholesterol (TC), and triglycerides (TG) enzymatic reagent kits were obtained from Assaypro LLC (St. Charles, MO, USA).
Serum glutathione (GSH), malondialdehyde (MDA) colorimetric reagent kits and complete blood count kit were purchased from Bio Diagnostic Company (Giza, Egypt). All other chemicals included were of the highest analytical grade available. Drugs used were suspended in 1% Tween 80 shortly before administration to animals.
Experimental design
After one week of acclimatization to the laboratory conditions, fourty rats were randomly allocated into four groups (n = 10) placed in individual cages and classified as follows: Group 1 served as vehicle control and received an injection of 0.2 mL of paraffin oil into the right hind paw every four days for twelve days and 1% of tween 80 in 0.9% physiological saline solution (0.1mL/ 100g body weight;p.o) on day thirteen for two weeks. The remaining three groups received subcutaneous injection of 0.2 mL of CFA (heat killed powdered mycobacterium cells suspended with liquid paraffin) in the planter surface of the right hind paw (
7) every four days for twelve days. On day thirteen, the treatment with various drug regimens started and continued up to two weeks. The second group was assigned as AIA control and received 1% tween 80 dissolved in 0.9% physiological saline solution (0.1mL/ 100g body weight;p.o). Groups 3 and 4 received prednisolone (10 mg/kg/day;p.o.) (
1) and losartan (20 mg/kg/day;p.o.) (
4) Respectively.
Induction of adjuvant arthritis
In order to induce a chronic rat model of arthritis and exclude the presence of just temporary inflammatory reaction, an aggressive modified model of adjuvant arthritis was used. Complete Freund’s adjuvant (5 mg of heat killed, powdered mycobacterium tuberculosis cell was suspended in liquid paraffin to get 5mg/mL suspension) was used to induce arthritis in rats. Pilot studies with the aid of a histopathological study on joint sections were performed to assess the success of the model.
Blood collection and processing of samples
At the end of the experimental period (day 27), blood samples were collected from orbital venous plexus from animals under light sodium phenobarbital (40 mg/kg) anesthesia sodium. Each sample was divided into two portions; the first portion was used for erythrocyte sedimentation rate (ESR) evaluation and hematological parameters including assessment of white blood cells (WBCs), red blood cells (RBCs), hemoglobin (Hb), hematocrit (Hct) and platelets values. The second part was collected into non heparinized tubes and centrifuged at 3000 rpm for 10 min using a cooling centrifuge (Sigma 3-30k, USA). Then, serum samples were separated, collected in clean tubes, and stored at -80 °C until use. The Serum was used for the determination of the levels of tumor necrosis factor (TNF-α), interleukin-6 (IL-6), rheumatoid factor (RF), glutathione (GSH), malondialdehyde (MDA), total cholesterol (TC), triglyceride (TG), high density lipoprotein (HDL), and low density lipoproteins (LDL).
Determination of serum TNF-α and IL-6 activities
Serum TNF-α and serum IL-6 were determined using Enzyme Linked Immunosorbent Assay (ELISA) kits according to the method described by Paine
et al. (2012) and Rysz
et al. (2006) respectively (
8,
9).
Determination of ESR and RF levels
ESR and RF were determined using diagnostic kits according to the methods described previously (
10;
11) and following the manufacturer’s instructions.
Determination of oxidative stress parameters
Serum GSH and MDA levels were determined according to the method described by Pedrini
et al. (2012) (
12) and Padurariu
et al. (2010) (
13) respectively using diagnostic reagent kits.
Determination of serum levels of TC, TG, HDL and LDL
Serum TC, TG, and HDL levels were estimated using diagnostic kits according to the methods described by Akbas
et al. (2010) and Zheng
et al. (2011) (
14;
15) respectively. Low density lipoprotein (LDL) level was calculated according to the formula described previously (
16) :
LDL = total cholesterol−HDL−TG/5.
Determination of hematological parameters
Blood smears containing EDTA were prepared as soon as possible after blood collection on a glass slide, quickly dried, and stained with Giemsa and May-Grunwald stain for the determination of total number of WBCs, RBCs, Hb concentration, platelets count, and Hct value. All were estimated by adopting standard procedures according to the method of Flouris
et al. (2012) (
17).
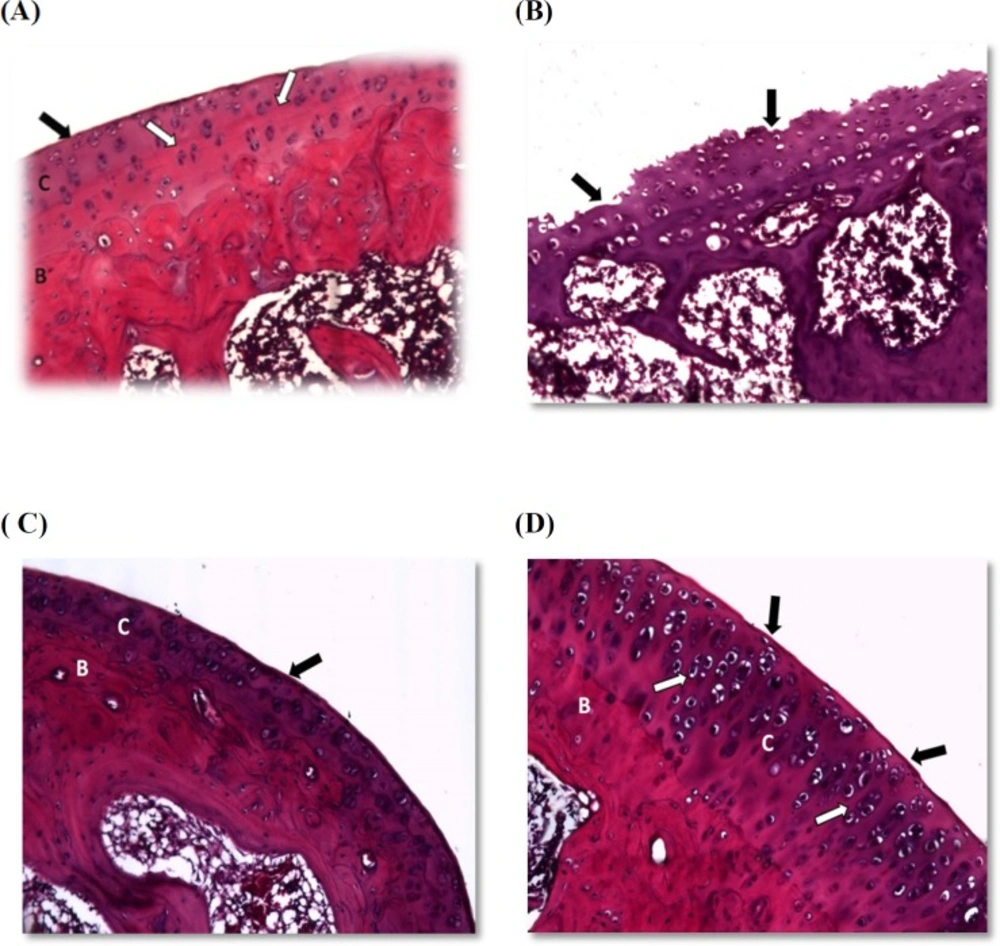
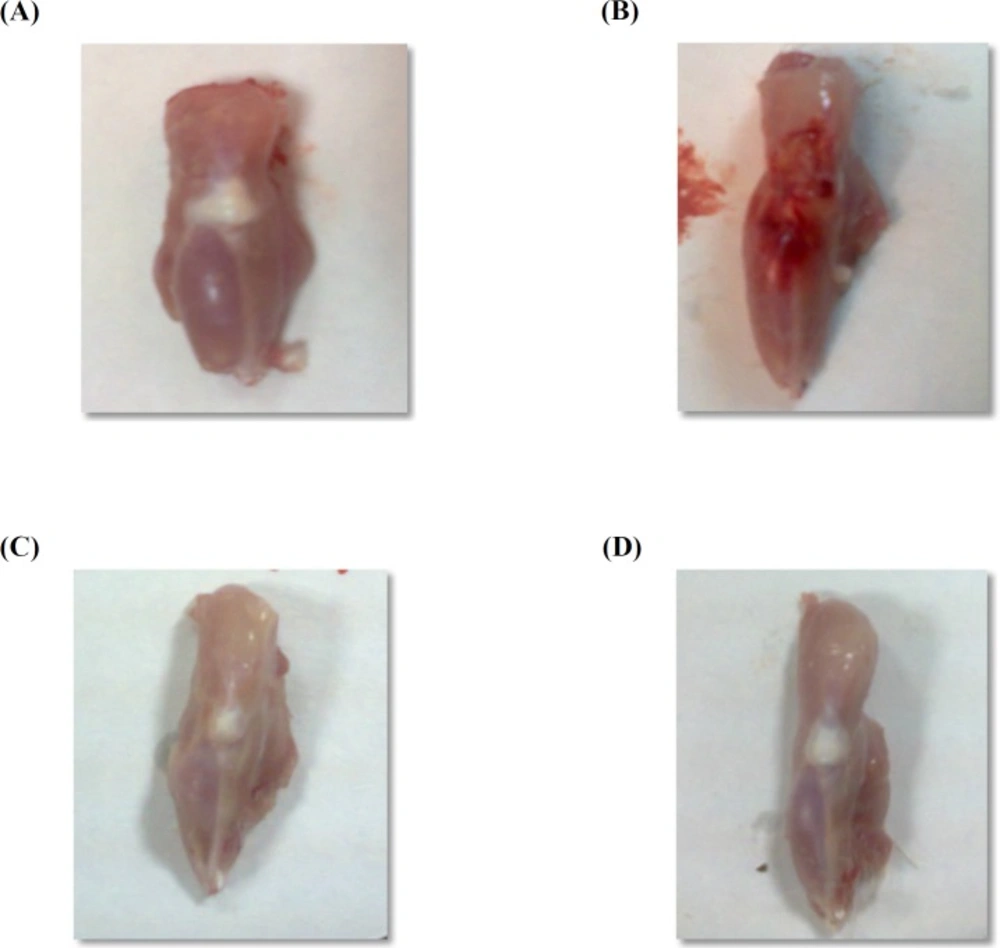
Hind paw processing and histopathological examination
Immediately, after blood withdrawal, the rats were anesthetized with thiopental sodium (50 mg/kg) and killed by decapitation. Whole knee joints, including synovium, adjacent tissues and bones, were carefully exposed, separated, and preserved in 10% formalin solution in saline in labeled well-sealed containers. After tissue hardening, the joints were transversely sectioned (4-5μm thick sections) and stained with standard Hematoxylin and Eosin (H&E) dye and evaluated microscopically using a light microscope (
18) .
Statistical analysis
The data were expressed as means ± standard deviation (SD). The statistical analysis was performed using Graphpad prism software program, version 5.01 (GraphPad Softwae, Inc, San Diego, USA).
One-way analysis of variance (ANOVA) followed by Tukey-Kramer multiple comparisons test was used for comparison of means of different groups. The level of statistical significance was set at
p < 0.05.