Materials
MTH was purchased from Apollo Health Care Ltd., China. PEO (Polyox WSR 301) and HPMC (Methocel K100M premium DC grade) were generous gift samples from Colorcon Asia Pacific Pvt. Ltd, Singapore. Sodium starch glycolate (SSG), talc, magnesium stearate, sodium bicarbonate, polyvinyl pyrrolidone (PVP K30), isopropyl alcohol, dicalcium phosphate (DCP) were purchased from Fisher Scientific UK limited, UK. Other reagents utilized for the present study were of analytical grade. Active drug and excipients used for tablet formulation were received together with the certificates of analysis (COA) from the manufacturers. All necessary information on various physicochemical properties of the product was evident on the COA.
Preformulation parameters
Determination of various important preformulation attributes such as angle of repose, bulk density, tapped density, Carr’s index and Hausner ratio are essential to determine the flow property and compression property of powder/granules prior to tablet compression. The detailed procedures of these attributes are in the following sections:
Bulk Density (BD)
Pre-weighed powder or granule sample was sieved through 18 mesh screen, poured into a 100 mL graduated cylinder, and its volume was recorded. The same procedure was repeated three times, and the readings were averaged. Bulk density was calculated according to equation 1 and expressed in gm/mL.
Tapped density (TD)
A pre-weighed powder sample or granule was put in a 100 ml graduated cylinder and fixed onto tap densitometer (JV 1000, Copley). The apparatus was run for a time until it achieved a constant volume (tapped volume). Tapped density was determined according to equation 2 and expressed in gm/mL.
Compressibility Index (CI)
CI is used to predict flowability of powder blend prior to compression. It was calculated according to equation 3:
Angle of repose
Powder or granule flow property at preformulation stage can be determined by this simple and quick test. Cone forming method with fixed base was applied to determine the angle of repose. Powder sample or granule, devoid of any aggregation, was poured from a fixed height of about 10 cm to a fixed base (r) through a funnel supported by stand to form a symmetrical cone of powder mass. The height of the powder mass (h) was measured in triplicate to calculate the angle of repose (Ɵ) according to equation 4.
Drug-excipient compatibility studies
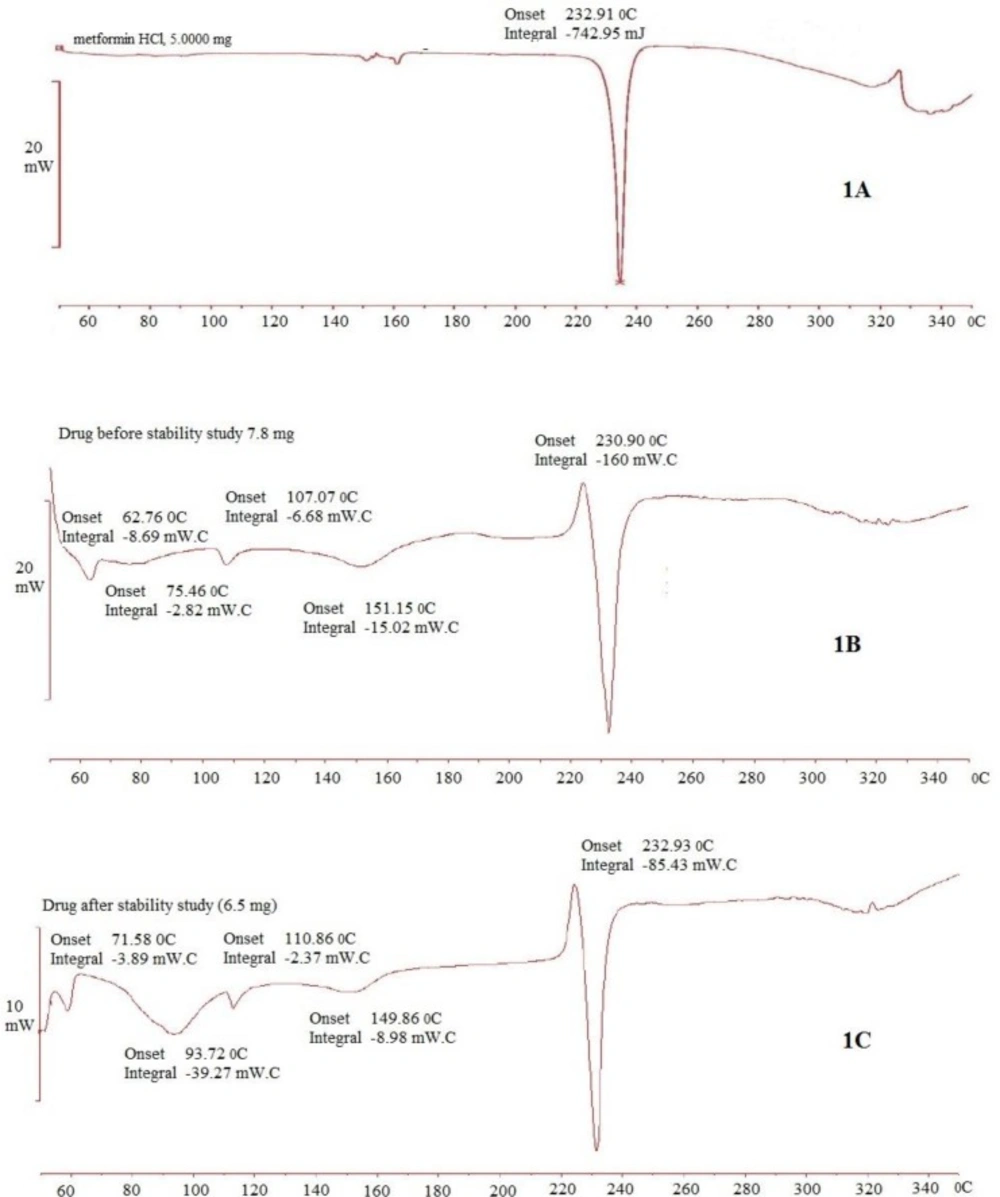
Differential Scanning Calorimetry (DSC) study was performed to determine drug-excipient compatibility. Pure sample of drug and excipients individually and their physical mixtures as per formulation composition were run on DSC apparatus (Mettler Toledo DSC821e, Switzerland). A sample of approximately 10 mg was passed through 60-mesh sieve and loaded in the pierced DSC aluminium pan. The sample was scanned within a temperature range of 50 to 300˚C with a heating rate of 10˚C/min with an inert atmosphere of dry nitrogen. Obtained DSC thermograms were analyzed to confirm any drug-excipient compatibility (
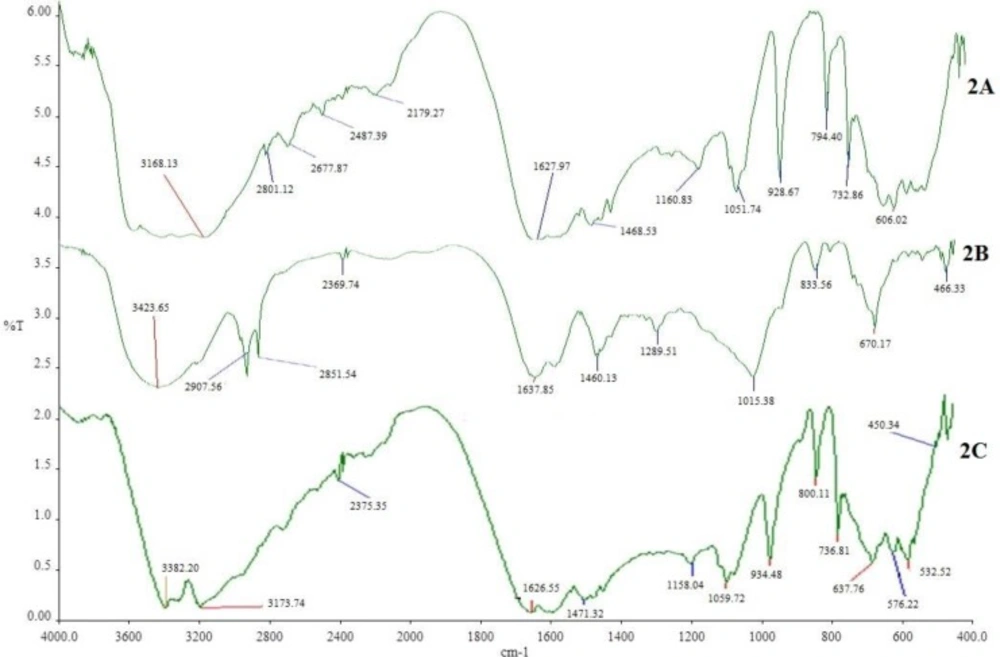
31). Apart from DSC, the pure drug and excipients, and their physical mixtures were analyzed by an IR spectrophotometer (Schimadzu IR–Prestige21) within a range of 4000-400 cm
-1.
Fabrication of MTH floating tablets
Sustained-release floating tablets of MTH were fabricated by wet granulation method with the ingredients listed in
Table 1. MTH and excipients excluding magnesium stearate and talc were passed through the sieve no.60. Accurately weighed quantities of MTH, HPMC, Polyox, NaHCO
3, SSG and DCP were mixed geometrically for 10 min to ensure uniform mixing of all the components. Dry powder blends were subjected to granulation by PVPK30 solution in isopropyl alcohol (IPA). Granules were dried at 45-50˚C in a hot air oven (Universal oven UM 400/Memmert) to a moisture content of 2 to 3%. The dried granules were passed through a sieve no 18 and lubricated with magnesium stearate and talc for further 2 min. Eventually gastro-retentive MTH tablets were fabricated from the final blend by a 10-station Rotary tablet press machine (Mini press II/Remek, Karnavati Engineering Ltd., India) using 12 mm circular, biconcave punches. All the tablets were stored in airtight containers for further study. Uniform thickness (5.7–5.9 mm) and hardness (165-171 N) were maintained for all produced tablets.
| Ingredient | Amount (mg) |
|---|
| Metformin HCl | 500 |
| Methocel K100M premium (HPMC) | 25 to 50 |
| Polyox WSR 301(PEO) | 100 to 200 |
| PVP K30 | 60 |
| Sodium starch glycolate (SSG) | 40 to 60 |
| Sodium bicarbonate | 40 to 60 |
| Talcum powder | 5 |
| Magnesium stearate | 5 |
| Dicalcium phosphate | qs to 950 |
Floating lag time and floating duration
Method reported by Tadros was utilized to measure floating lag time and duration of floating for the developed tablets (
32). One tablet was put in a 200 mL beaker containing 0.1 N HCl at 37˚C. Floating lag time was determined as the time taken for that tablet to reach to the surface, whereas duration of floating was measured visually as long as it maintained its floating in 0.1 N HCl. The test was performed in three replicates, and the result was averaged.
In-vitro dissolution study
USP type I (basket method) dissolution testing apparatus (Copley/DIS 8000) was used to measure
in-vitro drug release profile of the developed sustained-release floating tablets (
27). Each basket was filled with 900 mL of 0.1 N HCl as the dissolution medium maintained at a temperature of 37 ± 0.5˚C. The entire test was conducted at 100 RPM. Samples of 5 mL were withdrawn from an individual basket at predetermined time intervals (1, 2, 4, 6, 8, 10 and 12 h) and equal volume of a freshly prepared dissolution medium was replaced immediately. After filtration (150 mm whatman filter paper) and appropriate dilution with dissolution medium, the test samples were analysed by UV-Spectrophotometer (Hitachi/UV-1900) at a wavelength of 232 nm. LOQ (lower limit of quantification) of UV-visible spectrophotometric method was found to be 1 μg/ml with a linear relationship between peak areas and MTH concentrations in the range of 1 to 12 μg/mL (r
2 = 0.9989, equation: y = 0.0851x + 0.0015). Inter-day precision values for the developed UV method also were found to be within the acceptable limit of ICH method validation guidelines.
Formulation optimization by Response Surface Methodology
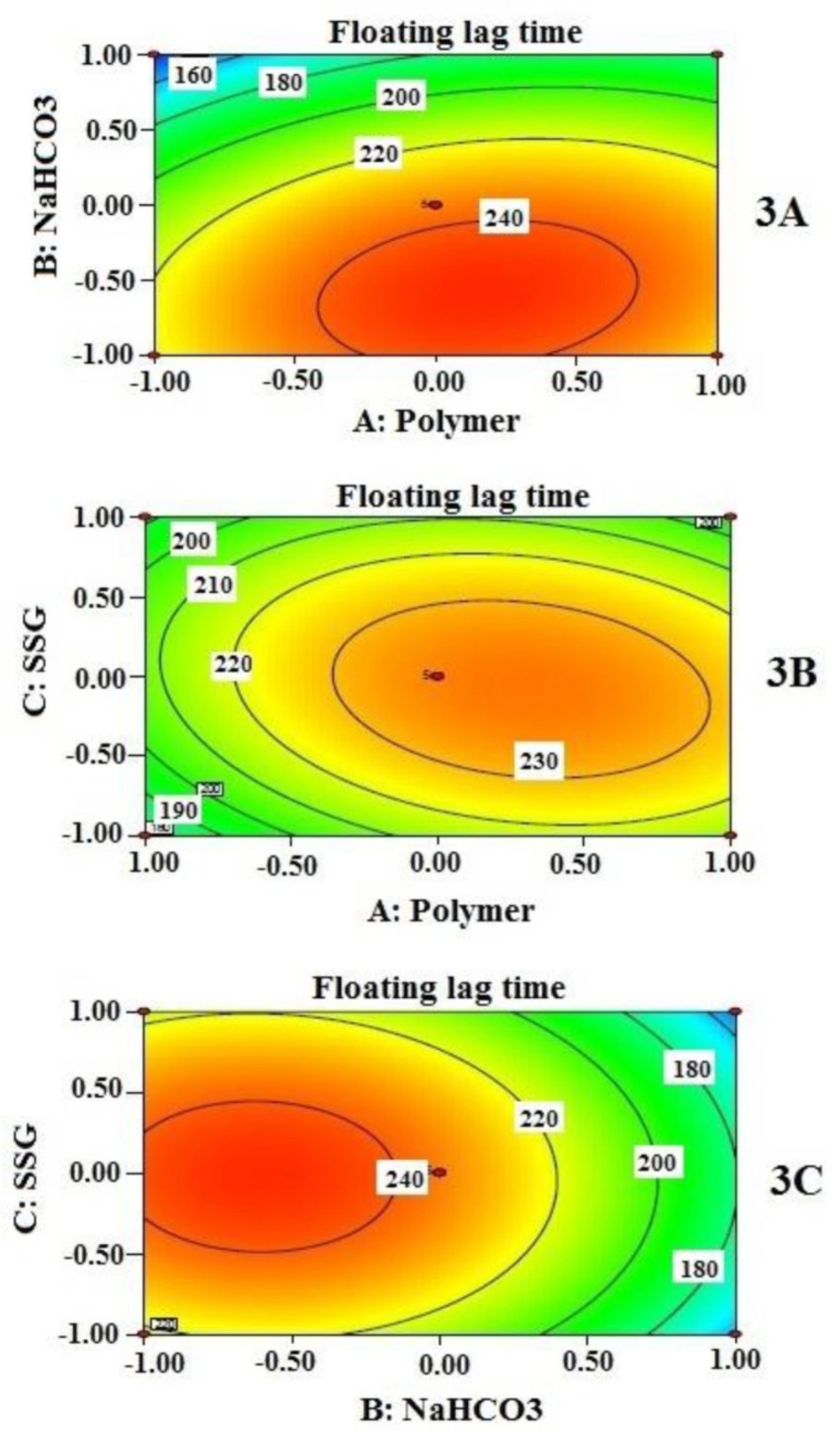
Response surface methodology (RSM) with 3 levels, 3 factors Box-Behnken design was applied to optimize the proposed formulation. Box-Behnken design was preferred as choice of experimental design considering its requirement of fewer numbers of experimental runs for three or four independent variables than full factorial design (
33). Concentration of hydrophilic swelling polymers, swelling enhancer and effervescent component have significant influence on floating lag time and drug release of a GRDDS as reported by several researchers (
29,
34). Therefore, the total amount of HPMC and PEO in the ratio of 1: 4 (A), SSG (B) and NaHCO
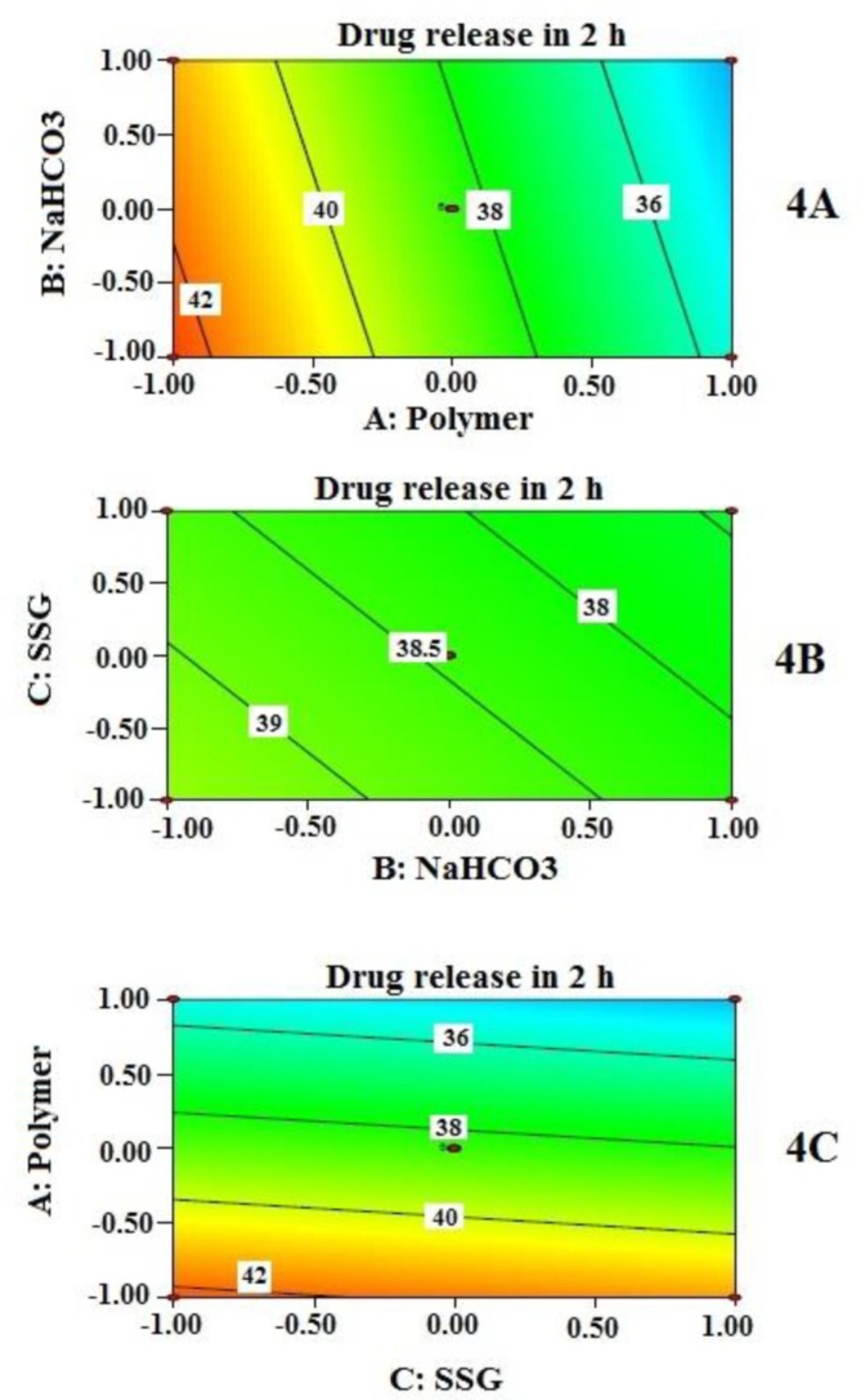
3 (C) were selected as independent variables considering their overall effects on the response variables such as floating lag time (Y
1), percentage drug released at 2 h (Y
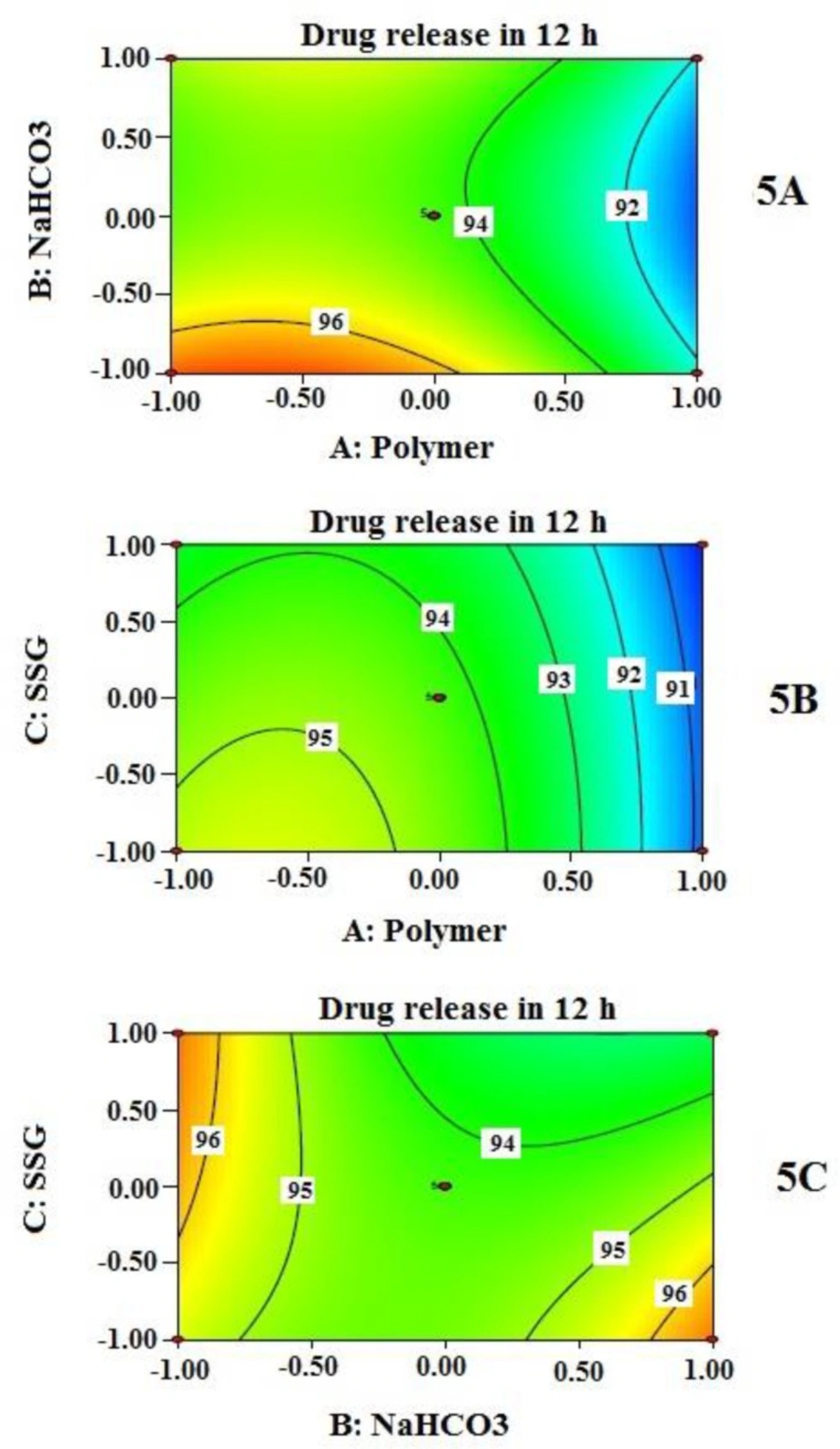
2), and 12 h (Y
3) (
Table 2).
| Independent variables | Levels of factors
|
|---|
| | +1 (High) | 0 (Medium) | -1 (Low) |
|---|
| A | HPMC: PEO (1:4) | 50:200 | 37.5:150 | 25:100 |
| B | NaHCO3 | 60 | 50 | 40 |
C
| SSG
| 60
| 50
| 40
|
Dependent variables
|
| Y1 = Floating lag time (sec)Y2 = Cumulative % drug release at 2 hY3 = Cumulative % drug release at 12 h |
Experimental trials originated from Box-Behnken design
The complete Box-Behnken experimental design consisted of 12 factor points and 5 replications at the center points; altogether, 17 experimental runs that are illustrated in
Table 3. Other composition and manufacturing conditions were kept constant for all experimental runs.
| Formulation code | Independent variables
| Dependent variables
|
|---|
| A | B | C | Y1 | Y2 | Y3 |
|---|
| F1 | 0 | +1 | -1 | 160 | 37.21 | 97.56 |
| F2 | 0 | 0 | 0 | 240 | 39.30 | 93.82 |
| F3 | 0 | 0 | 0 | 230 | 40.38 | 95.55 |
| F4 | 0 | 0 | 0 | 240 | 42.36 | 94.04 |
| F5 | +1 | 0 | -1 | 200 | 35.88 | 90.08 |
| F6 | 0 | -1 | -1 | 225 | 36.24 | 95.23 |
| F7 | -1 | 0 | -1 | 180 | 43.12 | 95.30 |
| F8 | +1 | 0 | +1 | 190 | 32.66 | 90.15 |
| F9 | 0 | 0 | 0 | 220 | 38.34 | 95.03 |
| F10 | +1 | -1 | 0 | 230 | 35.23 | 93.18 |
| F11 | -1 | -1 | 0 | 210 | 40.63 | 97.00 |
| F12 | -1 | +1 | 0 | 140 | 41.24 | 94.13 |
| F13 | 0 | -1 | +1 | 215 | 40.81 | 95.82 |
| F14 | +1 | +1 | 0 | 190 | 33.28 | 91.82 |
| F15 | -1 | 0 | +1 | 200 | 39.47 | 94.25 |
| F16 | 0 | +1 | +1 | 145 | 36.34 | 93.38 |
| F17 | 0 | 0 | 0 | 250 | 40.86 | 93.04 |
Data analysis and RSM model validation
RSM option of Design expert® software (version 8.0.7.1, stat-Ease Inc., Minneapolis, MN) was employed to perform optimization of developed sustained-release floating tablet of MTH composition. Multiple linear regression analysis (MLRA) option of the software allows to find statistically significant most appropriate linear and quadratic polynomial models containing individual (A, B, and C), interaction (AB, BC, and AC) and quadratic (A2, B2, and C2) terms. Mathematical forms of proposed linear and quadratic models are described by equation 5and equation 6 respectively.
Y = α0 + α1A + α2B + α3C (5)
Y = α0 + α1A + α2B + α3C + α12AB+ α13AC+ α23BC + α11A2 + α22B2 + α33C2 (6)
Where
Y is the model predicted response value consorted with all independent variables; α
0 is the constant value which is calculated from the arithmetic mean of experimentally obtained response variables of 17 experimental runs; α
1, α
2, α
3 are linear coefficients calculated from the experimentally obtained response values of
Y; α
12, α
13, α
23 are interaction coefficients of all three independent variables when considered any two of them at a time, whereas α
11, α
22, α
33 are quadratic coefficients of those independent variables (
35). Two dimensional (2-D) contour plots were generated for individual response variable in order to evaluate the effects of individual independent variables on individual response variable. Developed model was further validated based on experimental versus predicted values and their corresponding residual plot. Finally, the best formulation was selected from 17 trial formulations based on achieving optimum values set for the response variables.
Characterization of optimized gastro- retentive tablets
Tablets from optimized formulation were characterized for their routinely performed quality control (QC) parameters like uniformity of weight, thickness, hardness, friability, drug content, and percent of moisture content. Additionally, they were also tested for floating lag time, floating duration, and in-vitro drug release behavior.
Uniformity of weight
It is very important to maintain weight uniformity of tablets within a batch as well as among batches of the same weight. This test represents that all the tablets in a single batch are of same potency, within acceptable limits. Twenty tablets were selected at random, weighed individually and the average weight of the tablets was calculated from the total weight. Weight variation was calculated by comparing weight of individual tablet with the average weight (
36).
Hardness and thickness
Determination of hardness is required to assess the resistivity of tablets against mechanical shocks during their handling in manufacturing, packaging, and shipping operations. Tablet hardness is measured as compression force to break a tablet while applied diametrically. Tablet thickness, on the other hand, affects its packaging operation. Ten tablets were selected at random and measured for hardness and thickness simultaneously by using the Pharma test (PTB/411) hardness tester (
36). The average thickness with standard deviation was reported.
Friability
If the uncoated tablets are not strong enough to withstand mechanical shock subjected to coating, packing or transporting, they may undergo chipping, capping or breaking problem. This problem may arise if the tablet ingredients are not cohesive enough to bind them together. Friability test is performed just to assess that cohesive force.
Ten tablets were weighed, put into Roche friabilator (Sotax/CH 4123) and run for 4 min at 25 rpm. During each revolution the tablets were subjected to fall from a height of 6 inches. After completion tablets were cleaned to make them free from any adhered dust and reweighed. Friability was calculated by equation
7. The test was acceptable under the pharmacopoeal limit of less than 1% weight loss (
36).
Where, Wo is initial weight of tablet and
W is the final weight of tablet after the friability test
Drug content
To ensure uniform distribution of MTH within the developed tablets, drug content (assay) was verified. Twenty tablets were randomly selected, weighed and powdered with mortar and pestle. The quantity of powder equivalent to 100 mg of MTH was transferred carefully into a 100 mL volumetric flask and dissolved the drug within the powder with 0.1N HCl. Then the solution mixture was filtered and after an appropriate dilution, the filtrate was spectrophotometrically measured at 232 nm against 0.1 N HCl as blank. Drug content was estimated from the standard curve as mentioned in section 2.6.
Moisture Content
Moisture analyzer (Halogen moisture analyzer/HB43) was used to determine the moisture content of the fabricated tablets. Ten tablets were crushed, approximately 5 g powder sample was loaded in the pan and apparatus was run at 105ºC for 10 min. The result was recorded in triplicate.
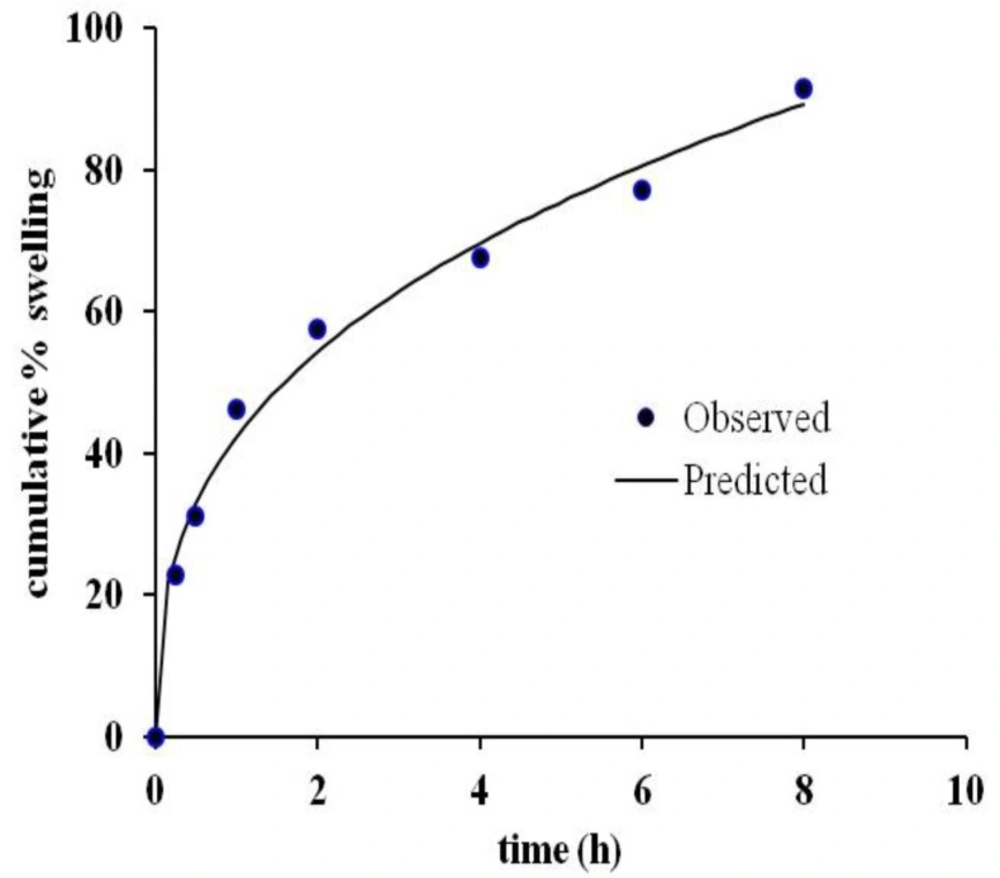
Cumulative % swelling
The swelling behavior of the tablet was measured by equilibrium weight gain method (
15). It was carried out in a dissolution apparatus (Copley/DIS 8000) without any stirring of the dissolution medium. Pre-weighed tablets (W
0) were placed in the basket containing 900 ml 0.1N HCl dissolution medium maintained at 37 ± 0.5˚C. The swollen tablets were taken out from the dissolution basket at predetermined time intervals t (0, 0.25, 0.5, 1, 2, 4, 6, 8 and 12 h). At each time point (t), tablets were taken out of the dissolution basket; excess water adhered to the swollen surface was soaked with tissue paper immediately and weighed on the analytical balance (W
t) (Mettler Toledo, AB125-S/FACT). The experiment was performed in three replicates. Cumulative % swelling was calculated by using equation
8.
Drug release kinetics
The
in-vitro drug release data from tablets of optimized formulation were applied to zero-order (
37), first-order (
38), Higuchi (
39), Hixon-Crowell (
40), and Weibull (
41), and Korsemeyer and Peppas model (
42) model to find out the drug release kinetic.
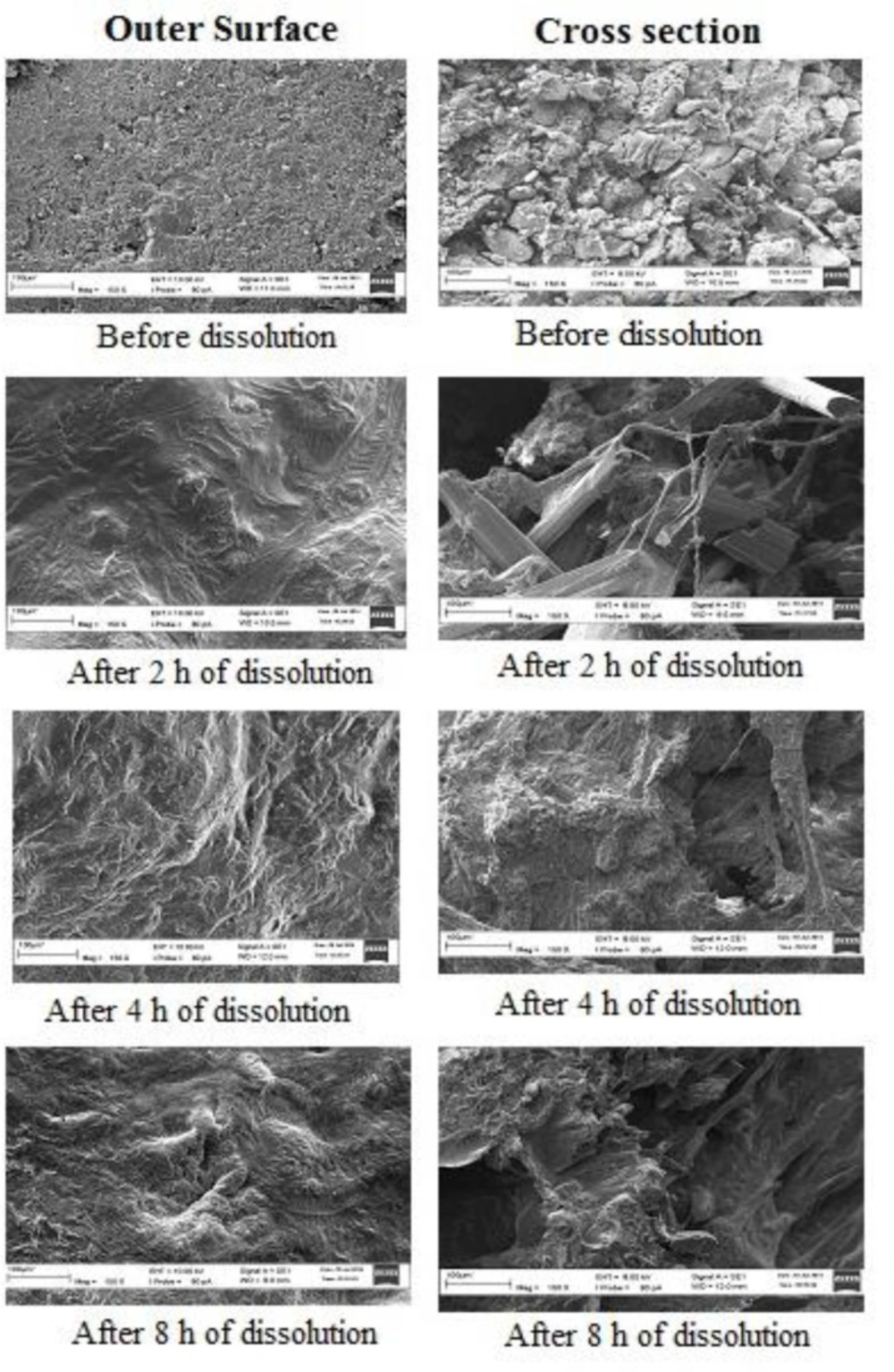
Scanning electron microscopy (SEM)
SEM study provides valuable information to confirm in-vitro drug release and floating mechanism of a GRDDS. During dissolution study, samples were taken in the different time interval (0, 2, 4 and 8 h) and blotted to remove excess water. Then they were dried in an oven (Universal Oven (UM 400/Memmert)). After that the samples were gold coated with Cool Sputter Coater (Leica EM SCD005), and viewed under Carl Zeiss scanning electron microscope (EVO series) at an accelerating voltage of 8 to 10 Kv.
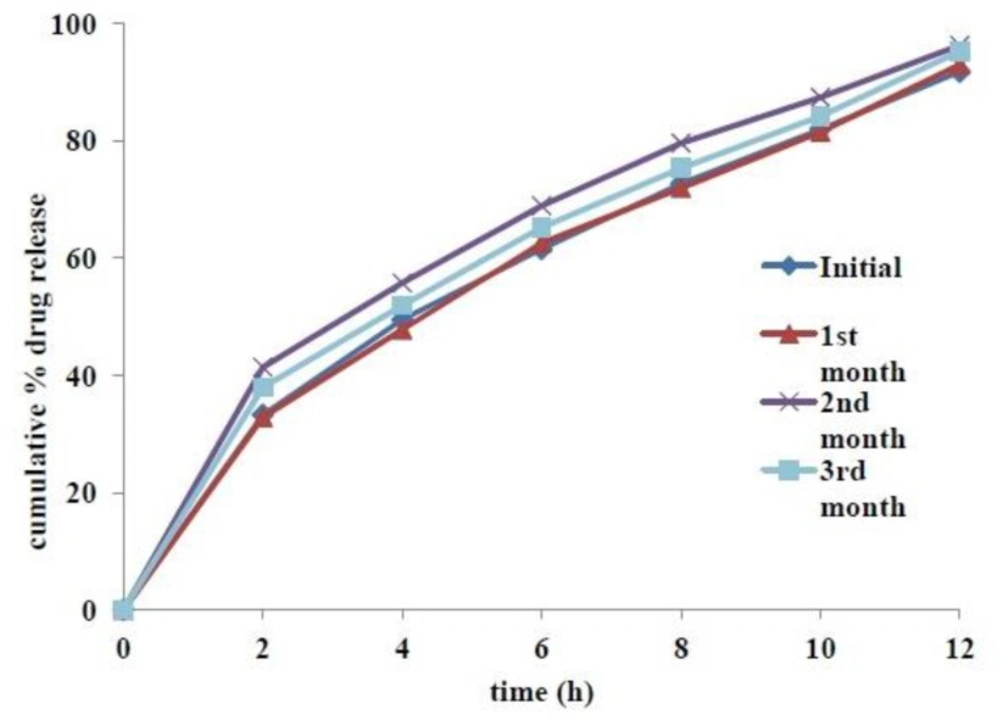
Accelerated stability study
The tablets from optimized formulation were tested for stability under accelerated storage condition (40˚C and 75%RH) for 3 months in accordance to ICH guidelines. The sampling was done at 0, 1, 2 and 3 months. Each time samples were evaluated for appearance, color, odor, size, hardness, friability, moisture content, drug content, in-vitro dissolution profile, and in-vitro buoyancy parameters such as floating lag time and duration of floating. All Results were compared against optimized formulation of 0 month as the reference.