
Introduction
Experimental
Results and Discussion
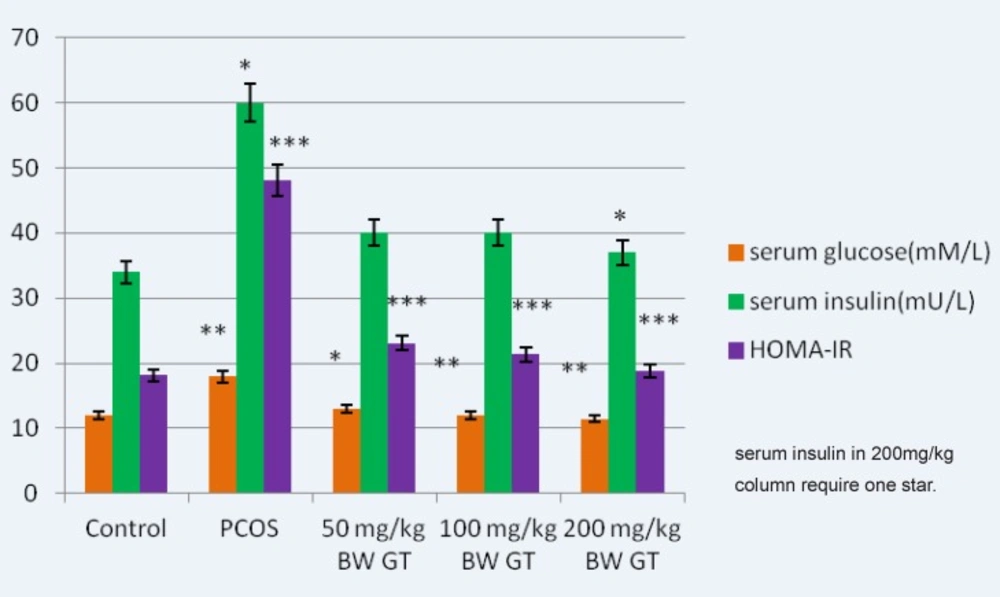
Comparison of the glucose, insulin and HOMA-calculated insulin resistance levels in control, PCOS and experimental groups. Relative to PCOS group, a significant decrease in the glucose relative to PCOS group, a significant decrease in the glucose, insulin (in 200mg/kg BW GT group) and HOMA- calculated insulin resistance level is seen in all green tea extract-treated groups, interaperitoneally. and HOMA-calculated insulin resistance level is seen in green tea extract-treated groups, intraperitoneally.GT: Green Tea, HOMA-IR: Homeostasis Model Assessment- insulinresistance. ***P<0.001; **P<0.01; *P<0.05.
| Groups | LH | Testosterone(ng/dl) | Body Weight(g) | Ovarian Weight(mg) |
|---|---|---|---|---|
| Control | 2.8±0.01 | 50±3.30 | 163±08 | 9.71±0.12 |
| PCOS | 6.75±0.05 (***) | 113±50.15 (***) | 222.8±36.8 (***) | 15.02±0.17 (***) |
| 50 mg/Kg BW GT | 2.22±0.09 (**) | 101±15.11 | 207±15 (*) | 12.4±0.3 (*) |
| 100 mg/Kg BW GT | 2.19±0.06 (***) | 96±40 (*) | 196±12 (**) | 11.23±0.62 (**) |
| 200 mg/Kg BW GT | 1.92±0.02 (***) | 93.5±40 (*) | 194±11 (***) | 11.33±0.54 (**) |
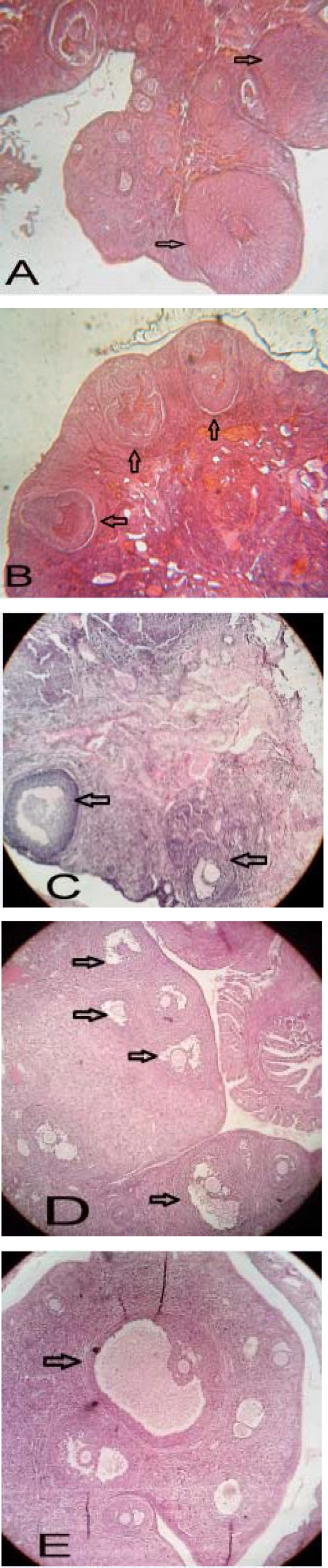
Histological analysis of normal (A), PCOS (B) and 50, 100 and 200 mg/Kg BW green tea extract -treated PCOS (C, D and E respectively) ovaries. Arrows indicate the corpus luteum in figure A, some cysts in figure B, some antral follicles in figure C, some late pre antral follicles in figure D and Gratian follicles in figure E. Ovarian sections were stained with hematoxylin and eosin, X400.
| Groups | The number of primordial follicles | The number of Primary Follicles | The number of Preantral follicles | The number of Preantral follicles | The number of Cystic Follicles | The number of corpus luteum |
|---|---|---|---|---|---|---|
| Control | 45.5±0.33 | 20.57 | 28.66±0.33 | 18.66±0.33 | 0 | 10.33±.36 |
| PCOS | 41±0.50(*) | 9.66±0.03 (***) | 4.66±0.02 (***) | 2.66±0.33 (***) | 4.66±0.13 (***) | 3.33±0.23 (***) |
| 50 mg/Kg BW GT | 41±0.52 | 16.33±0.05 (***) | 18.66±0.06 (***) | 18.66±0.33 (***) | 1.66±0.06 (***) | 9.66±0.33 (***) |
| 100 mg/Kg BW GT | 42±0.57 | 18.6±0.06 (***) | 25.66±0.09 (***) | 25.66±0.66 (***) | 0.33±0.01 (***) | 8.33±0.31 (***) |
| 200 mg/Kg BW GT | 43±0.61 | 20.6±0.07 (***) | 31.33±0.18 (***) | 31.33±0.88 (***) | 0 (***) | 9.01±0.38 (***) |
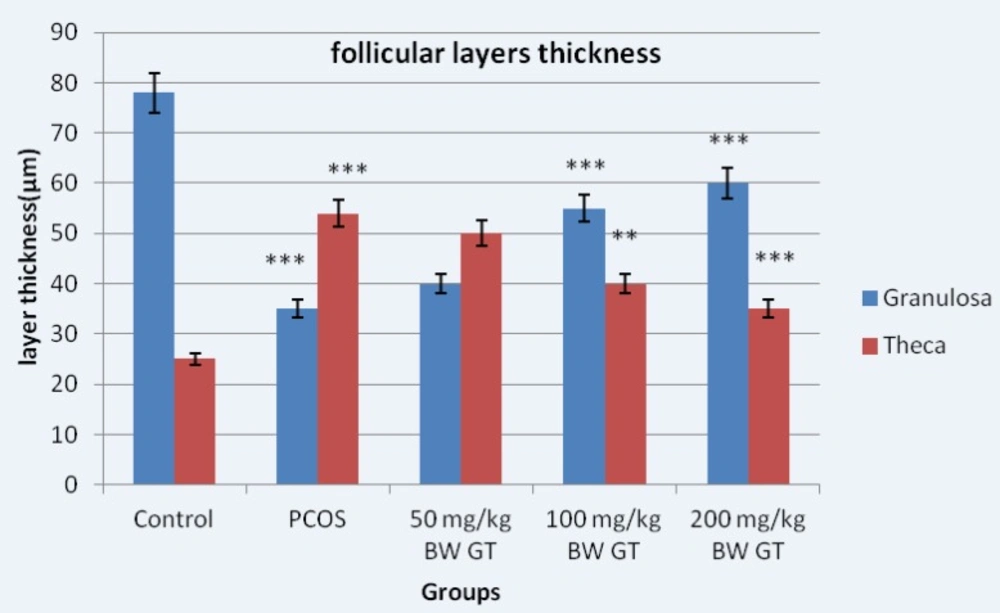
Diameter of the granular and theca layers thickness in control, PCOS control and experimental groups. Measuring the thickness of follicular layers showed the thickness of the theca layer in the PCOS control group significantly increased compared to the control group. However, the thickness of the theca layer in the experimental groups significantly decreased compared to the PCOS control group. Relative to PCOS control group, 10-day sequential treatment with the green tea extract resulted in a significant increase in theca and a significant decrease in granulosa layer thickness. ***P<0.001; **P<0.01.




