Materials
In this study, 28 male Wistar rats weighing 200-250 gr, (aged 8-10 weeks) were purchased from Physiology Research Center of Kerman University of Medical Sciences and kept under controlled conditions (12 h light/12 h dark) with free access to water and normal rodent chow. The general protocols for animal care and use were approved by the Ethics Committee of Kerman University of Medical Sciences (Permission No. IR.KMU. REC.1395.660).
The animals were randomly divided into 4 groups: Control/vehicle, asthma, asthma + dexamethasone (Dexa), and asthma + myrtenol (MYR).
MYR and ovalbumin (OVA) were purchased from Sigma Aldrich (Gillingham, UK). Dexa was purchased from Iran Hormone (Iran). SOD and MAD assay kits were obtained from Nalondi (Iran). Glutathione peroxidase (GPX) activity colorimetric assay kit was purchased from Biovision (USA). Rat IL-10, IL-1β and TNF-α ELISA kits were obtained from Eastbiopharm (Hangzhou China).
Induction of asthma and treatment protocols
For induction of asthma, the animals were sensitized by intraperitoneal (IP) injection of 1 mg OVA and 200 µg Al (OH) 3 in 0.5 mL phosphate buffered saline (PBS) on days 0 and 7 (26). From days 15 to 42, the animals were exposed to aerosolized OVA (1%) in a closed chamber (40×40×70 cm) using a nebulizer (Omron CX3, Japan) for 30 min, every other day. The rats in the control/vehicle group received IP injection of PBS with aluminum hydroxide on days 0 and 7 and aerosolized with PBS for 30 min every other day from days 15 to 42 (26-28).
At the end of inhalational exposure, the rats in the asthma + MYR group received 50 mg/kg MYR (
24) and in the asthma + Dexa group they received 2.5 mg/kg Dexa (
29), both daily and intraperitonealy, for one week (
30).
Preparation of lung tissue sections and serum
On day 50, the rats were euthanized under deep anesthesia by ketamine (80 mg/Kg) and xylazine (10 mg/Kg) injection, and their blood was collected and sera were separated by centrifugation and stored at -80 °C. The middle lobe of right lung was removed and frozen in liquid nitrogen and stored at −80 °C. The prepared tissues and sera were used for the measurement of oxidants, antioxidants, and interleukins.
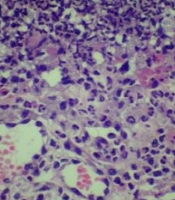
Left lungs of the rats were removed and placed into 10% buffered formalin. Then the tissues were paraffin blocked, and 4-μm slices were obtained and stained with Hematoxylin/Eosin (H&E). The sections were examined microscopically by two pathologists who were blind to the animal groups. The pathologic indices included pneumocyte and fibroblastic hypertrophy and hyperplasia, edematous and degenerative changes, necrosis and airway epithelial denudation, atelectasis, hyperemia, hemorrhage and exudation. The indices were scored using a 5-scale grading system: 0 = no lesion, 1 = slight, 2 = mild, 3 = moderate and 4 = severe lesions (
31).
The damage to the epithelium was evaluated with a grading lesion score as fallow: 1 = normal appearance, 2 = observable loss of cilia, or degeneration or necrosis of less than one-fourth of the ciliated cells without epithelial sloughing, 3 = observable epithelial sloughing and degeneration or necrosis of less than one-fourth of the ciliated cells, 4 = epithelial sloughing and degeneration or necrosis between one-fourth and one-half of the ciliated cells, and 5 = epithelial sloughing and degeneration or necrosis more than one-half of the ciliated cell (
32).
Measurement of oxidants, antioxidants and interleukins
Superoxide dismutase (SOD) was measured using a colorimetric assay based on the ability of SOD to inhibit the auto-oxidation of pyrogallol. Briefly, 50 mg of lung tissue was homogenized on ice in 250 μL of lysis buffer. The sample was then centrifuged at 12000 rpm for 5 min at 4 °C. 50 μL of the supernatant was used to measure the activity of SOD using the related kit, according to the manufacturer′s instructions.
To measure GPX activity in the lung tissue, 100 mg of the tissue was homogenized on ice in 200 µL assay buffer. The homogenate was centrifuged at 10000 x g for 15 min at 4 °C and the supernatant was used. The serum was tested directly. GPX activity was evaluated by reducing Cumene Hydroperoxide and oxidizing glutathione (GSH) to oxidized glutathione (GSSG). The generated GSSG was reduced to GSH with the consumption of nicotinamide adenine dinucleotide phosphate hydrogen (NADPH) by Glutathione Reductase. The decreased NADPH (that is proportional to GPX activity) was measured at 340 nm.
Malondialdehyde (MDA) level, as an index of lipid peroxidation, was estimated by the concentration of thiobarbituric acid reactive substances (TBARS). 250 μL of the serum or homogenized tissue samples were used to measure it according to the kit′s instructions. Tissue samples were lysed using 1.5% potassium chloride solution. The homogenate was centrifuged at 1200 rpm for 10 min.
Quantitative assessments of IL-1β, TNF- α, IL-10 and INF-γ were conducted using double– antibody sandwich Enzyme- Linked Immunosorbent Assay (ELISA) kits based on their manufacturers’ instructions.
Statistical analysis
Quantitative data are presented as Mean ± SEM. After analyzing the normality of the data using Shapiro-Wilk statistical test and were analyzed using ANOVA followed by Tukey′s post-hoc test. Scored data (lung pathology indices) were analyzed using nonparametric tests (Kruskal Wallis test) with the Bonferroni correction. P values less than 0.05 were considered as significant.