With the globally increase of the bacterial resistance, it has been recognized that individual use of antibiotics should be based on the PK/PD principle. Personalized medication is useful to improve efficacy, decrease resistance and minimize toxicity, especially for the drugs with severe adverse reaction (e.g., vancomycin), or population with larger variability on pharmacokinetics (e.g., geriatrics and pediatrics). FDA is advocating the use of computer simulation technology to develop clinical dosage regimen of antibiotics, design assumptions and research the effect of variables on the results, prediction and evaluation of potential benefits and risks of different regimens, in order to provide objective evidence to develop therapeutic schedule. This technique can effectively avoid the dilemmas in real clinical trial such as limited sample size and large subjective interference. MCS is an analytical method for random events or "experiments" based on artificial creation, usually obtains the probability of occurrence of a specified goal by running thousands of simulations, in order to provide reference for decision-making. Most of the published reports on antibiotic regimen optimization by using MCS were based on the PK data of healthy volunteers. Due to the difference between healthy subjects and patients, the applicability of MCS results was limited. MCS research based on the PPK is the focus of academic field in the present, which can truly reflect the disposition of drugs under clinical disease states.
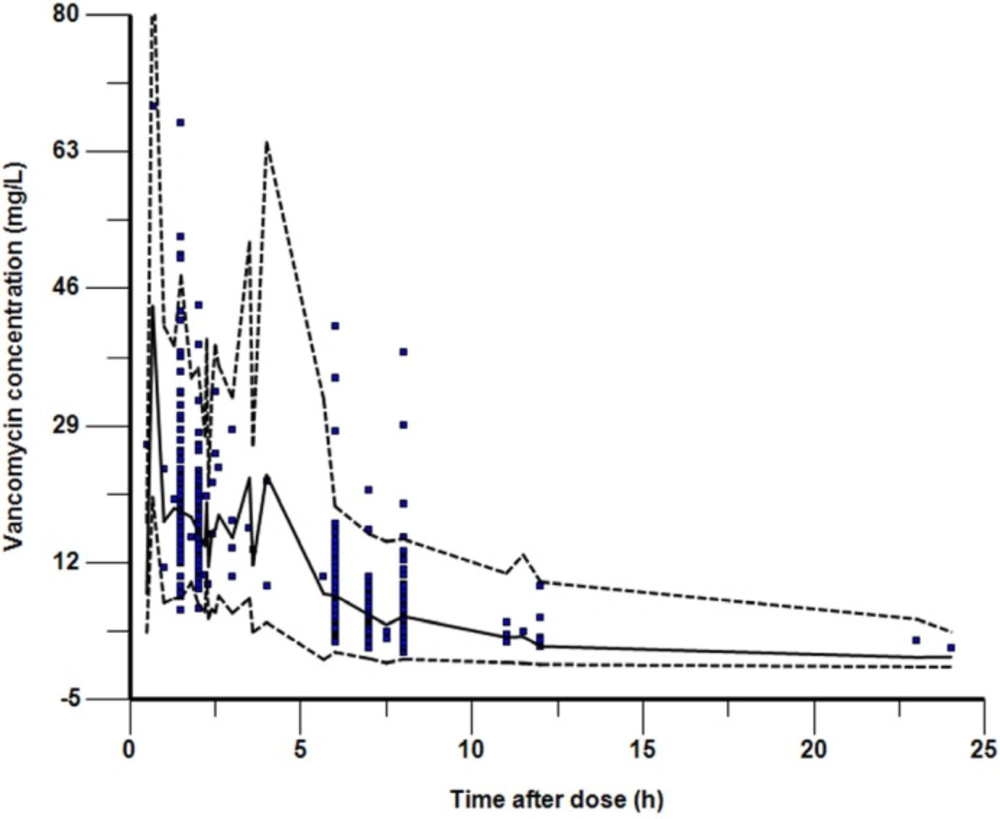
In this study, the data of 155 children (aged from 1 month to 16 years) infected with MRS were used to establish a PPK model suitable for Chinese children. And then the PK parameters were obtained by Bayesian method. The mean values of CL and V
d were 0.133 ± 0.066 L·kg
-1·h
-1 and 0.65 ± 0.30 L·kg
-1, respectively. Our result were similar with that of Wrishko
et al.(16) (in which CL= 0.12 L·kg
-1·h
-1 and V
d= 0.57 L·kg
-1) and Yasuhara
et al.(
17) (in which CL = 0.119 L·kg
-1·h
-1 and V
d= 0.522 L·kg
-1). But the value of CL is faster than that reported by Marques-Minana
et al.(
23) (0.066 L·kg
-1·h
-1) in neonates, probably due to that, the age of the children in the present study were older. About 80%~90% of vancomycin was excreted by glomerular filtration in less than 24 h (
8), some by renal tubular secretion (
24), therefore renal function, especially the glomerular filtration rate (GFR) will directly affect the
in-vivo elimination rate of vancomycin. Dailly
et al. (
25) found a positive correlation between GFR and vancomycin clearance in 70 patients suffered burns. Chen YC
et al.(
26) found the correlation coefficient between GFR and vancomycin clearance was 84.65% in 65 patients infected with MRSA. Many vancomycin PPK studies also found various covariates which indirectly reflect the GFR such as CRE(
27), Ccr (
28), or cysteine proteinase inhibitor in serum c (Cystatin c) (
26,
29) were significant correlated with vancomycin clearance. Modified Schwartz′s formula (
15) was used to calculate GFR in children with this study and it was successfully integrated into the final model, well elaborated the quantitative relationship between GFR and vancomycin clearance. After grouping according to NKF-K/DOQI standard, we found vancomycin clearance and elimination rate constant in children with 30 ≤ GFR<60 mL/min·1.73m
2 decreased by 39.4% and 42.4% compared with the children with GFR ≥ 90 mL/min·1.73m
2, which proved once again the necessary of adjustment for vancomycin dosage.
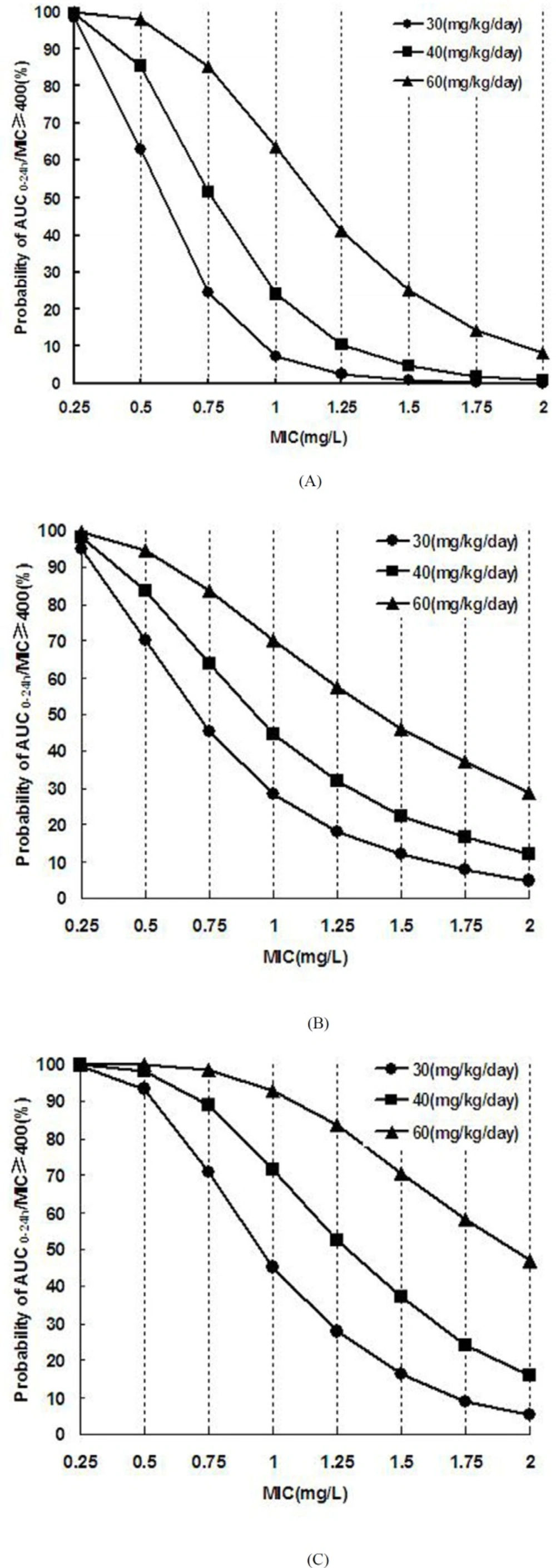
After establishing the vancomycin PPK model and obtaining the PK parameters in patients with different renal function, a large sample (10 000 cases) simulation "experiment" was conducted by using MCS to explore the efficacy and safety of various dosage regimen under different preset scenes. The correlation between vancomycin antimicrobial effect against MRSA and AUC
0-24h/MIC has been reported since 90′s of the last century in animal models (
7,
8). Subsequently, a number of large samples of human PK/PD studies (
5,
9,
10) confirmed that vancomycin organizational penetration and anti-infection is optimal when its AUC
0-24h/MIC was above 400. Current United States infectious disease society (IDSA) (
4,
11) and Chinese expert consensus recommends that AUC
0-24h/MIC ≥ 400 should be regarded as the target indicator. Our MCS results indicated that the dose of 40mg·kg
-1·d
-1 was effective against MRSA strains with MIC ≤ 0.50 mg·L
-1 (PTA of AUC
0-24h/MIC ≥ 400 was ≥ 85.31%) in patients with normal renal function. But this dosage regime may fail to kill the bacteria with MIC ≥ 0.75 mg·L
-1 (PTA ≤ 51.53). In that case, a larger dose was needed. For MRSA infection with MIC 1-2 mg·L
-1, the success rate is not enough (63.64%) even given a dose of 60mg·kg
-1·d
-1. In 2006, United States Clinical Laboratory Standardization Association (CLSI) reduced the susceptibility breakpoint of vancomycin from 4 to 2 mg·L
-1 (
11,
30), whereas our simulation results indicated that the conventional doses of 40-60mg·kg
-1·d
-1 is only effective for MRSA with MIC ≤ 1 mg·L
-1 but inadequate for MRSA with MIC 1-2 mg·L
-1. Eiland
et al. (
31) analyzed the vancomycin TDM results of 295 children and found vancomycin given at 40-60mg·kg
-1·d
-1 was difficult to achieve effective target trough concentration (10-20mg·L
-1). They calculated using a formula and concluded that 70mg·kg
-1·d
-1 was needed for patients with normal renal function to achieve the target trough concentration of 10 mg·L
-1. Giachetto
et al. (
32) also observed that the probability of AUC
0-24h/MIC ≥ 400 is only 50% even given vancomycin 39.92mg·kg
-1·d
-1 for MRSA strains with MIC 1 mg·L
-1. Frymoyer
et al. (
33) suggested that the probability of AUC
0-24h > 400 will be over 90% when vancomycin trough concentration was at least 10 mg·L
-1. That is, vancomycin trough concentration may not need to reach 10 mg·L
-1 for MRSA strains with MIC ≤ 1 mg·L
-1, whereas for MRSA strains with MIC 1-2 mg·L
-1 the concentration should be more than 10 mg·L
-1 which was difficult to achieve routine dose. Therefore, supernormal dosage is permissible when the bacterial resistance is increased in order to ensure clinical efficacy. However, the risk of adverse drug reaction will increase with the dose. Even though the ototoxicity is rarely reported after the purity of vancomycin was improved, many toxicologic studies have demonstrated that vancomycin nephrotoxicity sharply increased when its trough concentration was above 20 mg·L
-1 (
19-
22), especially for co-administration with nephrotoxic drugs such as aminoglycoside (
4). Our simulation results indicated that the probability of C
smin > 20 mg·L
-1 will be more than 20% when vancomycin dose is 70,50, and 30 mg·kg
-1·d
-1 respective for patients with GFR ≥ 90 mL/min·1.73 m
2, 60 ≤ GFR < 90 mL/min·1.73 m
2 and 30 ≤ GFR < 60 mL/min·1.73 m
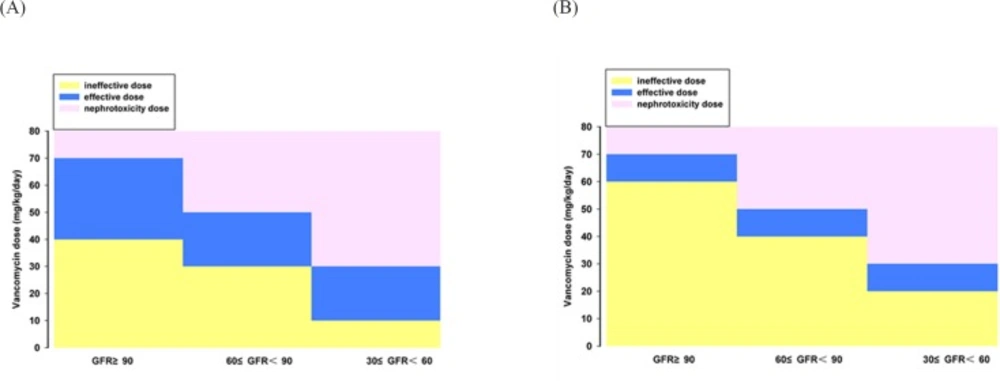
2. In that cases, the probability of nephrotoxic were greater, so the corresponding dose was not recommended. Combined with the simulation results of efficacy and safety, the reasonable dose range of vancomycin for children with various degrees of renal function is obtained (
Figure 4). We concluded that the range of vancomycin dose is narrow for MRSA strains with MIC 1-2 mg·L
-1; hence, the treatment will be more difficult and the cure rate is not high. Since the MRSA strains with MIC 1-2 mg·L
-1 are prone to mutate into heterogeneous Vancomycin-Intermediate Staphylococcus aureus (hVISA), producing offspring MIC ≥ 4 mg·L
-1 resistant subpopulation (30), which should be paid attention and a better way to fight infection was necessary. For this type of strain, the clinicians can increase the dose of vancomycin under blood concentrations monitoring and toxicity monitoring, or combine vancomycin with rifampicin (
34) or fosfomycin (
35), or replace with lower nephrotoxic drugs such as linezolid, daptomycin, and teicoplanin for the patients with moderate or even worse renal function.
The present study suggested that individualized dosing regimen of vancomycin should be developed in accordance with bacterial resistance and renal function of the patients, and fully considering the pros and cons in order to ensure the efficacy and safety of antibiotic therapy. According to the simulation results, 40-70, 30-50, 10-30 mg·kg-1 vancomycin daily dose for MIC ≤ 1 mg·L-1 MRSA infection treatment is adapted to pediatric patients with GFR ≥ 90, 60 ≤ GFR < 90 and 30 ≤ GFR < 60 mL/min·1.73m2 , respectively. And the adjustable dosage interval of vancomycin is narrow for treating MIC 1-2 mg·L-1 MRSA infection. The limitation of the study is the number of the patients with renal insufficiency is small, so fitting errors may exist for the pharmacokinetic characteristics of such population. We will collect more patients in the future to in-depth explore the regularity of vancomycin PK/PD in Asian children.
Funding: This work was funded by The Key Project of Science and Technology of Wuhan (2013060602010258) and The National Futang Fund for Children’s Medicine Development (2015 No.33).
Conflicts of interest: All authors have no potential conflicts of interest to declare.
Ethical approval: All procedures in this study were carried out in accordance with the 1964 Helsinki declaration and its amendments and the ethical committee or institutional review board which approved the study.
Informed consent: Written informed consent was obtained from the legal representative or guardian of each patient when they began treatment but was not required for the present analyses because this was a retrospective study.