






1. Background
Today, human resources, as the most valuable asset of the organization, are facing many problems. Therefore, management experts and organizational psychologists pay attention to the factors that affect the increase or decrease of human efficiency, and try to increase the impact of effective factors and reduce the role of negative factors by identifying these factors and applying the necessary measures (1). The International Labor Organization estimates that there are 270 million occupational accidents in the world each year, resulting in the absences of more than three working days and 210,000 mortalities in the workplace (2). The cost of these injuries is so high that in the UK, the total cost of workplace injuries to employers in 2005 - 2006 was estimated at around 1.2 - 1.3 billion pounds (3). Today, industry executives have realized that paying attention to safety is one of the most important ways to improve productivity and even to transfer and develop the technology. Even many managers in developed countries see and treat safety as a high-return investment, both economically and humanely. Due to the costs of accidents and the benefits of safety, it is necessary to acknowledge workplace safety by developing and strengthening occupational health institutions, implementing effective measures, and doing safety research to prevent hazards (4).
One of the important determinants of occupational safety and health is organizational risk factors in the workplace, which include psychosocial factors such as safety climate (5, 6). Safety, which is a psychological phenomenon, was first introduced by Zohar and refers to employees' shared perceptions of how to manage safety and the real priority of safety in the workplace. Therefore, the safe atmosphere is temporary and can be changed. Zohar studied the safety climate in various industrial organizations and determined eight dimensions for it, such as management's attitude towards safety, the effects of implementing safety instructions on promotion, work pressure, social status of individuals, observance of safety principles through a safety officer, the status of the safety committee, the importance of safety training and risks in the workplace (7, 8). In other words, the safety climate examines employees' perceptions and inferences about the work environment, the level of management's interest in safety and safety-related measures, and the degree of participation in risk control (9). Safety climate is a state of safety that indicates the basis of safety culture in working groups, factories, or organizations and is a practical tool to measure the behavior and attitudes of employees towards safety (10). Safety climate predicts and encourages workers to work safely and affects the occurrence of occupational accidents (11). A direct relationship has been reported between the safety climate and the safety performance of an organization or workplace (12) so as to reduce workplace accidents (13).
Studies have shown that the difficulty in decision-making in the absence of a safe climate is 17.5% in the health sector and 5.6% in security industries that require a high degree of confidence; besides, the experience of decision-making in this situation by health staff is 12 times more than by the staff of security organizations. Thus, fundamental changes to achieve a safe climate in medical centers are very important. Also, there is a significant relationship between safety climate and predictions of workplace injuries to the extent that 70% of occupational injuries relate to the safety climate in the workplace (14). That is why health care organizations, by examining safety culture, hold managers accountable for the proper allocation of resources and manpower (15).
One of the most important areas of sustainable health development in human societies is the health sector, which has a direct relationship with human health and has the serious task of maintaining and restoring health to human society. The hospital is also one of the most important components of the health care network. Today, managing hospitals effectively is one of the main challenges of any country's health care system (16). Nurses are one of the largest groups of health care providers in hospital wards, and patients have more contact with nurses compared to other care providers. Therefore, the inadequacy of the work of this group will have irreparable results due to their important role in the recovery of patients (17). The nursing workforce is also the basis for providing health care in all countries. As a result, the effectiveness of health systems and the quality of health care are directly related to the performance of nurses. The nursing workforce in health systems has an important place in the provision of health services (18). Therefore, to increase the productivity and efficiency of health organizations, paying attention to the needs of nurses and ensuring their mental and physical health is of special importance (19). In many situations, nurses face patients and incurable diseases and constantly experience severe psychological stress (20). Stressful occupational nursing is a stressful profession with a high rate of accidents and occupational diseases (21, 22). These factors can cause fatigue in the long run and have adverse effects on the professional activity of nurses (23). Fatigue is an unpleasant feeling that is also a useful function to prevent physical and cognitive damage. This category is a general, multi-causal, and multi-dimensional concept that all people experience, and despite having different mental, behavioral, and physiological manifestations, it does not have a comprehensive and clear definition (24).
In fact, fatigue is a condition that only the individual is able to recognize and the person experiences a constant feeling of analysis and reduction in the capacity of general physical and mental function (5). Today, nurses experience high levels of fatigue, which affects the outcomes of patient care and imposes significant costs on the health care system (25). Fatigue can reduce the ability to process information, reduce response to dangerous situations, decrease the level of safety, lower the physical and mental level, reduce consciousness, and impose negative effects on the safety and performance of people (26, 27). In other words, fatigue reduces the physical performance of nurses and is a potential factor in increasing the incidence of human error (28), (29). These errors can lead to death and injury to thousands of people each year, and increase medical costs (30). Fatigue is also one of the most important factors for nurses to leave work environments (31). Occupational fatigue is known as a risk factor for musculoskeletal disorders (28). The prevalence of fatigue reported by nurses was 91.9%, and two-thirds of nurses experienced fatigue in most cases (32). Decreased self-confidence, decreased job satisfaction or dissatisfaction, failure to take on organizational responsibilities, increased transfer, and leaving the service are the consequences of fatigue (5).
2. Objectives
Because nurses spend time with patients more than do any other treatment team members and due to the role of fatigue and its consequences such as burnout, increased medication errors, and reduced quality of nursing care and due to the importance of the awareness of the safety climate in the workplace, and also due to the limited studies of safety climate related to the medical environment in the country and since health centers are one of the most important organizations in a country that play a major role in promoting the health of society, this study aimed to investigate the relationship between occupational fatigue and safety climate in nurses.
3. Methods
This descriptive-analytical study was done in 2018. The statistical population included all nurses working in Shahrekord teaching and research hospitals. We enrolled 216 nurses in the study using a quota random sampling method. Based on the following formula, the subjects entered the study:
The normal distribution value of type II error was 0.2 (statistical power 80%) and the error level was 5%. Besides, the expected correlation between occupational fatigue and safety climate was considered to be 0.19.
Inclusion criteria were nurses with at least a bachelor's degree in nursing or higher who were willing to participate in the study. Before collecting information, participants completed the consent form. Data collection tools included a demographic and occupational characteristics questionnaire (age, gender, shift work, etc.), nurses' safety climate questionnaire, and Multi-dimensional Fatigue Inventory (MDFI). Exclusion criteria included unwillingness to continue cooperation, the presence of underlying illness, and psychiatric disorders recorded in the medical record.
3.1. Nurses' Safety Climate
Nurses' safety climate questionnaire was used to assess the nurses' safety climate. This questionnaire has 22 questions of six factors concerning nurses' safety climate, including cumulative burnout (five questions), education (five questions), communication with doctors (three questions), communication with nurses (three questions), supervisors' attitude (three questions), and reporting errors and mistakes (three questions). The answers to the questions are based on a five-point Likert scale (score 1 for strongly disagree, score 2 for disagree, score 3 for neither agree nor disagree, score 4 for agree, and score 5 for strongly agree). The average score to questions related to each factor was considered as the score of that factor and according to the scale used, the score of each factor was in the range of 1 to 5. Considering that all questions have a positive aspect, higher scores of safety climate indicate a better situation in terms of safety (33). The questionnaire was translated into Persian and the content validity of the questionnaire was 0.77 and its reliability was 0.79 (34).
Multidimensional Occupational fatigue: This questionnaire consists of 20 questions that include five areas: (1) general fatigue, (2) physical fatigue, (3) mental fatigue, (4) decreased activity, and (5) decreased motivation, with each area including four items (35). Each question is answered based on a three-point Likert scale in the range of “yes, it is absolutely correct” to “no, it is completely wrong”. A score of 1 to 3 is devoted to each item, and reverse scoring is done for some items. Therefore, the total score of each domain will be 4 - 20 and the total score of the scale is obtained from the sum of all domains’ scores, which can be between 20 and 100. This questionnaire has been translated into Persian, with a reliability of more than 0.7 and a validity of 0.85 (36).
3.2. Data Analysis
After data collection, data were entered into SPSS version 21 software. Then, the normality of the data was checked. Statistical tests for two independent samples, analysis of variance, Mann-Whitney, Kruskal-Wallis, and linear regression model were used to analyze the data according to the objectives of the study. Initially, using univariate regression analysis, the effect of each independent variable was examined on fatigue separately. Then, the variables with a confidence level of less than 0.2, after examining the alignment, entered the final multiple regression model.
3.3. Ethics Approval
Ethical approval for this study was obtained from the University of Social Welfare and Rehabilitation Sciences (IR.USWR.REC.1399.049).
4. Results
In the present study, 216 nurses were enrolled, of whom 116 (53.7%) were women and 100 (46.3%) were men. The demographic information of the participants is given in Table 1.
| Variable/Category | Number | Percentage |
|---|---|---|
| Gender | ||
| Female | 116 | 53.7 |
| Male | 100 | 46.3 |
| Shift work | ||
| Morning | 158 | 73.1 |
| Evening | 38 | 17.6 |
| Night | 9 | 4.2 |
| Rotating | 11 | 5.1 |
| Marital status | ||
| Single | 57 | 26.4 |
| Married | 159 | 73.6 |
| Level of education | ||
| Bachelor | 130 | 60.2 |
| Masters | 69 | 31.9 |
| Ph.D. | 17 | 7.9 |
| Satisfaction with colleagues | ||
| Yes | 103 | 47.7 |
| No | 113 | 52.3 |
| Second job | ||
| Yes | 25 | 11.6 |
| No | 191 | 88.4 |
| Job satisfaction | ||
| Yes | 102 | 47.2 |
| No | 114 | 52.8 |
| Age (Miankin's standard deviation) | 36.62 ± 9.43 | |
| Work Experience (Miankin's Standard Deviation) | 16.05 ± 7.79 | |
Demographic Information of Study Participants
According to the data in Table 1, the mean age of nurses was 36.62 ± 9.43 years, with a minimum of 23 years and a maximum of 57 years. Also, the average work experience was 16.05 ± 7.79, with a minimum of one year and a maximum of 28 years.
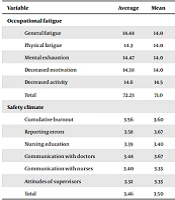
According to Table 2, the average score of nurses' occupational fatigue was 72.23 ± 7.75, with the lowest score of 58 and the highest score of 97. Also, the minimum score of safety climate was 2.55 and the maximum score was 4.18. The mean score of nurses' safety climate was 3.46 ± 0.305. The results of the Kolmogorov-Smirnov test also showed that only the variables of general fatigue and nursing education followed the normal distribution and other variables did not have a normal distribution.
| Variable | Average | Mean | Standard Deviation | Minimum | Maximum | Statistics Value a | P-Value |
|---|---|---|---|---|---|---|---|
| Occupational fatigue | |||||||
| General fatigue | 14.48 | 14.0 | 2.50 | 8.0 | 20.0 | 1.21 | 0.106 |
| Physical fatigue | 14.3 | 14.0 | 2.49 | 8.0 | 20.0 | 1.73 b | 0.005 |
| Mental exhaustion | 14.47 | 14.0 | 2.45 | 8.0 | 20.0 | 1.48 c | 0.024 |
| Decreased motivation | 14.38 | 14.0 | 2.49 | 9.0 | 20.0 | 1.51 c | 0.02 |
| Decreased activity | 14.6 | 14.5 | 2.55 | 9.0 | 20.0 | 1.37 c | 0.046 |
| Total | 72.23 | 71.0 | 7.75 | 58.0 | 97.0 | 1.76 b | 0.004 |
| Safety climate | |||||||
| Cumulative burnout | 3.56 | 3.60 | 0.54 | 2.20 | 4.80 | 1.63 b | 0.01 |
| Reporting errors | 3.58 | 3.67 | 0.66 | 2.0 | 5.0 | 1.69 b | 0.007 |
| Nursing education | 3.39 | 3.40 | 0.58 | 1.80 | 4.60 | 1.33 | 0.057 |
| Communication with doctors | 3.48 | 3.67 | 0.75 | 1.33 | 5.0 | 1.85 b | 0.002 |
| Communication with nurses | 3.40 | 3.33 | 0.70 | 1.67 | 5.0 | 1.68 b | 0.007 |
| Attitudes of supervisors | 3.32 | 3.33 | 0.75 | 1.33 | 5.0 | 1.39 c | 0.04 |
| Total | 3.46 | 3.50 | 0.305 | 2.55 | 4.18 | 1.46 c | 0.028 |
Description of Statistical Indicators of Occupational Fatigue and Safety Climate Among Nurses and Evaluation of Their Normality
The relationships of safety climate and its subscales with job characteristics and demographics are shown in Table 3. Nonparametric statistical tests including Mann-Whitney U and Kruskal-Wallis were used to investigate the relationship between all variables in Table 3. The parametric tests including independent sample t test and one-way analysis of variance were used only in the analysis of nursing education variable.
| Variables | Cumulative Burnout | Nursing Education | Communication with Doctors | Communication with Nurses | Attitudes of Supervisors | Reporting | Safety Atmosphere |
|---|---|---|---|---|---|---|---|
| P-Value | |||||||
| Gender | 0.085 | 0.006 a | 0.52 | 0.99 | 0.46 | 0.96 | 0.54 |
| Marital status | 0.81 | 0.19 | 0.42 | 0.62 | 0.15 | 0.37 | 0.14 |
| Level of education | 0.61 | 0.26 | 0.71 | 0.33 | 0.34 | 0.08 | 0.25 |
| Shift work | 0.005 a | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a | 0.005 a | 0.0001 a |
| Job satisfaction | 0.11 | 0.06 | 0.08 | 0.043 | 0.036 b | 0.71 | 0.08 |
| Satisfaction from colleagues | 0.08 | 0.025 b | 0.036 b | 0.026 b | 0.25 | 0.63 | 0.15 |
| Second job | 0.005 a | 0.001 a | 0.024 b | 0.0001 a | 0.0001 a | 0.247 | 0.0001 a |
Relationship Between Safety Climate and Its Subscales With Job Characteristics and Demographics
According to the findings of Table 3, the relationship between safety climate and its subscales and job characteristics and demographic variables showed that the safety climate and its subscales were significantly different between different groups of fascination. On the other hand, the scores of communication with nurses and the attitude of supervisors were lower in people who were not satisfied with their job and this difference was significant. Also, nursing education and communication with physicians scored higher for people who were satisfied with their colleagues (P-value < 0.05). Finally, the safety climate and its subscales were significantly different between those who had a second job and those who did not have (P-value = 0.000).
The relationships of occupational fatigue and its subscales with job characteristics and demographics are shown in Table 4. Nonparametric statistical tests including Mann-Whitney U and Kruskal-Wallis were used to investigate the relationship between all variables in Table 4. The results showed that occupational fatigue, general fatigue, and physical fatigue were more in women. Married people also had more general fatigue, physical fatigue, reduced activity, and occupational fatigue than single people (P-value < 0.05). Occupational fatigue and its subscales were more in people who worked part-time or on a rotating basis than in other people (P-value = 0.000). Nurses who were dissatisfied with their colleagues had more general fatigue, mental fatigue, reduced activity, and occupational fatigue (P-value < 0.05). Also, people who had a second job had more occupational fatigue and its subscales (P-value = 0.000). In order to test the effect of job, demographics, and job characteristics on the dependent variable, occupational fatigue using multiple linear regression by forward method, finally the variables of shift work, second job, age and safety climate remained in the final model. The results are as follows.
| Variables | General Fatigue | Physical Fatigue | Mental Exhaustion | Decreased Motivation | Decreased Activity | Occupational Fatigue |
|---|---|---|---|---|---|---|
| P-Value | ||||||
| Gender | 0.0001 a | 0.037 b | 0.53 | 0.07 | 0.08 | 0.029 |
| Marital status | 0.036 b | 0.0001 a | 0.07 | 0.32 | 0.035 b | 0.004 a |
| Level of Education | 0.17 | 0.08 | 0.44 | 0.71 | 0.39 | 0.14 |
| Shift work | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a |
| Job satisfaction | 0.52 | 0.22 | 0.14 | 0.58 | 0.053 | 0.35 |
| Satisfaction from colleagues | 0.007 a | 0.07 | 0.037 b | 0.023 | 0.18 | 0.004 a |
| Second job | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a | 0.0001 a |
Relationship of Occupational Fatigue and its Subscales with Job Characteristics and Demographics
In Table 5, the regression results of job characteristics, demographics, and safety climate effects on the dependent variable, occupational fatigue, show that the above variables could explain about 69.8% of the changes in the response variable, occupational fatigue. It should be noted that the effect of the shift variable on occupational fatigue was about 0.53. This means that by keeping other variables constant if shifts increase one unit, the rate of occupational fatigue will increase by 53%.
| Variables | Model coefficients | T Statistics | P-Value | ||
|---|---|---|---|---|---|
| Regression Coefficient (β) | Standard Deviation Error | Standardized Regression Coefficient (β) | |||
| Constant | 66.19 | 3.97 | - | 16.67 | 0.000 a |
| Shift work | 5.21 | 0.45 | 0.53 | 11.62 | 0.000 a |
| Second job | 4.77 | 1.16 | 0.19 | 4.11 | 0.000 a |
| Age | 0.18 | 0.04 | 0.22 | 4.59 | 0.000 a |
| Safety atmosphere | -2.42 | 1.04 | -0.09 | -2.33 | 0.021 b |
Regression Test of Job Characteristics, Demographics, and Safety Atmosphere Effects on Dependent Variable (Occupational Fatigue)
The effect of the second job variable on occupational fatigue was about 0.19. This means that by keeping the other variables constant, having a second job increases the rate of occupational fatigue by 19%. That is, if a person who does not have a second job chooses a second job, it can be stated that there is a 95% chance that his occupational fatigue will increase by 19%. Also, the effect of the age variable on occupational fatigue was about 0.22. This means that by keeping other variables constant if the age increases one unit, the rate of occupational fatigue will increase by 22%. Finally, the effect of the safety climate variable on occupational fatigue was about -0.09. This means that by keeping other variables constant if the safety climate increases one unit, the rate of occupational fatigue will decrease by 9% (Table 5).
5. Discussion
This study aimed to investigate the relationship between occupational fatigue and safety climate in nurses. Finally, 216 nurses entered the study. The mean scores of occupational fatigue and safety climate in nurses were 72.23 ± 7.75 and 3.46 ± 0.305, respectively.
The findings showed no significant relationship between the education level and safety climate, which was not in line with the findings of the studies by Moghani Bashi Mansourieh et al. (37), Kalte et al. (27), and Depietro (19). This may be related to the differences between the study populations, and the fact that this result confirms that an individual factor such as education does not have much effect on safety climate. However, the results of the studies by Moghani Bashi Mansourieh et al. (37), Heidari et al. (29), and Gurková et al. confirm the findings of the present study (38). There was no statistically significant difference between gender and safety climate, which was in line with the studies by Kho et al. (12), Raftopoulos et al. (3), Kalte et al. (27), and Sarsangi et al. (13), but did not match with the study by Wu et al. (11). In the Wu study, gender had a significant effect on the safety climate of university laboratories, which could be due to a different statistical population from our study population. Also, no significant relationship was observed between job satisfaction and safety climate, which was not consistent with the study by Lee (14), and Williamson et al. (15). On the other hand, people who were not satisfied with their job had a lower score on communication with nurses, i.e. their colleagues, and also a lower score on supervisors' attitudes, which was not observed in a similar study. This can be important in the sense that nurses who do not have a strong yet positive relationship with other nurses and colleagues are dissatisfied with their work environment and even their job, and such a lack of interaction with colleagues may play a key role in their satisfaction (39, 40).
In the present study, 72.23% of nurses reported occupational fatigue, which indicates a high rate of occupational fatigue among nurses in the present study, while in the studies by Saki et al. (41) and Saremi and Fallah (42), 47.61 and 59% of nurses reported feeling tired, respectively, which seems to be due to long term of dealing with patients, different work departments, long shifts, low staffing in hospital wards, and high workload. Also, in the study by Sabokro et al., it was shown that occupational fatigue affected the procrastination of nurses and reduced productivity, causing physical and psychological complications in them (43).
The results of the study also showed no significant relationship between occupational fatigue and education level, which was not in line with the findings of Javadpour et al. (44), Halvani et al. (45), and Azad et al. (21). Beurskens et al. reported that people without a college education were more likely to perceive fatigue (46). Similar to this study’s findings, occupational fatigue was higher in people with lower education. Also, the findings of the study showed no significant relationship between occupational fatigue and job satisfaction. However, it should be noted that the job satisfaction of nurses in different medical centers is different and research findings cannot be easily generalized to other centers because differences in styles of leadership, communication, promotion system, and other components can affect the nurses' perceptions and job satisfaction. In the study by Habibi et al. (47), it was shown that the rate of occupational fatigue had a significant relationship with gender so that the rate of occupational fatigue was higher in men than in women, which is consistent with the present study in terms of occupational fatigue and gender, but in the present study's occupational fatigue and dimensions of general fatigue, physical fatigue was more in women than in men, which can be one of the reasons that in addition to anthropometric characteristics of women compared to men and their lower ability to withstand work stress, endure work activity during everyday life and marital worries may be more.
In the study by Karimi and Honarbakhsh (25), occupational fatigue did not show a significant difference between marital status and the educational group, which was in line with the present study. In the present study, the difference in occupational fatigue between married people and single people was found to be significant so that occupational fatigue was more in married people than in single people. It should be noted that the study by Karimi and Honarbakhsh (25) was conducted among people who were truck drivers, and this difference between the two studies could be due to this issue. In the present study, it was found that age was a factor affecting occupational fatigue so that occupational fatigue increased with increasing age. The study by Hosseini et al. showed that occupational fatigue is important in nurses, so it is recommended to improve their job performance by modifying the causes of burnout, ultimately increasing the quality of nursing care and patient satisfaction (48).
One of the limitations of the research was the small sample size. Therefore, its ability to be extended to other hospitals in the country is limited.
5.1. Conclusion
Based on the results of this study, it was found that increasing the safety climate can reduce employees’ job fatigue; this shows that their job fatigue, which includes mental fatigue, decreased motivation, and reduced activity, will be reduced if the employees have common ideas about how to manage safety and the real priority of safety in the workplace and they have confidence in how to manage safety in the workplace. Also, the findings of this study showed that among the demographic variables, second job, age of nurses, and shift work had a significant effect on their job fatigue. Also, reducing fatigue can increase the safety climate of nurses.
It is suggested that deeper relationships be found between the research variables by using the dependent variables in the studies and by using the existing conceptual models in the field of the relationship between general health and quality of life.
