Menopause is described by a decline in estrogen levels, which activates the uncomfortable symptoms of hot flushes, night sweats, sleep disorders, and vaginal atrophy. Among these signs, vaginal dryness and vaginal atrophy are reported by many women to be the most annoying (
1). Vaginal atrophy is a chronic and progressive condition characterized by thinning, drying and inflammation of the vaginal walls due to lower level of estrogen (
2,
3). About 50 percent of women experience vaginal atrophy, also referred to as genitourinary syndrome of menopause, during and after the menopause; its symptoms include dyspareunia, irritation, bleeding during intercourse, burning and itching (
4,
5). Despite other symptoms derived from hypoestrogenemia, like flashing, this condition would not tend to diminish over time (
2). This condition wields a significant effect on their attitudes towards sexuality and healthcare and on their quality of life (
6,
7). In spite of a wide range of effective hormonal and non-hormonal treatments available to relieve vaginal atrophy symptoms and improve quality of life, many women are unaware of their existence or are unwilling to use them (
8). However, it is well understood that hormone replacement therapy (HRT) has some disadvantages and deals with side effects that could be challenging. Lack of compliance and fearing of cancer make patients leave the treatment regimen (
9,
10).
In comparison with other menopausal complaints, lower estrogen levels are needed to keep up vaginal health and this could be a positive therapeutic aspect of this condition (
11). Both systemic and local estrogen derivatives can alleviate vaginal dryness symptoms and restore vaginal moisture (
12). Consequently, introduction of plant derived alternatives for hormone replacement therapy, provide another chance to treat this condition. Phytoestrogens are plant compounds with estrogen-like properties (
13). Two major groups of phytoestrogens are isoflavones and lignans; soybeans are affluent in isoflavones, and lignans are found in flaxseed, whole grains, legumes, fruits, and vegetables (
14). Soy, red clover, and flaxseed based products are excellent source of these compounds (
13,
15-
17).
Although administration of such these is increasing in these days, no consensus has been reached and most of the studies are inconclusive (
18). The aim of this study was to perform a meta-analysis of high-quality, randomized, controlled trials (RCTs), to investigate the effectiveness of phytoestrogens in alleviating the menopausal symptoms (vaginal atrophy).
Methodology
In the current study, the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed to report a systematic review and meta-analysis (for details on further use, see the PRISMA website, www.prisma-statement.org).
Information Resources and Search Strategies
Variety of databases including PubMed, Scopus, and Cochrane Central Register of Controlled Trials (CCRCT) were searched according to the below-mentioned pre-specified search strategy and using the relevant MeSH terms. The databases were searched for articles published up to the end of May 2015, regardless of any limitation such as the language barrier.
Search Strategy
In the present study, the search strategy followed was as follows: (Vagina) AND (complementary treatments OR alternative treatments OR nonhormonal OR phytomedicine herbal treatments OR herbs OR red clover OR soy).
Inclusion Criteria
Evaluating the effectiveness of non-hormonal or herbal treatments on the alleviation of vaginal atrophy in postmenopausal women and considering the following criteria, all the studies were chosen to be involved in a systematic review. These criteria were as follows:
1. Postmenopausal women participating in the study ought to have at least one year of amenorrhea.
2. At least one of the following indexes is presumed to be reported for the patients with atrophic vaginitis:
a. Vaginal atrophy should be reported by the vaginal cell maturation index.
b. The study should be designed as a randomized, controlled clinical trial.
c. The studied patients should not simultaneously take other hormonal or non-hormonal medications.
d. The study should report the required quantitative data to do a meta-analysis.
Interventions
The interventions of this study included prescribing non-hormonal or herbal drugs to alleviate vaginal atrophy in postmenopausal women.
Implications
In this meta-analysis study, the vaginal cell maturation index (as a measure of vaginal atrophy) was considered as the primary outcome measurement.
Data Extraction
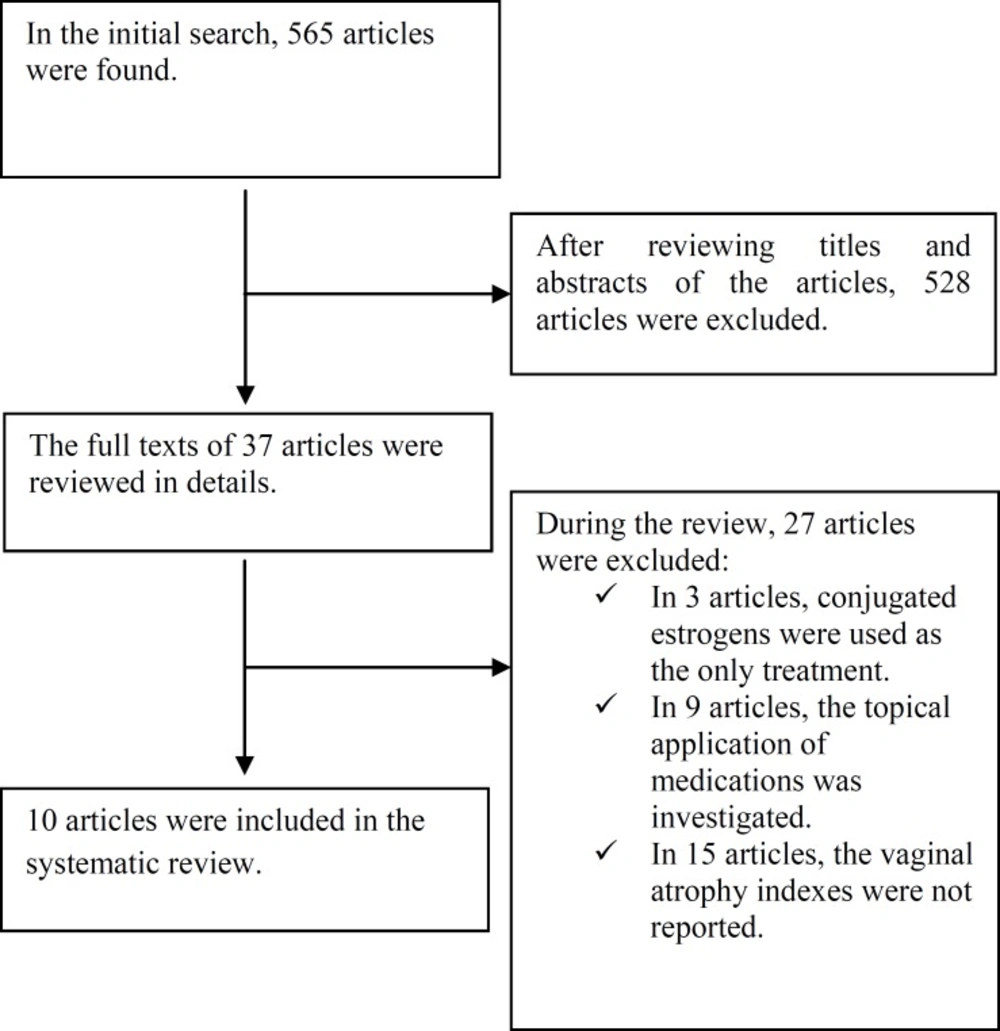
At first, general interest databases consisting of Web of Science, PubMed, Scopus, Google scholar, and Cochrane Library hosting the Central Register of Controlled Trials (CENTRAL) were searched and the search results were entered in the initial list by the researchers. Then, an in-depth research was conducted on the treatments for vaginal atrophy through subject-specific databases. Moreover, in Scopus and PubMed, the key journals related to the issue at hand were manually searched for the content of tables. The researchers made use of the list of references of the chosen articles. In addition, some experts and authors of the articles were consulted in this study. The PRISMA checklist was used to guide the reporting of the systematic review. The search results were entered in
Figure 1. Data collection and analysis were done using the
Cochrane Handbook for Systematic Reviews of Interventions.
In the next phase of the study, two reviewers (M. G. and E. H.) independently screened articles obtained from the search. Initially, in order to attain the eligibility criterion, the titles and abstracts obtained in the search were scrutinized by considering inclusion criteria; thus, the articles which did not meet the inclusion criteria were excluded from the study. All the articles and the tables included in them were carefully scrutinized so as to determine the design of the study and necessary information to evaluate interventions. The reference lists of the articles were reviewed to find out any related article and include it in the study. Any disagreement on the above-mentioned articles between the two reviewers was resolved after additional discussion until a consensus was reached.
Assessing the Quality of Eligible Studies
In the research team, two reviewers were selected to assess the quality of the articles by the use of the CONSORT (CONsolidated Standards of Reporting Trials) checklist which was a version of the 2001 CONSORT checklist for reporting trials with medicinal herbs. This checklist was reviewed and changed to some extent. After the two reviewers reached a consensus, the 22-item checklist was utilized to assess the quality.
Data extraction was conducted independently by two reviewers, and any discrepancy discussed until agreement was reached. Besides, at the beginning of the extraction process, after discussing any disagreement, the two reviewers with the assistance of a field supervisor entered into agreements with each other and the designed form was used for data extraction. The extracted data consisted of the year of publication, number of patients in the two segregated groups, age range, duration of menopause, type and dose of herbal treatment, attrition rate, duration of treatment, and the measured values of the desired outcome.
Statistical Analysis
The quantitative data extracted from the compiled articles were analyzed and summarized using the Comprehensive Meta-analysis (CMA) software. In this meta-analysis, the vaginal cell maturation index as a measure of vaginal atrophy was considered to be the primary outcome measurement. The sample size, average values before and after the treatment, and standard deviation values of the measured outcome were needed to perform a meta-analysis.
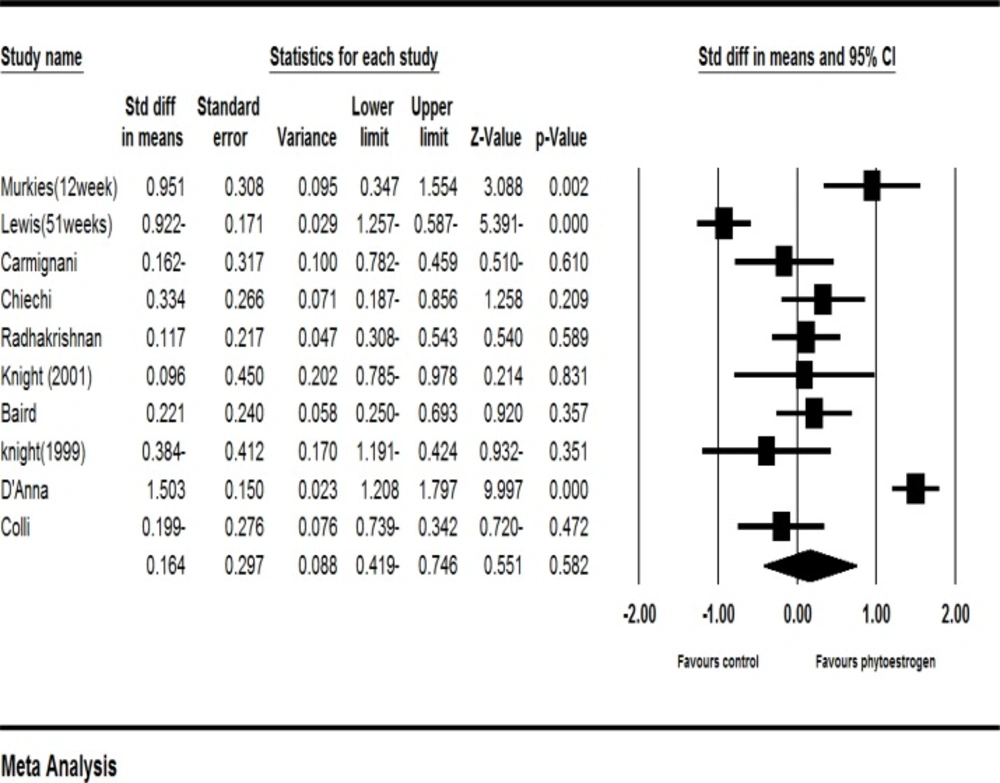
The mean difference was applied as an estimate of the main effect size. Moreover, due to the considerable heterogeneity among studies, the random-effects model was used to obtain the pooled effect size derived from primary studies.
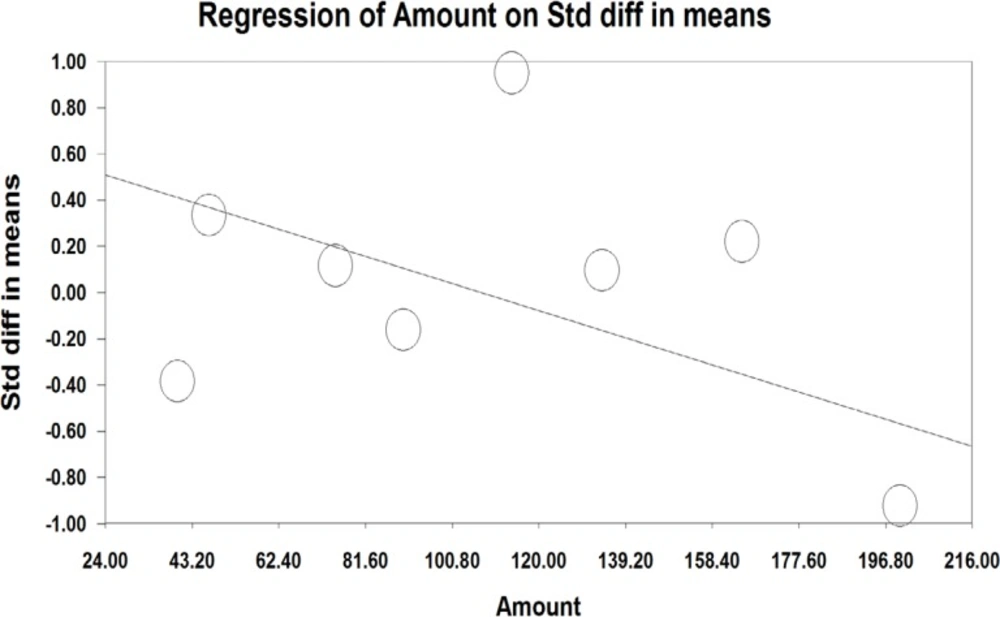
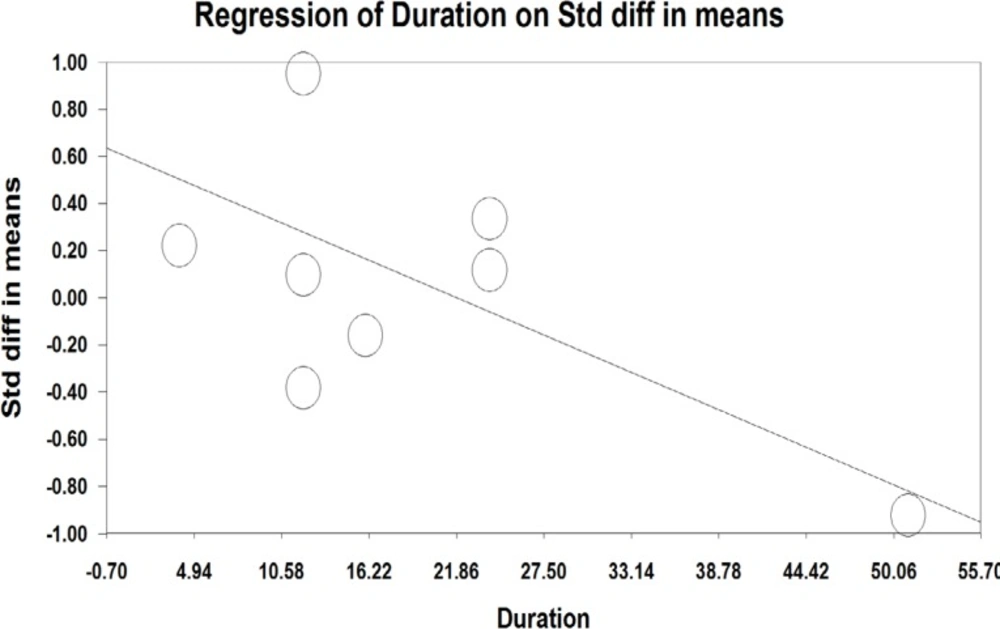
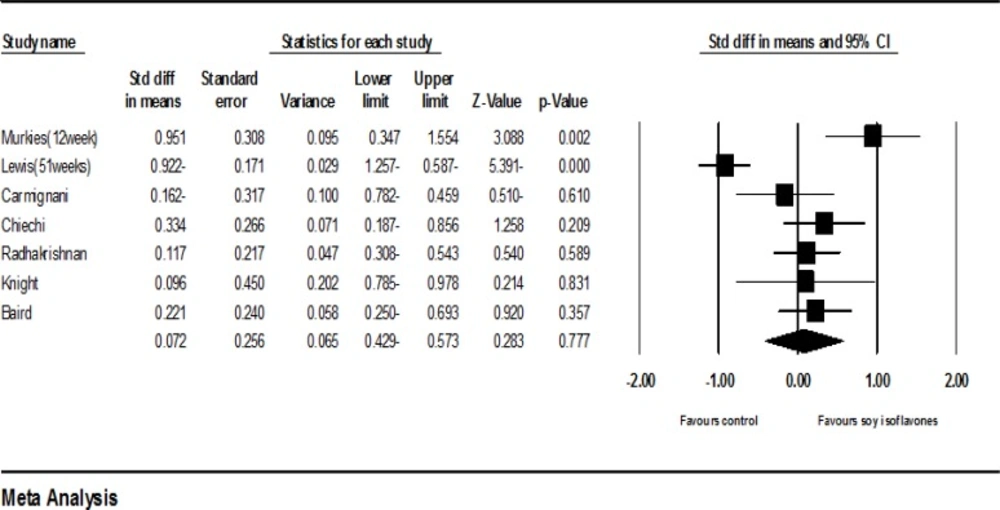
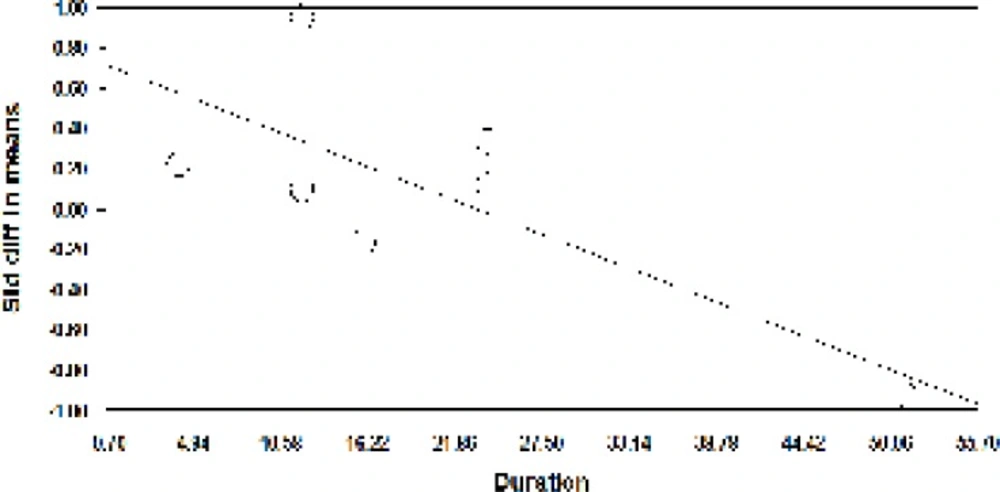
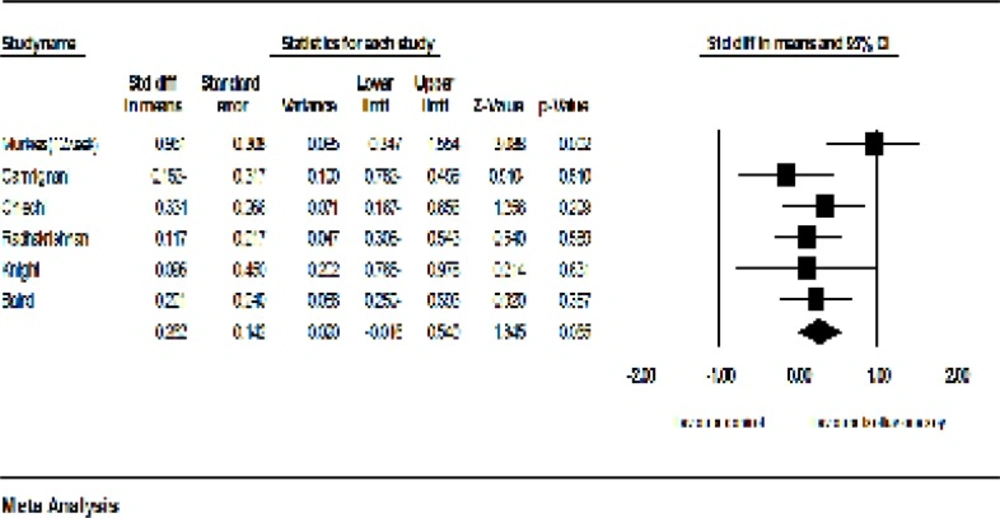
Furthermore, the results of the meta-analysis are graphically displayed in the forest plot. To assess the presence (or absence) of heterogeneity, the Cochran’s Q value was calculated, and P <0.05 was considered significant. The I2 index was also used to determine the amount of heterogeneity. If there was significant heterogeneity, the sensitivity analysis, meta-regression, and sub-group analysis were used as a standard way to investigate the causes of this heterogeneity.
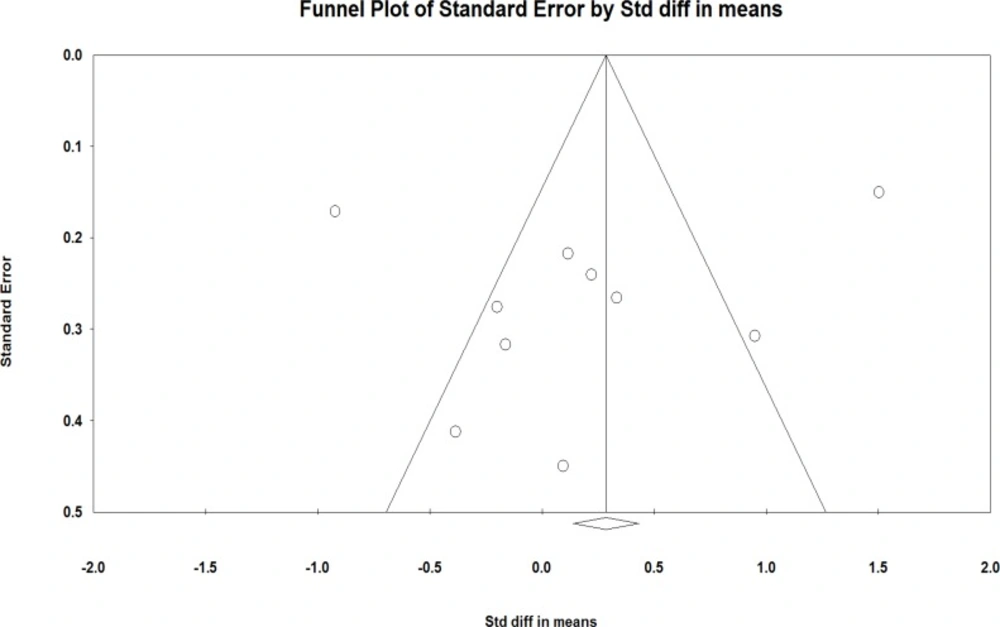
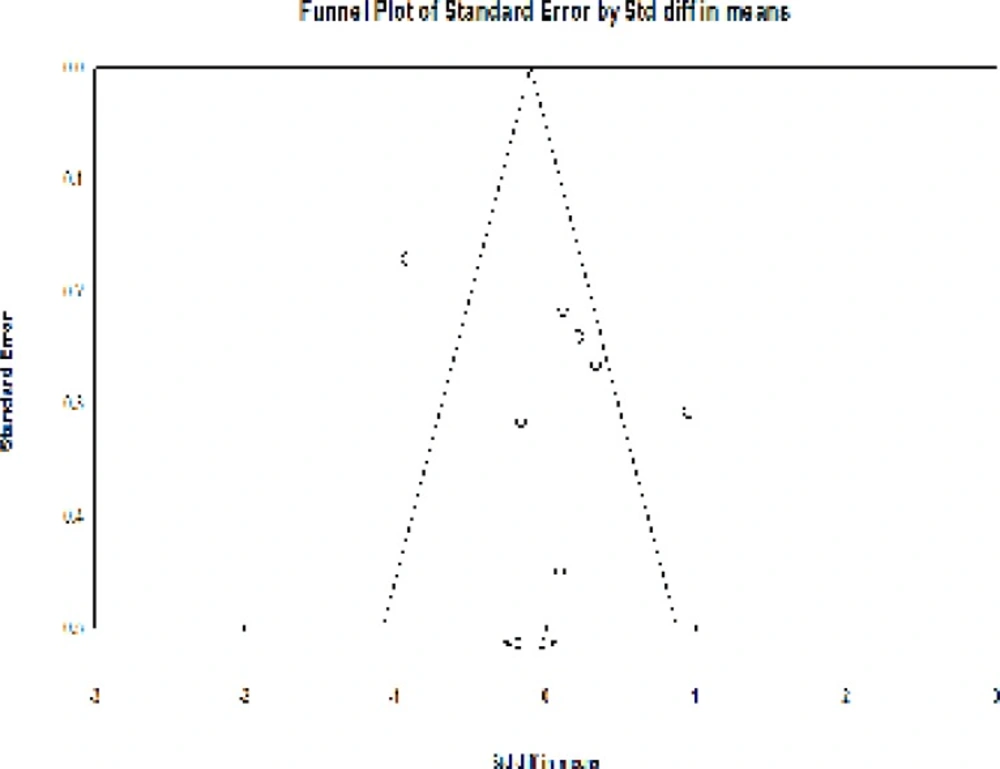
For each analysis, the publication bias was detected using the funnel plot and Egger’s regression intercept tests.