
Introduction
Experimental
| Scoring parameter | Score definition |
| Inflammation severity | 0 (None) |
| 1 (Mild) | |
| 2 (Moderate) | |
| 3 (Severe) | |
| Inflammation extent | 0 (None) |
| 1 (Mucosa) | |
| 2 (Mucosa and submucosa) | |
| 3 (Transmural) | |
| 0 (None) | |
| Crypt damage | 1 (Basal 1/3 damaged) |
| 2 (Basal 2/3 damaged) | |
| 3 (Crypts lost, surface epithelium present) | |
| 4 (Crypts lost, surface epithelium lost) |
Results
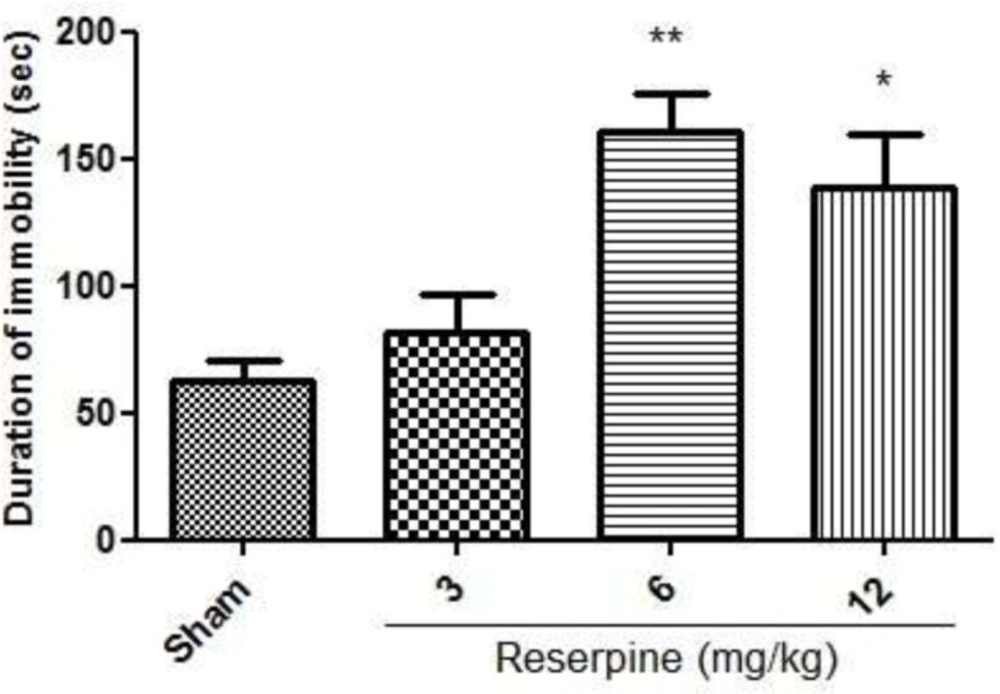
Effect of different doses of reserpine (3, 6, 12 mg/kg, i.p) in the rat forced swimming test; i.p. =intraperitoneally; Values are presented as mean ± S.E.M of six rats in each group; * P<0.05, ** P<0.01 compared to Sham, one-way ANOVA followed by Tukey test
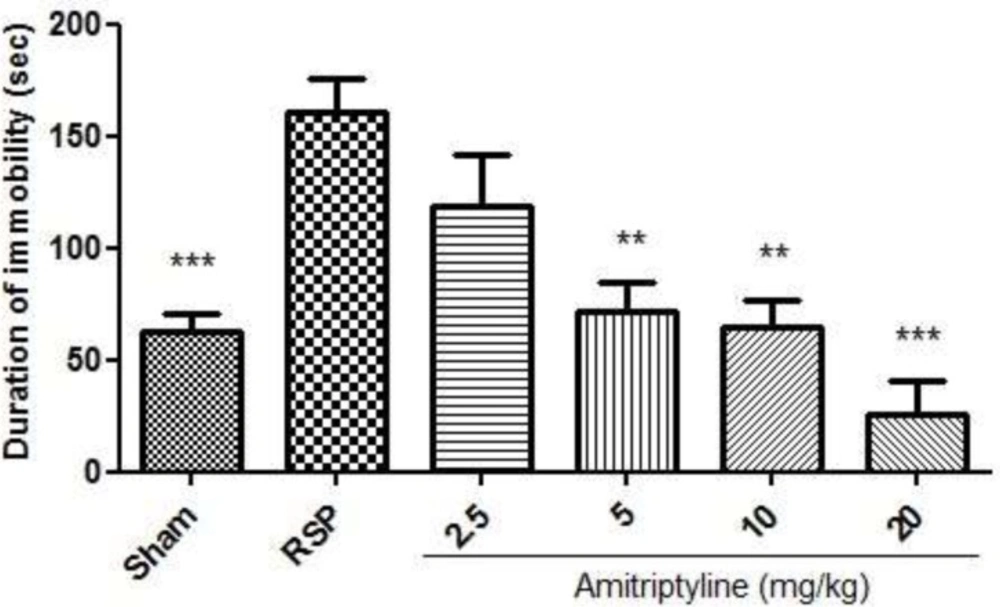
Effect of amitriptyline (2.5, 5, 10, 20 mg/kg, i.p.) on immobilization time (seconds) during forced swimming test in reserpinised (6 mg/kg) rats; i.p. =intraperitoneally, RSP= reserpine; Values are presented as mean ± S.E.M of six rats in each group; ** P< 0.01 and *** P< 0.001, compared to RSP, one-way ANOVA followed by Tukey test
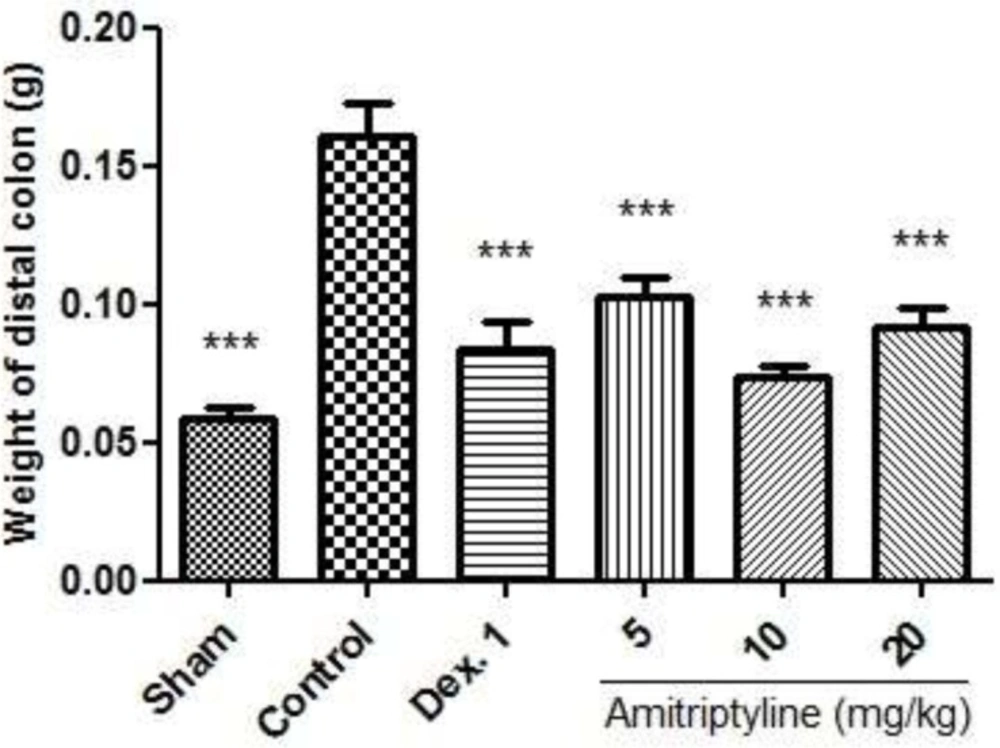
Effect of amitriptyline (5, 10, 20 mg/kg, i.p.) on weight of distal colon; i.p. = intraperitoneally, Dex. 1=dexamethasone (1 mg/kg); Values are presented as mean ± S.E.M of six rats in each group; *** P< 0.001 compared to control, one-way ANOVA followed by Tukey test
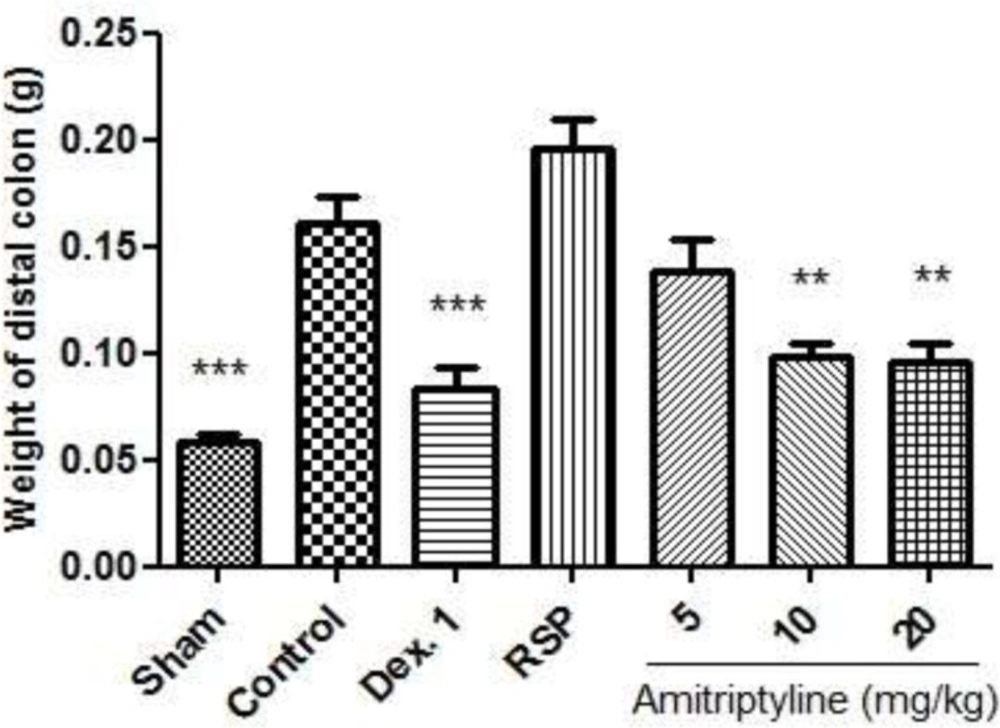
Effect of amitriptyline (5, 10, 20 mg/kg, i.p.) on weight of distal colon in reserpine (6mg/kg) induced depressed rats; i.p. =intraperitoneally, RSP= reserpine (6mg/kg), Dex.1 = dexamethasone (1mg/kg); Animals were also induced colitis; Values are presented as mean ± S.E.M of six rats in each group; ** P<0.01, *** P < 0.001 compared to control, one-way ANOVA followed by Tukey test
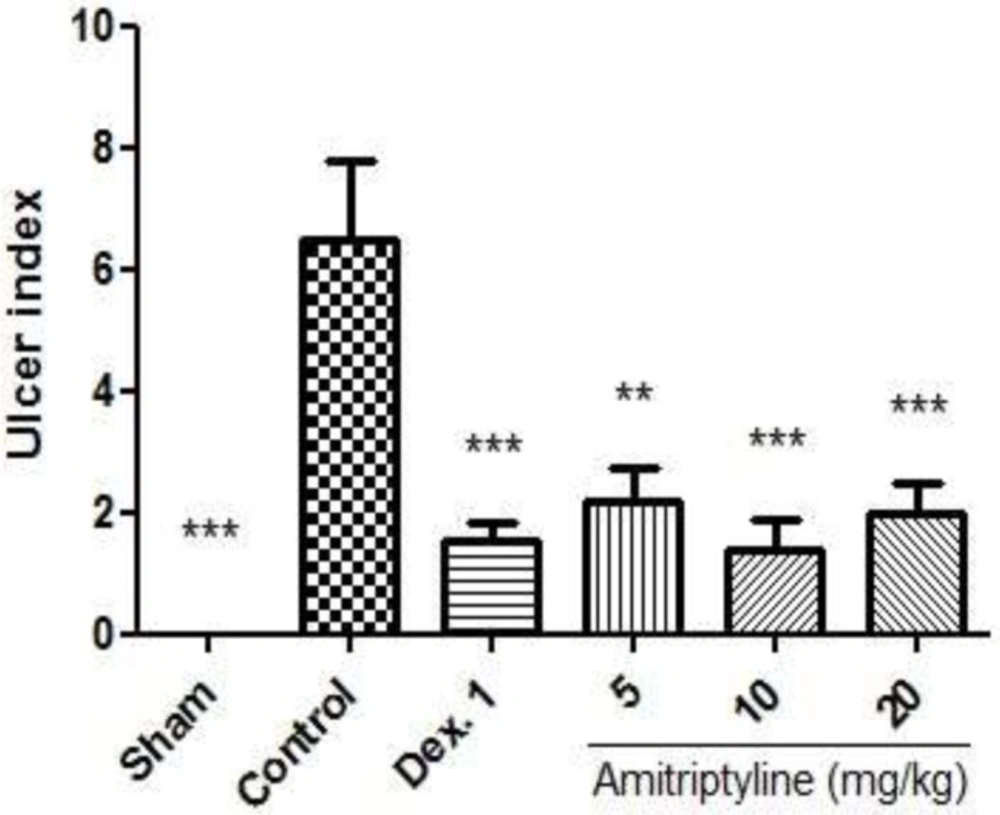
Effect of amitriptyline (5, 10, 20 mg/kg, i.p.) on ulcer index; i.p. =intraperitoneally, Dex. 1=dexamethasone (1mg/kg); Values are presented as mean ± S.E.M of six rats in each group; ** P < 0.01, *** P< 0.001 compared to control, one-way ANOVA followed by Tukey test
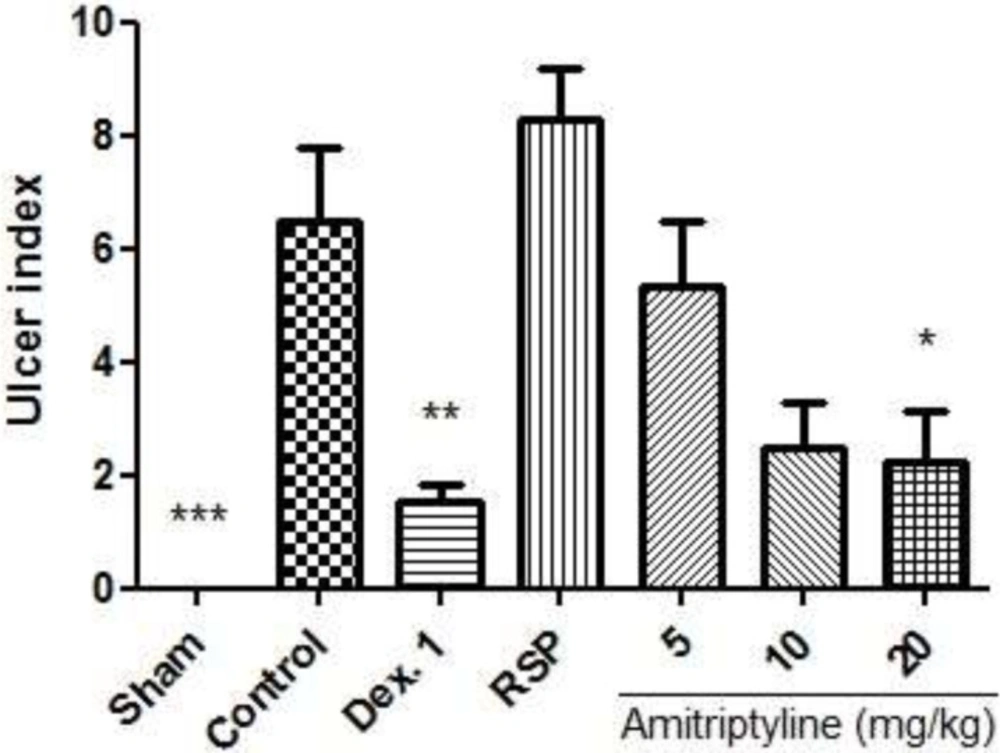
Effect of amitriptyline (5, 10, 20 mg/kg, i.p.) on ulcer index in reserpine induced (6mg/kg, i.p.) depressed rats; i.p. =intraperitoneally, RSP= reserpine (6mg/kg), Dex. 1 = dexamethasone (1mg/kg); Animals were also induced colitis; Values are presented as mean ± S.E.M of six rats in each group; * P<0.05, ** P<0.01 and *** P<0.001 compared to control, one-way ANOVA followed by Tukey test
| Group | Inflammation | Inflammation | Crypt Damage (0-4) | Total Colitis |
|---|---|---|---|---|
| Sham | 0 (0-0)** | 0 (0-0)** | 0 (0-0)** | 0 (0-0)** |
| Control | 3 (2-3) | 3 (2-3) | 4 (1-4) | 9.5 (6-10) |
| Dex. 1 | 0.5(0-1)** | 0 (0-2)** | 0 (0-2)** | 1 (0-5)** |
| AMT 5 | 2 (0-3) | 2 (0-3) | 2 (0-4) | 6.5 (0-9) |
| AMT 10 | 0.5 (0-1)** | 0.5 (0-2)** | 0 (0-1)** | 1 (0-4)** |
| AMT 20 | 1 (0-1)** | 1.5 (0-2)* | 0 (0-0)** | 2.5 (0-3)** |
P < 0.05,
P< 0.01 compared to control, Mann-Whitney U test.
| Group | Inflammation | Inflammation | Crypt Damage | Total Colitis Index (0-10) |
|---|---|---|---|---|
| Sham | 0 (0-0)** | 0 (0-0)** | 0 (0-0)** | 0 (0-0)** |
| Control | 3 (2-3) | 3 (2-3) | 4 (1-4) | 9.5 (6-10) |
| Dex.1 | 0.5(0-1)** | 0 (0-2)** | 0 (0-2)** | 1 (0-5)** |
| RSP | 3 (1-3) | 3 (1-3) | 4 (1-4) | 10 (4-10) |
| AMT 5 | 2.5 (1-3) | 2.5 (1-3) | 1.5 (0-4) | 6.5 (2-10) |
| AMT 10 | 1 (1-1)** | 1 (0-2)** | 0(0-0)** | 2 (1-3)** |
| AMT 20 | 0.5 (0-3)* | 0.5 (0-3)* | 0 (0-1)** | 1 (0-7)** |
P< 0.05,
P<0.01 compared to control, Kruskal–Wallis followed by Mann-Whitney U test.
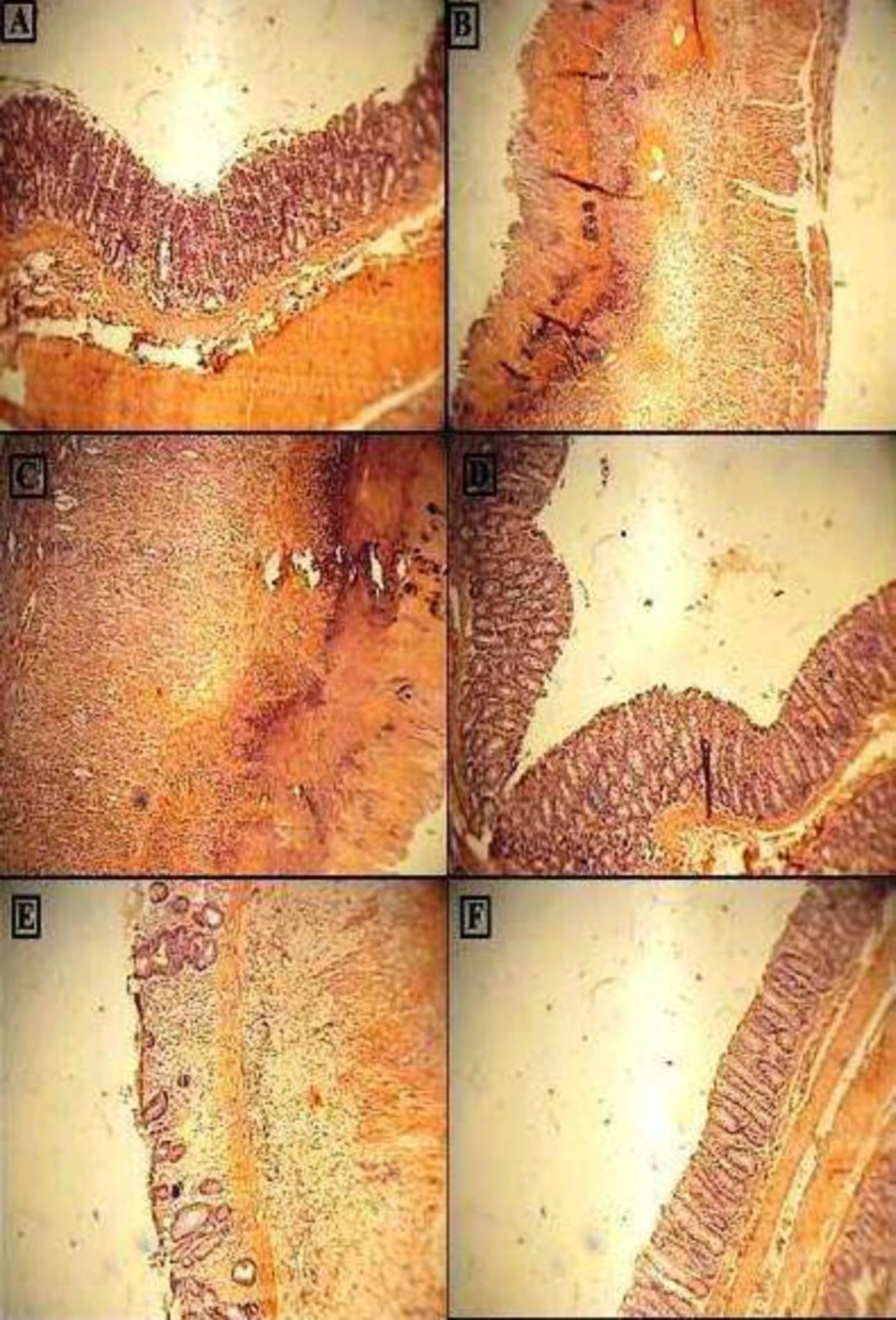
Photomicrographs of H&E stained paraffin sections of rat colonic tissues; (A) Normal intact mucosa from normal control animals showed intact epithelial surface. (B) Colitis induced by acetic acid in control group; Crypt damage, mucosal layers destruction and leukocyte infiltration are evident; (C) acetic acid-induced colitis in reserpine induced (6 mg/kg, i.p.) depressed rat showing massive necrotic destruction of epithelium; D, E and FColitis tissue treated with dexamethasone (1 mg/kg, i.p.), amitriptyline (10 mg/kg, i.p.), amitriptyline (20 mg/kg, i.p.) respectively, showing attenuated the extent and severity of the histological signs of cell damage;i.p. =intraperitoneally; Original Magnification×10
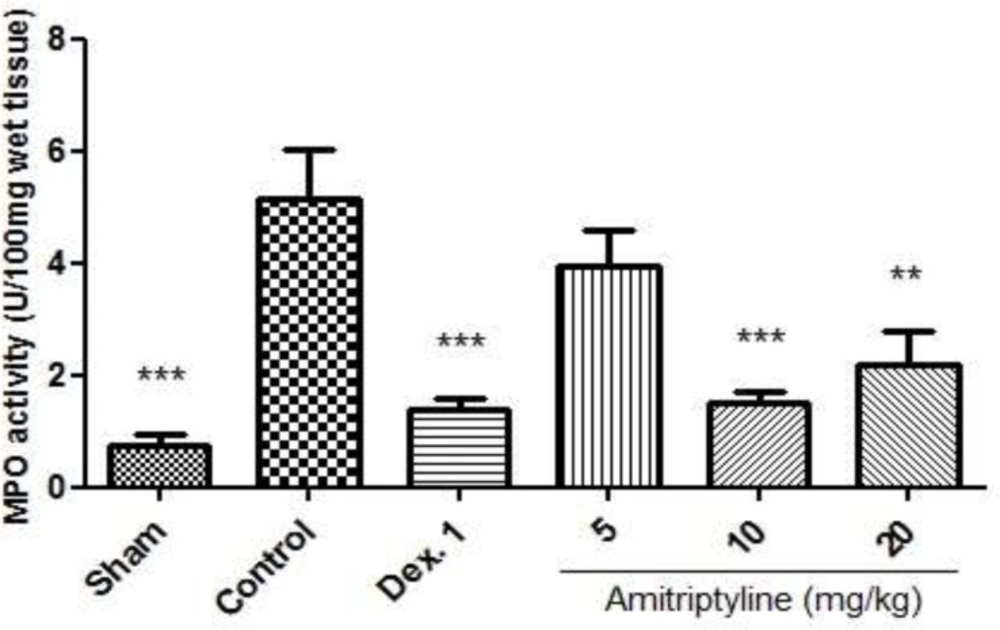
Effect of amitriptyline (5, 10, 20 mg/kg, i.p.) on myeloperoxidase (MPO) enzyme activity in the colonic tissue; i.p. =intraperitoneally, Dex.1=dexamethasone (1 mg/kg); Values are presented as mean ± S.E.M of six rats in each group; ** P<0.01, *** P<0.001 compared to control, one-way ANOVA followed by Tukey test
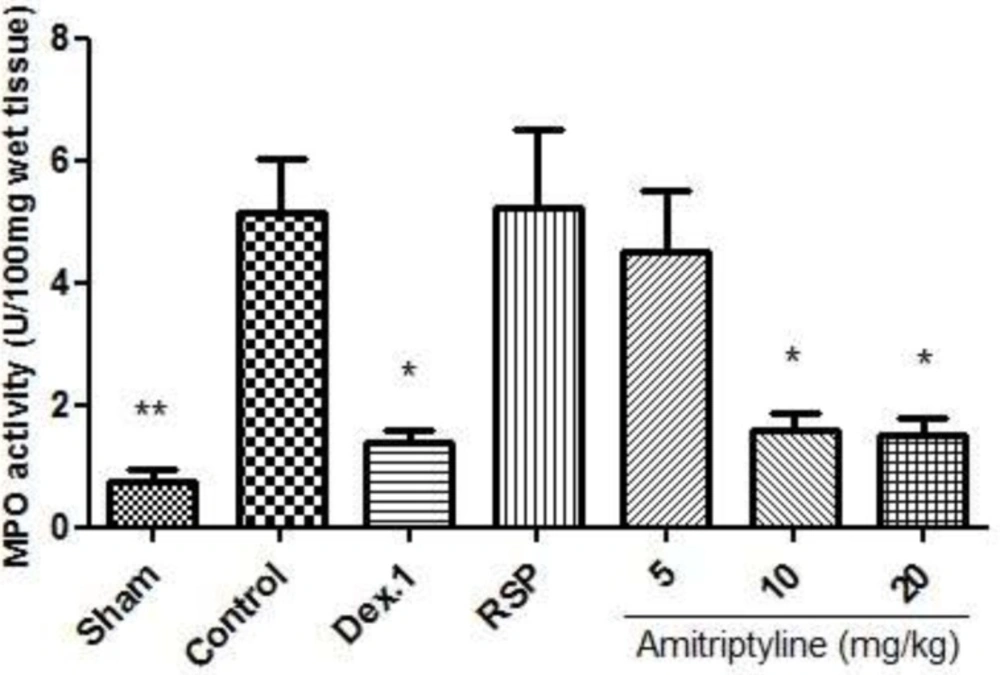
Effect of amitriptyline (5, 10, 20 mg/kg, i.p.) on myeloperoxidase (MPO) enzyme activity in the colonic tissue; Animals were reserpine induced (6 mg/kg) depressed and colitis was also induced; i.p. =intraperitoneally, RSP= reserpine, Dex.1=dexamethasone (1 mg/kg); Values are presented as mean ± S.E.M of six rats in each group; * P<0.05 compared to control, one-way ANOVA followed by Tukey test



