
Introduction
Labor pain is one of the most tiresome types of pain and human has been seeking to allay this pain at all time. In addition to suffering mothers both physically and psychologically, severe labor pain can cause prolonged labor and dystocia which are hazardous for either mother or fetus. This occurs due to releasing catecholamines which in turn impact on labor progression because of maternal anxiety during an intolerable pain (1, 2). In addition, severe labor pain can lead to excessive maternal exhaustion and impaired pushing ability during delivery (3). Therefore, administration of a suitable analgesic agent during labor is very beneficial for childbirth outcomes (2).
Nowadays, various methods are applied for pain relief such as injectable opioids, regional anesthesia and inhalational analgesics (4, 5). Although using gas inhalation is widespread in Asian and European maternity care centers, application of regional anesthesia is more prevalent in America. Of course the option of using nitrous oxide to relieve pain has been more acceptable recently, it is limited by its lack of availability in America (2, 6).
English scientist, Joseph Priestly, was the first one who experienced N2O for pain relief during labor in 1772. Years later, Minitti invented a machine to mix N2O and O2, in 1933. Finally, Entonox (50% of N2O and 50% of O2), compacted in cylindrical containers, was offered commercially by an English company in 1961 (6, 7). Analgesic effect of Entonox is thought to be an increased release of endogen opioids that its euphoric and anxiolytic effects are through stimulation of gama-aminobutyric acid receptors in brain (6, 7). Advantages of Entonox, such as being non-inflammable, odorless, colorless, tasteless, rapid onset and offset of effect have made it a desirable method for pain relief of labor. Its lower cost and less invasive nature are its other benefits (6). In addition, its filtration is totally in lungs, which makes it useable in hepatic and renal diseases (7-8). Entonox disadvantages include drowsiness, dizziness, mouth drying, nausea, vomiting, tingling and muscular spasm, which usually disappear a few minutes after discontinuation of the gas (7-9).
Entonox is used by the mother herself through putting on a face mask at the beginning of the active phase of labor and can be administered in two ways: intermittently or continuously (10). In the intermittent method, the mother breathes in the mask during uterine contractions and puts it aside at the end of pain, whereas in the continuous method, she uninterruptedly breathes in the mask (6, 8).
As it takes at least 30-50s for gas to be mixed with blood, in the intermittent method, gas inhalation should be performed at least 30s before beginning of the contraction to receive the maximum analgesic effect (7, 10, 11). Sometimes, it is difficult for mothers to do this synchronization exactly, so some women would rather the continuous method than the intermittent one.
From 1961 till now, the intermittent method has been used worldwide prevalently in maternity care centers. Avoiding of maternal side effects, such as drowsiness and dizziness, is the most important causes of using this method (7, 10, 11). It seems that there have not been enough clinical trials comparing both methods yet. Rosen et al (1981) in a comparative study with two methods showed a high maternal satisfaction rate by using continuous method. Also midwives declared more simplicity in training this method (13). Since it seems many mothers desire to use Entonox continuously for more painless perception and easier usage, we intended to conduct a comparative study of continuously vs. intermittently use of Entonox during active phase of labor. The aim was to demonstrate whether continuous method is as safe as intermittent, and can midwives set the mothers free to choose the optional method.
Experimental
Materials and methods
This randomized clinical trial was conducted in Sabzevar Mobini hospital in 2013, and after the approval of the ethics committee of Sabzevar Medical University and obtaining the informed consent forms, a total of 100 women admitted for vaginal delivery, were enrolled in the study. This number of sampling was determined by confidence coefficient of 95%. The inclusion criteria were singleton pregnancy, cephalic presentation, and term gestation. The exclusion criteria were macrosomia, contracted pelvis of mother, repeated cesarean section, insecure fetal heart rate (FHR), spo2 less than 95% and contraindications of Entonox usage including head injury, severe asthma, inability and unwillingness of patients to use Entonox.
Experimental details
The mothers were divided into two groups by simple randomization, group A including 50 women received Entonox intermittently, group B containing 50 women that used Entonox continuously. Selection of patients was through simple choosing and they were settled in two groups by accidental allocation. Before participating in the study, a comprehensive interview was conducted with mothers and registered in the questionnaire. Training of mothers was done by a midwife (sampler). In group A, mothers were breathing in mask during uterine contractions and put it aside between them. In group B, mothers were using Entonox constantly. The gas inhalation was performed at the beginning of active phase (cervical dilatation 3-4 cm, and effacement 40-50%) and was terminated by full dilatation of cervix for two groups. All the mothers’ conditions influenced by gas were written in the study forms. Also contraction duration and fetal heart rate (FHR) were monitored and registered; also labor progression was assessed by partograph. Maternal o2 saturation was monitored with pulse oximetry. At the end of delivery, the mothers’ satisfaction was evaluated among the two groups. Data was analyzed by spss17, t-test and chi-square(X2). p-value <0.05 was considered significant statistically.
Results and Discussion
Our findings showed that demographic data and also obstetrics and fetal characteristics were matched in both groups (Table 1). The maternal side effects of Entonox had no significant differences in two groups (Figure 1). Spo2 was more than 95% in both groups and had no significant differences between two groups (p>0.05). Interestingly, Mothers’ satisfaction rate in continuous group was more than the intermittent group significantly (p<0.001) (Figure 2). Mothers’ cooperation during delivery in continuous group was more than intermittent group (p<0.05). Mean duration of active phase of labor was 142 and 172 minutes in continuous and in the intermittent group respectively that was not a significant difference (p=0.2). Fetal and maternal obstetrics outcomes were not different significantly in two groups (p>0.05).
Table 1Demographic characteristics of the participants
| p-value | Intermittent | continuous | Characteristics | |
|---|---|---|---|---|
| 0.8 | 24.8±5.7 | 24.7±4.0 | Age(mother) | |
| 0.2 | 30.3±5.9 | 28.9±4.7 | Age(husband) | |
| 0.3 | 24.8±3.0 | 24.2±2.9 | Body mass index(kg/m2) | |
| 0.5 | 66% | 60% | Primary(%) | Educational level(mother) |
| 16% | 14% | Secondary(%) | ||
| 18% | 26% | University(%) | ||
| 0.7 | 58% | 48% | Primary(%) | Educational level(husband) |
| 42% | 52% | Secondary(%) | ||
| 0.3 | 88% | 72% | less than 200 dollar | Annual household income |
| 12% | 28% | More than 200dollar | ||
| 0.3 | 58% | 54% | primipara(%) | Parity |
| 42% | 46% | multipara(%) | ||
| 0.2 | 40.9±1.7 | 40.3±1.2 | Gestation(wk) | |
| 0.06 | 3097.4±357.1 | 3245.4±436.9 | Birth weight | |
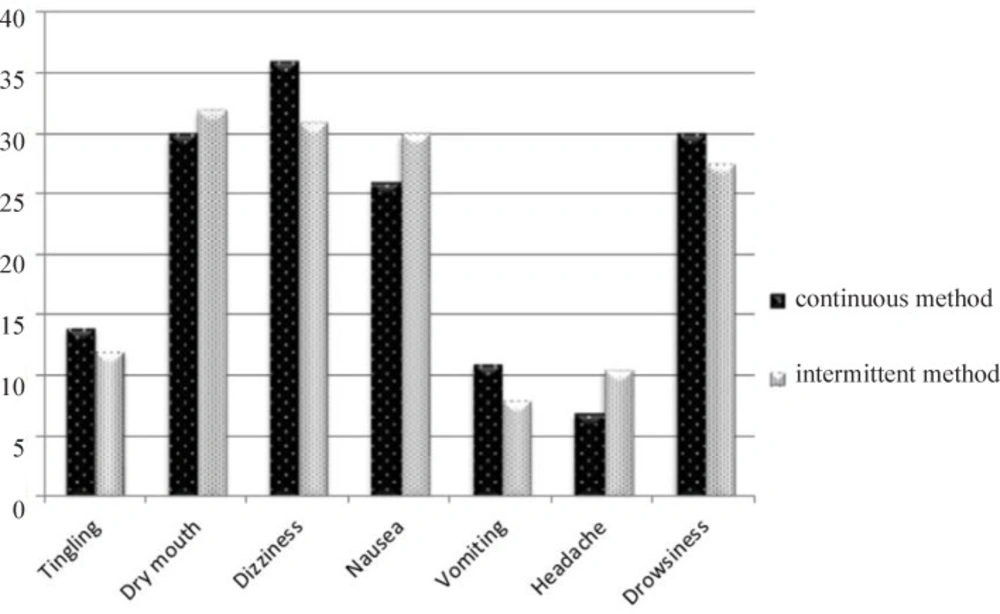
Figure 1
Comparison of maternal side effect in continuous vs. intermittent method of using Entonox
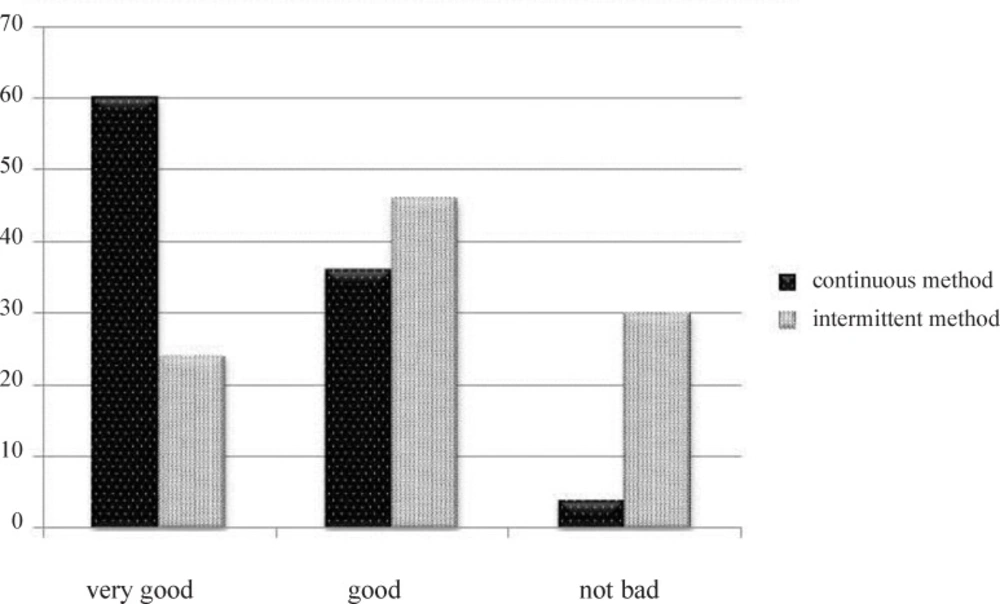
Figure 2
Comparison of maternal satisfaction rate in continuous vs. intermittent method of using Entonox
There is no doubt that relieving pain during labor is beneficial for obstetric outcomes. Severe pain can lead to prolonged labor and dystoscia and also increasing cesarean section (2, 14). Indeed, prolonged labor in addition to jeopardizing the fetus, increases maternal morbidity and mortality rates due to mothers’ exhaustion, postpartum hemorrhage and even uterine rupture (4).
Efficacy and safety of Entonox for this purpose have been proved for many years (7, 15-16). Because of fear of maternal adverse effects by continuous method, it has been customary to use Entonox intermittently for several decades (2, 7, 17).
Our study showed that nausea, dry mouth and headache were more in the intermittent method. In comparison to the intermittent method, dizziness, drowsiness, vomiting and tingling were more in continuous method. But there was no significant difference between two methods. Our data supports the findings of Rosen (1981) that showed this method is without demonstrable side effects (13). Also Tazarjani (2010) did not report any significant side effects by continuous method (18).
Most of the studies about maternal side effects of Entonox have been showed in the intermittent method, such as Jaffari et al. 2013 declared drowsiness (29%), dry mouth (25%), headache and dizziness (14%), nausea (8%) and vomiting (2%) (19); Donen et al. 2007 showed drowsiness (40%), dizziness (18%), nausea (5%) (20); Esfandiari et al. 2002 mentioned dizziness and headache (23%) (21); And Najafian et al. 2013 showed lethargy (40%), dry mouth (%31), vertigo and headache (20%), vomiting (11%) (22).
Cynthia et al. 2012 and Baysinger et al. 2013 mentioned that Entonox is mostly used intermittently, because drowsiness caused by continuous method; but our study showed that this complication was not so problematic to avoid recommending the continuous method to the mothers, especially regarding the more satisfaction rate in mothers that used it continuously (10, 12).
In our study, mothers’ satisfaction rate was (96%) in continuous method and (70%) in intermittent method, but in others’ studies this rate was (78%), (96%) and (42%) in intermittent group (20, 23, 24).
The more satisfaction rate in continuous vs. intermittent method was similar to Rosen’s results (1981) that showed continuous method had better acceptance and 96% of mothers wished to continue offering the continuous method (13).This result may be due to some reasons, including easier usage, more analgesic effect, less anxious status for mothers and shorter duration of active phase of labor by continuous method. Consequently, mothers had more cooperation during delivery obviously by continuous method.
Conclusion
In this study, the aim was to demonstrate the best way of Entonox usage in terms of facilitation, painless effects associated with acceptable safety and satisfaction. Generally, health staff are afraid of continuous method and remind mothers to put the mask aside between contractions repeatedly. This belief and action usually lead to anxiety and inconvenience both for mothers and midwives. It seems that by more investigations we can set the mothers free to choose the desired method of Entonox usage, intermittently or continuously.
This approach leads to reduction of difficult labor and cesarean section and consequently helps to improve the health level, both physically and psychologically.
