
Introduction
| RIFLE criteria | ||
|---|---|---|
| Serum creatinine (S Cr) criteria | Urine output (UO) criteria | |
| Risk | ↑ S Cr × 1.5 | < 0.5 mL/Kg/h × 6 h |
| Injury | ↑ S Cr × 2 | < 0.5 mL/Kg/h × 12 h |
| Failure | ↑ S Cr × 3 | < 0.3 mL/Kg/h × 24 h or anuria × 12 h |
| Loss | Complete loss of renel function > 4 weeks | |
| End stage | End stage renal disease for > 3 month | |
| Groups | High dose group | Conventional dose group | P-value |
|---|---|---|---|
| Variable | |||
| Age (mean ± sd) | 60.95(12.77) | 57.8(21.85) | 0.58 |
| Male (%) | 12(60) | 15(75) | 0.50 |
| APACHE II score on the first day (mean ± sd) | 18.5(5.88) | 17.35(6.11) | 0.55 |
| Site of infection | 0.29 | ||
| Lung (%) | 14(70) | 14(70) | |
| Blood (%) | 4(20) | 6(30) | |
| CNS (%) | 2(10) | 0 | |
| Pathogen type | 0.61 | ||
| Acinetobacterbaumannii(%) | 18 (90) | 17(85) | |
| Pseudomonas aeruginosa (%) | 0 | 2(10) | |
| Klebsiella pneumonia (%) | 2(10) | 1(5) | |
| Baseline serum creatinine level (mean ± sd) | 0.9(0.2) | 0.89(0.17) | 0.86 |
| Baseline serum cystatin C level (mean ± sd) | 1.1 (0.44) | 0.9 (0.32) | 0.11 |
| Concomitant nephrotoxic drugs (mean ± sd) | 0.8 (0.7) | 0.65 (0.49) | 0.60 |
| Concomitant nephroprotective drugs (mean ± sd) | 0.85 (0.49) | 0.9 (0.85) | 0.93 |
| No AKI | AKI | P-value | |||
|---|---|---|---|---|---|
| RIFLE | |||||
| Risk category | None | Risk | Injury | Failure | |
| Study group | |||||
| High dose group | 8 | 3 | 7 | 2 | 0.01 |
| Conventional dose group | 17 | 2 | 1 | 0 | |
: Repeated measure Test.
: Repeated measurestest, comparing differences.
: Independent sample t- test
: Repeated measure test.
: Repeated measure test, comparing difference.
: Independent sample t- test
: Repeated measure test.
: Repeated measure test, comparing difference.
Independent sample t- test
: Repeated measure test.
: Repeated measure test, comparing difference.
: Independent sample t- test
Study CONSORT
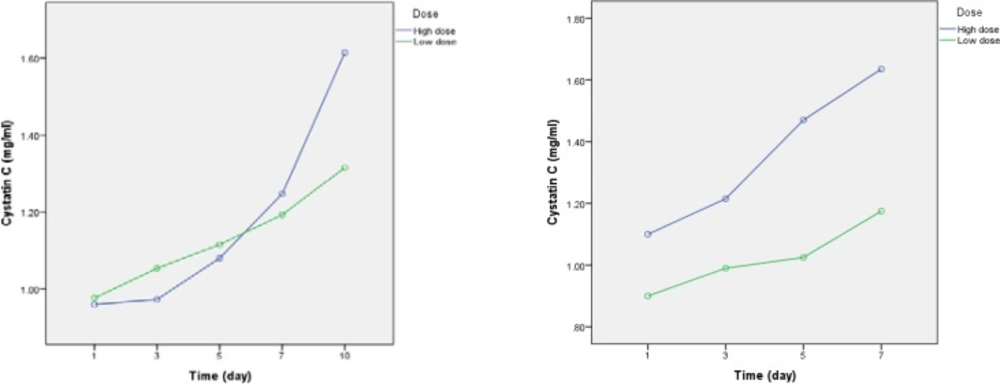
Serum Cystatin C level changes during studyperiod in high dose and conventional dose groups.a)Serum Cystatin C level changesuntill day 10. b) Serum Cystatin C level changesuntill day 7
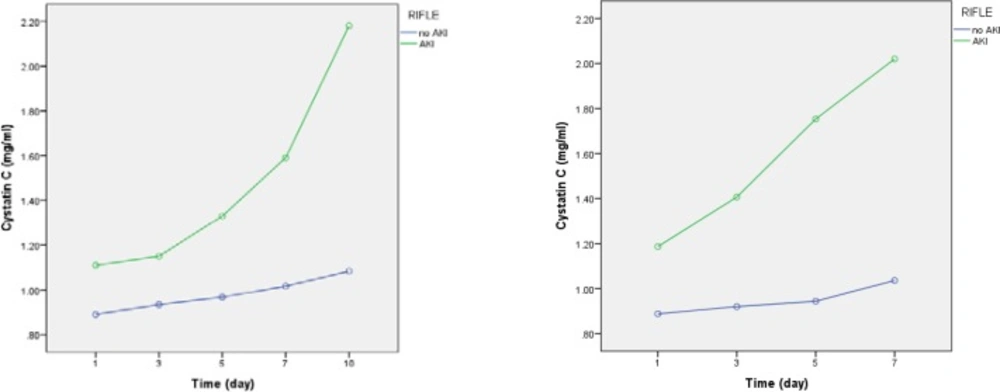
Serum Cystatin C level changes during study period in AKI and non- AKI groups.a)Serum Cystatin C level changesuntill day 10. b) Serum Cystatin C level changes untill day 7.
