Animals were randomly divided into four groups (n = 18 in each group).The first group served as control and vehicle was given orally (p.o.); the other three groups were pretreated orally (p.o.) once daily (10-11.00 h), for 30 days with RHE (50, 75 and 100 mg/Kg body weight): doses identified using previously published data. 2 h after the last pretreatment, the rats subjected to 60 min of middle cerebral artery occlusion followed by 24 h of reperfusion. After 24 h reperfusion, neuro-behavioral studies, infarct volume (n = 6), water content (n = 6), and blood brain barrier permeability (n = 6) were measured. Additionally, 12 sham-operated animals underwent the same surgical procedures (without blocking the arteries).
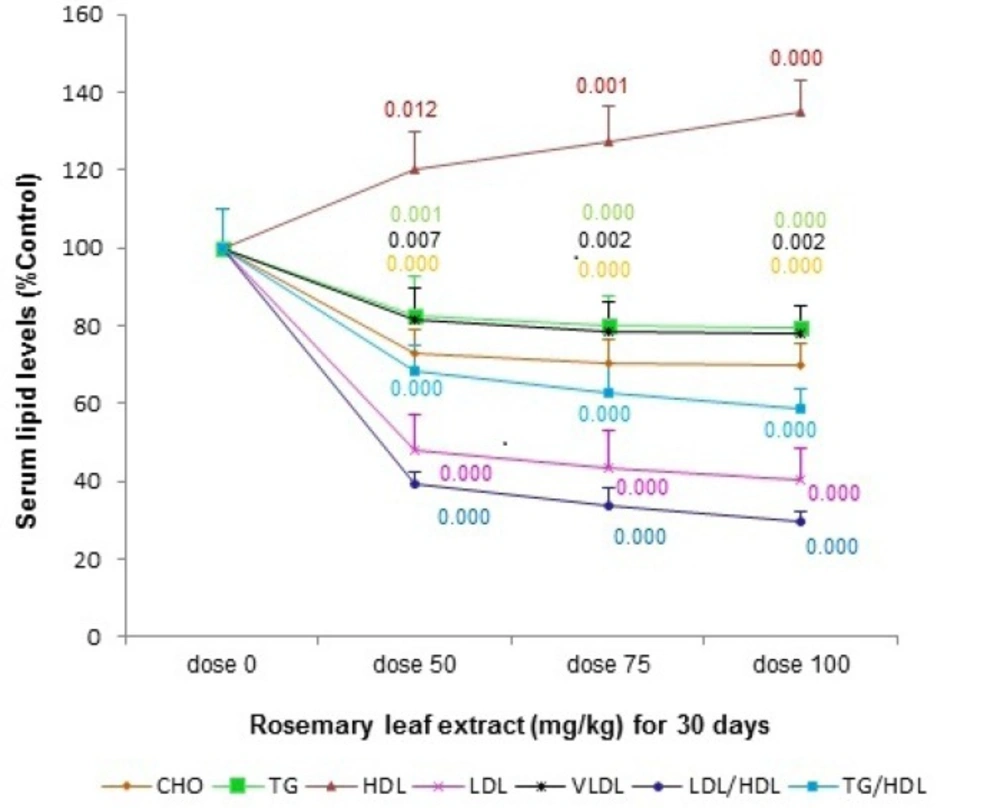
Lipid profiles
The rats were anesthetized with chloral hydrate (400 mg/Kg i.p.) at 30 days after the initiation of pretreatment, just before surgery. Then, blood samples were taken by tail vein. The blood samples were centrifuged at 7000 × g for 10 min, room temperature to obtain plasma.
The serum samples were stored at -20 °C until biochemical analysis. Levels of HDL, triglyceride, and cholesterol content (Pars Azmun, Iran according to manufacturer’s instructions) were measured using an autoanalyzer (Liasys, Roma, Italy).
Middle cerebral artery occlusion
The right middle cerebral artery (MCA) occlusion (MCAO) was induced using an intraluminal filament model (
21). The rats were anesthetized with chloral hydrate (Merck, Germany; 400 mg/kg i.p.). Briefly stating, neck vessels were exposed through a midline incision. Under an operating microscope, the right common carotid artery (CCA), the right external carotid artery (ECA), and the right internal carotid artery (ICA) were isolated. Then, a 3-0 silicone-coated nylon was carefully inserted from the external carotid artery into the internal carotid artery (ICA) until light resistance was felt. The filament was inserted approximately 20 mm from the carotid bifurcation to effectively block the middle cerebral artery (MCA). After 60 min of transient MCA occlusion (tMCAO), blood flow was restored by withdrawing the nylon filament and the ECA was permanently tied. During these procedures, body temperature was monitored with a rectal probe, and was maintained at 37±0.3 °C (Citizen-513w) using a heating pad. Animals were then recovered from anesthesia and were returned to their cages for 24 h. Sham animals were subjected to surgery with sutures of the same size but the suture was not advanced into the middle cerebral artery. The animals were kept at ambient temperature until sampling, with free access to water and food.
Neurological examination
Neurological function was evaluated using a 0-5 point scale neurological score (21) after 24 h of reperfusion: 0 = no neurological dysfunction; 1 = failure to extend opposite forepaw; 2 = circling to the contralateral side, when held by tail with feet on floor; 3 = falling to the left; 4 = unable to bear weight on affected side; 4 = no spontaneous walking and a depressed level of consciousness; 5 = death.
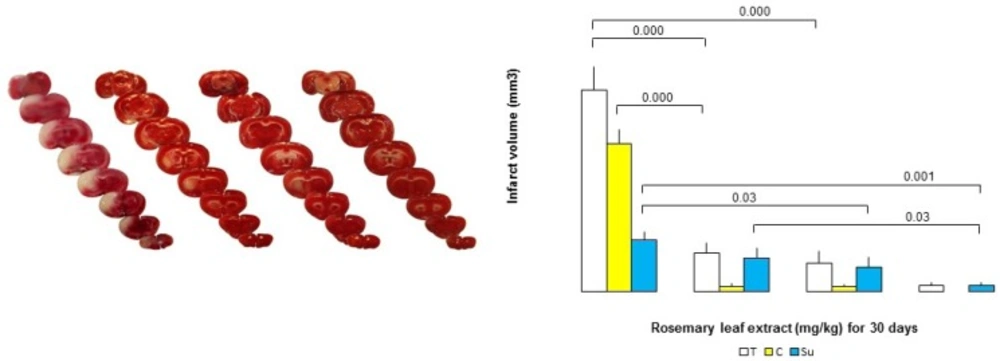
Measurement of infarct volume
The rats were decapitated under chloral hydrate anesthesia (800 mg/Kg), 24 h post-stroke and the brains were rapidly removed. The brains were cooled in ice-cold saline for 10 min and sectioned coronally into eight 2 mm-thick slices starting from the forebrain area (i.e. from the olfactory bulbs to the cortical-cerebellar junction),by using a Brain Matrix Slicer. Brain slices were incubated for 20 min in a 2% solution of 2, 3, 5-triphenyl tetrazolium chloride (Merk, Germany) and kept at 37 °C in a water bath for 15 min. The stained brains were then photographed using a digital camera connected to a computer (Cannon, Japan). Damaged regions were defined as areas that were completely white. The infarct area in each section was measured using image analysis software (UTHSCSA Image Tool). The infarct volume was calculated by taking the average of infarct area on both sides of the slice and multiplying it by section thickness. The total infarct volumes of each brain were calculated as the sum of the infarct volumes of each slice (
22): corrected infarct volume = left hemisphere volume-(right hemisphere volume - infarct volume).
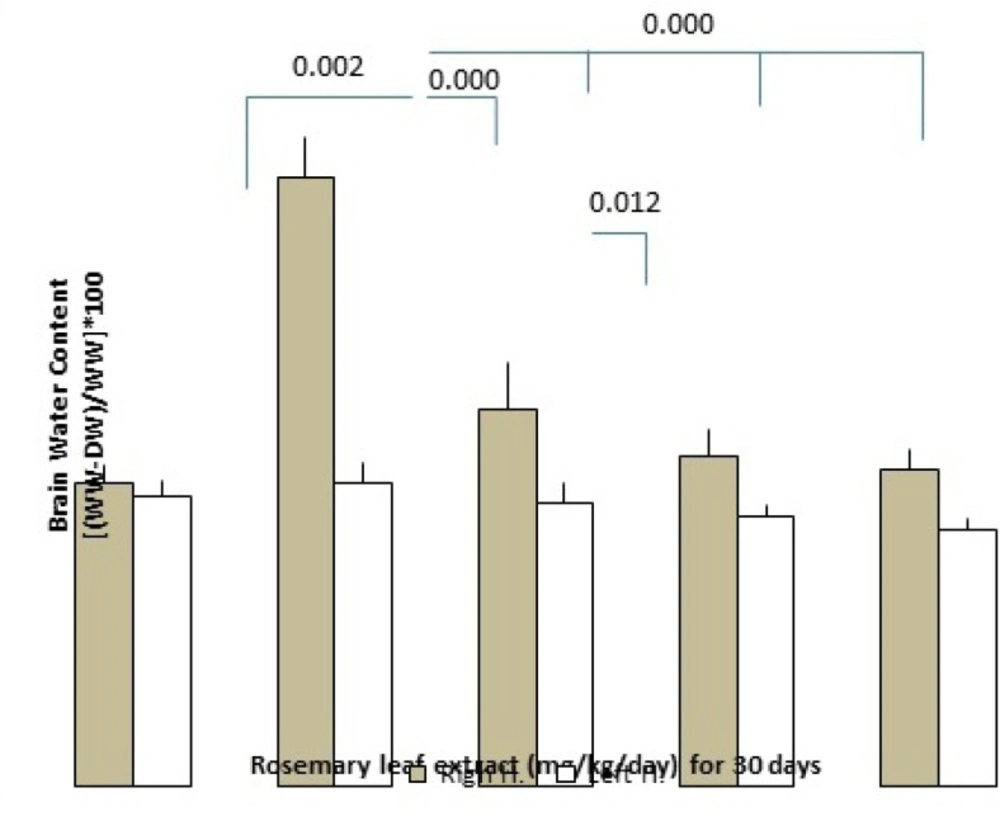
Water content of the brain
The rats were decapitated at 25 h after reperfusion and the brains were removed. Then, the pons and olfactory bulb were removed and the brain tissues were weighted immediately to obtain their wet weight (WW) (
23). Subsequently, brains were dried at 110 °C for 24 h in an oven to determine their dry weight (DW). Brain water content (BWC), was calculated according to the formula: (WW−DW)/WW×100.
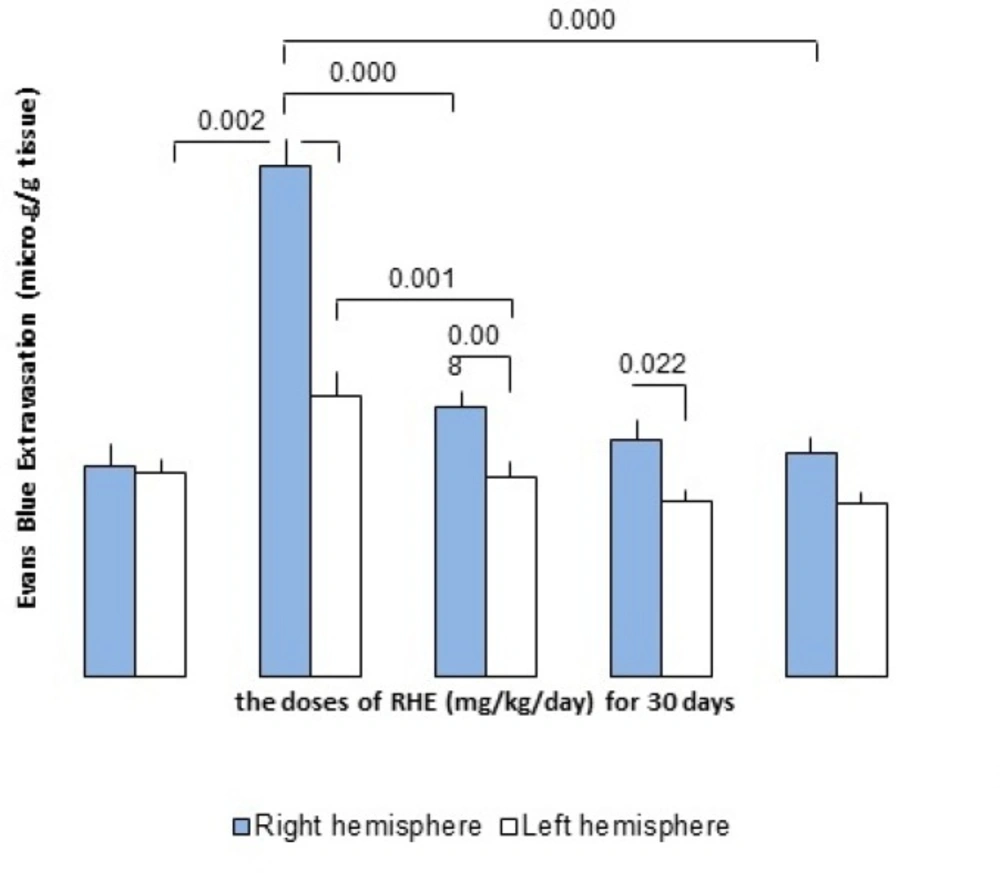
Evaluation of BBB permeability disruption
Measurement of Evans blue extravasations BBB permeability was assessed by measuring EB extravasations. Briefly stating, 4 mL/Kg of 2% Evans blue solution (EB, Sigma Chemicals, USA) in saline was injected into the tail vein, 30 min before reperfusion. Twenty-four h after, rats were deeply anesthetized, chest walls were opened, and trans-cardially perfused with 250 mL saline solution. After decapitation, the brain tissue was removed and hemispheres were separated and weighed. Each hemisphere was homogenized, in the 2.5 mL phosphate buffer saline, and then 2.5 mL of 60% trichloroacetic acid (Merck, Germany) was added to precipitate protein. The mixture was then vortexed for 3 min, cooled for 30 min and centrifuged for 30 min at 1000 ×g. The supernatants were measured at 610 nm for absorbance of EB using a spectrophotometer (UV-visible, USA). The results were expressed as microgram per gram brain tissue calculated according a standard curve (
23).
Statistical analysis
All data are presented as the mean± S.E.M. Statistical analysis of neurological score was assessed using analysis of variance followed by a post hoc Fisher’s indicated least significant difference . For neurological score, we have applied Mann-Whitney U test. A p-value of less than 0.05 was considered to be statistically significant.