
Introduction
Experimental
| Case no | Age of patient | Histological type of tumor* |
|---|---|---|
| 1 | 64 | Serous adenocarcinoma G.3 |
| 2 | 74 | Serous adenocarcinoma G.3 |
| 3 | 67 | Serous adenocarcinoma G.3 |
| 4 | 24 | Serous adenoma of borderline malignancy |
| 5 | 56 | Serous adenocarcinoma G.3 |
| 6 | 72 | Serous adenocarcinoma |
| 7 | 47 | Surface papillary adenocarcinoma |
| 8 | 30 | Serous cystadenoma of borderline malignancy |
| 9 | 43 | Endometrioid adenocarcinoma |
| 10 | 63 | Endometrioid adenocarcinoma G.2 |
| 11 | 53 | Endometrioid adenocarcinoma G2 |
| 12 | 48 | Serous adenocarcinoma |
| Chemotherapeutic drugs | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | P | C | D | E | P+D | P+C | P+E | D+C | D+E | C+E | |
| P1 | -30 | -50 | -56 | -54 | -25 | -25 | -30 | -50 | -50 | -50 | |
| P2 | +40 | 0 | 0 | 0 | +40 | +30 | +40 | 0 | 0 | 0 | |
| P3 | +190 | 0 | 0 | 0 | +110 | +102 | +85 | 10 | 0 | 0 | |
| P4 | +20 | 0 | 0 | 0 | +40 | +20 | +25 | +10 | +10 | +10 | |
| P5 | +40 | 0 | 0 | 0 | +70 | +50 | +50 | +10 | +10 | 0 | |
| P6 | +35 | 0 | 0 | 0 | +90 | +70 | +80 | +100 | 0 | +60 | |
| P7 | +30 | +30 | +10 | 0 | +40 | +20 | +40 | +50 | 0 | +10 | |
| P8 | +70 | +10 | 0 | 0 | +90 | +70 | +60 | +10 | +10 | 0 | |
| P9 | +60 | 0 | 0 | 0 | +70 | +60 | +30 | 0 | 0 | +10 | |
| P10 | -25 | -74 | -77 | 0 | -55 | -50 | -27 | -40 | -40 | -20 | |
| P11 | +70 | +10 | +10 | +10 | +106 | +90 | +90 | +20 | +20 | +10 | |
| P12 | +102 | 0 | 0 | 0 | +90 | +100 | +90 | 0 | +20 | +10 | |
| Chemoteraupetic drugs | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | P | C | D | E | P+D | P+C | P+E | D+C | D+E | C+E | |
| P1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| P2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| P3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| P4 | 0 | 43 + | +30 | +50 | 0 | 0 | +35 | 0 | +50 | +60 | |
| P5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| P6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| P7 | +80 | +98 | +80 | +80 | 0 | +141 | +165 | 0 | +200 | +260 | |
| P8 | +80 | +60 | +80 | +85 | +45 | +90 | +108 | 0 | +220 | +280 | |
| P9 | 0 | 0 | 0 | 0 | 0 | +80 | 0 | +70 | +95 | +70 | |
| P10 | +80 | 0 | +45 | 0 | 0 | 0 | +60 | 0 | 0 | 0 | |
| P11 | +195 | +102 | +40 | +130 | +190 | +160 | +160 | 0 | +70 | +90 | |
| P12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
Results and Discussion
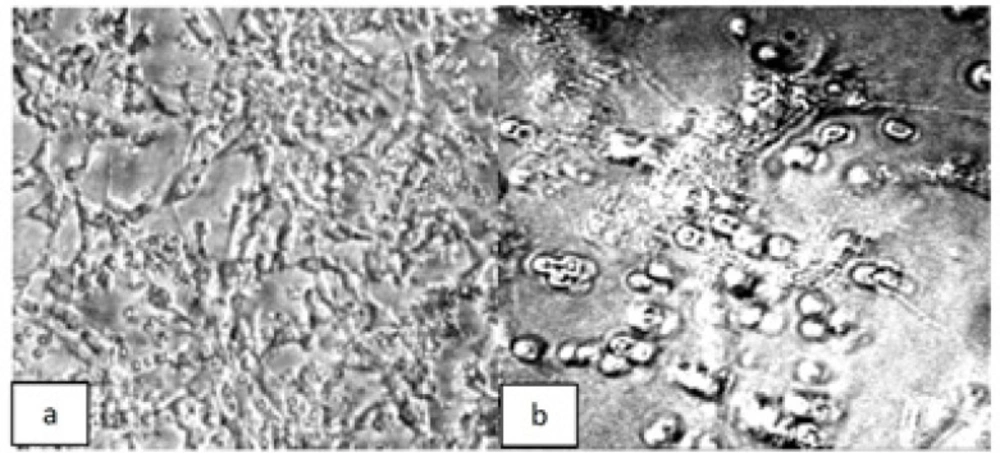
Phase contrast photomicrographs of ovarian tumor cells derived from patient 1, and cultured for 6 days in (a) control media or (b) media containing paclitaxel plus carboplatin
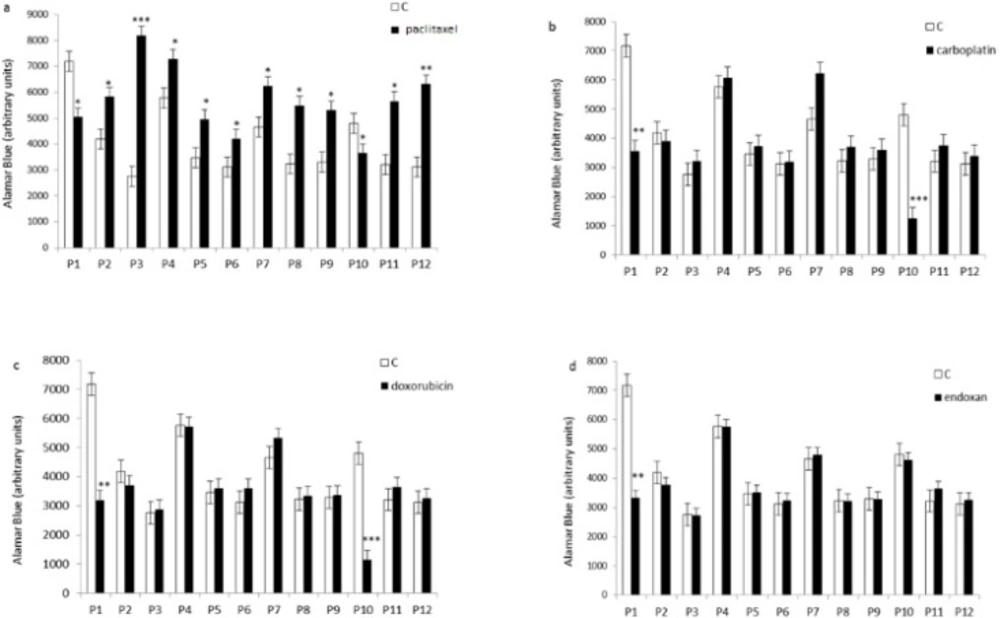
Effect of individual chemotherapeutic drugs on tumor cell proliferation. Cells derived from 12 patients (P1–12) were treated with paclitaxel (13.8µM), doxorubicin (2.5µM), carboplatin (13.4µM), or endoxan (19µM) for 6 days. Cell proliferation was measured using an Alamar Blue assay. *p < 0.05, **p < 0.01, statistically significant inhibition or stimulation of cell proliferation
Effect of combined chemotherapeutic drugs on tumor cell proliferation. Cells were treated with paclitaxel plus doxorubicin (P + D), paclitaxel plus carboplatin (P + C), paclitaxel plus endoxan (P + E), doxorubicin plus carboplatin (D + C), doxorubicin plus endoxan (D + E), or carboplatin plus endoxan (C + E) for 6 days. Cell proliferation was measured using an Alamar Blue assay. *p < 0.05, statistically significant inhibition of cell proliferation; #p < 0.05, statistically significant stimulation of cell proliferation
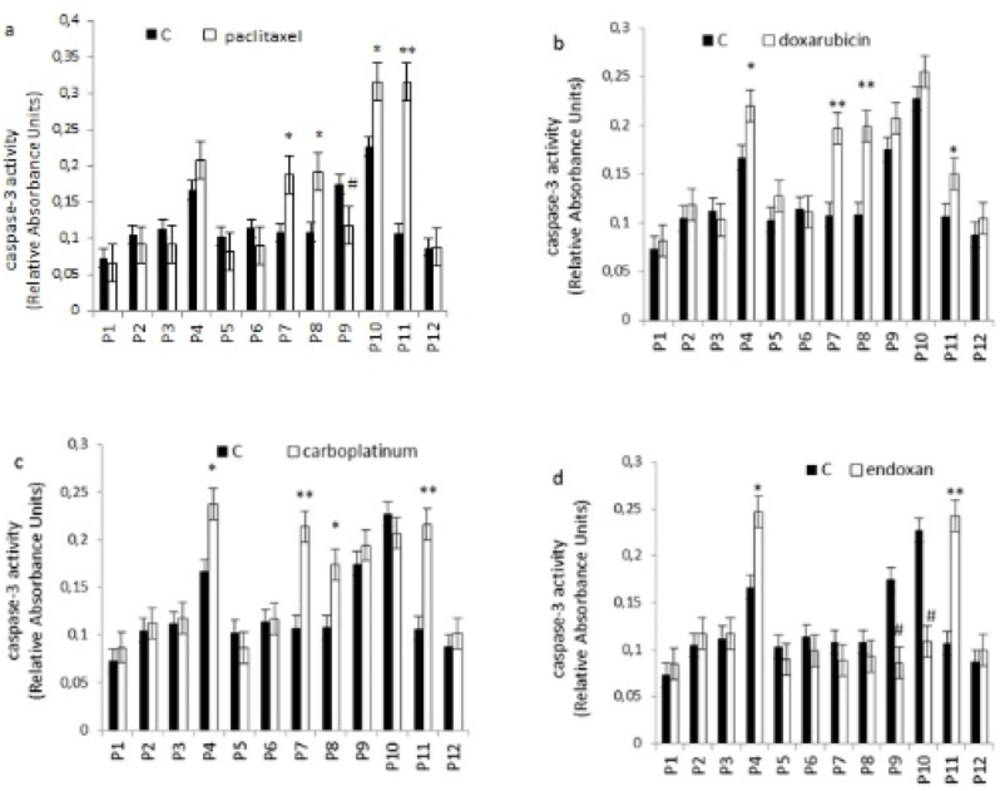
Effect of individual chemotherapeutic drugs on tumor cell apoptosis. Cells were treated with paclitaxel (13.8µM), doxorubicin (2.5µM), carboplatin (13.4µM) or endoxan (19µM) for 6 days. Apoptosis was measured using a caspase-3 assay. *p < 0.05, **p < 0.01, statistically significant stimulation of apoptosis; #p < 0.05, statistically significant inhibition of apoptosis
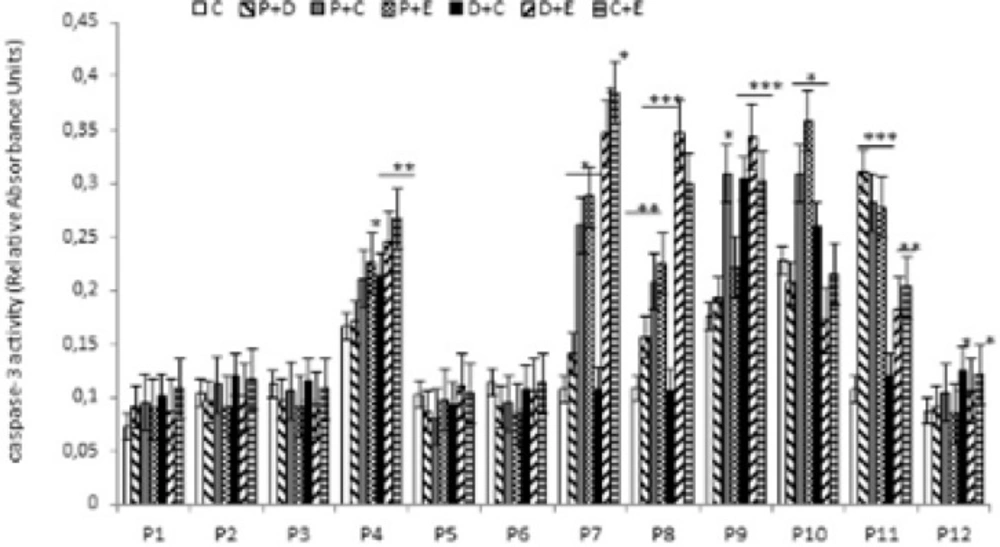
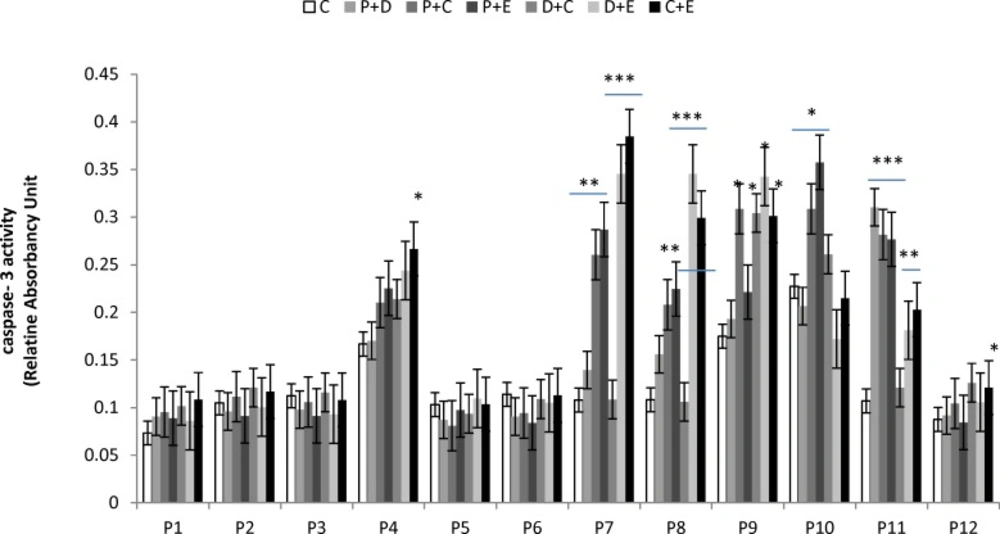
Effect of combined chemotherapeutic drugs on tumor cell apoptosis. Cells were treated with paclitaxel plus doxorubicin (P + D), paclitaxel plus carboplatin (P + C), paclitaxel plus endoxan (P + E), doxorubicin plus carboplatin (D + C), doxorubicin plus endoxan (D + E), or carboplatin plus endoxan (C + E) for 6 days. Apoptosis was measured using a caspase-3 assay. *p < 0.05, **p < 0.01, ***p < 0.001, statistically significant stimulation of caspase-3 activity

