






1. Background
Prostate cancer is the second leading cause of cancer death in men worldwide (1-3). The disease is more common in African men than in other races (4). According to the American Cancer Society (2020), about 191,930 new cases of prostate cancer are diagnosed in men, and 33,330,000 cases would die from the disease (5). The Age-Standardized Incidence Rate (ASR) of this disease among Iranian men is reported to be 21.42 per 100,000 persons (6). Khuzestan province is also in the first rank regarding the prevalence of cancers in men with an average age of 23.36 years, and the frequency of cases in the male population is 2529 persons, with a prevalence rate of 31% according to the latest report of the Cancer Statistics Centre. Accordingly, prostate cancer is a major concern worldwide and in Iran (7). Prostate cancer is more common in middle-aged and older men, with > 75% of new cases diagnosed in men aged above 61 years (8, 9). Since the disease is asymptomatic in the early stages, most symptoms indicate localized or metastatic advanced disease (10). However, some risk factors of prostate cancer are racial differences, genetic and environmental factors, family history, aging-related hormonal changes, infection, poor nutrition, physical inactivity, smoking, and alcohol consumption, vasectomy, and sexually-transmitted infections (STIs), some of which can be changed and prevented (10, 11). Prostate cancer mortality and proper treatment in the early stages have highlighted the significance of early diagnosis (12).
There are disagreements about the timing of prostate cancer screening. The American Urological Association (AUA) recommends men aged above 40 years with a life expectancy of at least 10 years to perform prostate cancer screening (13, 14); however, the American Prostate Cancer Society (ACS) recommends men aged above 50 years with a life expectancy of at least 10 years to do screening (14, 15). The U.S. Preventive Services Working Group (USPSTF) states that screening should not be performed in individuals aged 75 years and above due to increased risk and reduced screening benefits (14, 16). Accordingly, men aged 40 - 75 years are the most suitable target group for prostate cancer screening (15, 17).
Screening and the early diagnosis of prostate cancer allow for the initial classification of the disease, prognosis, and treatment before reaching the advanced stages (18). Prostate cancer screening is a search to identify individuals with prostate cancer on a large scale and asymptomatic cases (1). Prostate cancer screening principles include prostate-specific antigen (PSA) (19) and digital rectal examination (DRE) (20). Digital rectal examination is the oldest and cheapest test. Before the discovery of PSA, it was the first and the only diagnostic tool used to detect prostate cancer until the mid-1980s (21).
Prostate-specific antigen is the most commonly used and the simplest screening test (22). The early detection of prostate cancer using PSA blood tests and timely treatment allow for the eradication of prostate cancer and the prevention of metastasis (8). The PSA screening reduces the number of men with metastatic disease by about 70% and significantly decreases costs imposed on healthcare systems by reducing complications (22). Cancer prevention and early detection are critical factors in controlling the disease and increasing patient survival. Choosing a health education model is the first step in planning for education and behavior change (11). Health Belief Model (HBM), developed by Hochbham and Rosenstock in the 1950s for health education professionals, encompasses the following dimensions: Perceived susceptibility to disease, perceived severity, perceived barriers, perceived benefits, self-efficacy, and cue to action (23). According to this model, individuals should believe that the disease can exist without symptoms. Individuals are more likely to perform this behavior when they consider themselves at risk for the disease (perceived susceptibility), perceive that the disease has serious consequences (perceived severity), and believe that preventive action has a positive outcome (perceived benefits), that the barriers to that behavior are fewer than its benefits (perceived barriers), and that they are capable of performing health behaviors (self-efficacy). Health Belief Model is one of the most accurate and important models used to predict health-related behaviors (11, 24, 25). The model is underpinned by this theory that individuals’ willingness to change their health behavior is primarily due to their health perceptions. The growing cancer rate in Iran, the lack of referral until the disease reaches the advanced stage, not participating in screening programs, and poor awareness of prostate cancer screening behavior (10, 11) indicate the need for promoting men's sensitivity to the adoption of prostate cancer screening behavior.
2. Objectives
Accordingly, the present study aimed to perform prostate cancer screening behavior according to the Health Belief Model for men aged above 40 years.
3. Methods
This cross-sectional study encompassed 120 male employees aged above 40 years working at the Dezful University of Medical Sciences in 2018.
The sample size estimate was based on 80% power for detecting a significant relationship of 0.37 with a significance level of α = 0.05 and a 10% loss to the follow-up rate. The sample size formula is:
The participants were selected using the multi-stage sampling method. In the first stage, out of eight departments of the Dezful University of Medical Sciences, four departments were selected using the random cluster sampling method. According to the registered file of the employees, 30 men aged above 40 years from each department were included using the sample random sampling method and according to a table of random numbers (n = 120). Inclusion criteria were willingness to participate in the study, completing the written informed consent form, no history of prostate cancer, benign prostatic hyperplasia with obvious clinical symptoms, and aged above 40 years. The only exclusion criterion was unwillingness to participate in the study.
The data collection tool was a researcher-made questionnaire developed based on previous studies (26). This questionnaire consisted of four sections. The first section included questions on demographic factors (four items about age, occupation, and others) and the second section encompassed items on performance cancer screening behavior, scored using yes (score 1) and no (score 0) options.
The third section of the questionnaire (awareness questions) was scored using 1 for correct and 0 for incorrect responses and unanswered items (0 - 12).
A panel of experts from the Dezful University of Medical Sciences, including ten specialists in health education, urology, oncology, preventative medicine, and nursing, confirmed the validity of the data collection tools by determining the content validity ratio and the content validity index.
Considering the cut-off point, the content validity of the questionnaires was determined using CVI and CVR. Higher scores indicate the higher levels of knowledge about prostate cancer. The estimated reliability screening behavior of the knowledge scale was 0.75, indicating the internalization compatibility of this questionnaire.
The fourth section consisted of questions developed based on the HBM constructs (n = 32): Perceived susceptibility (3 questions), perceived barriers (11 questions), perceived severity (3 questions), and perceived self-efficacy (6 questions), and cue to action (4 questions). A 5- point Likert scale (strongly agree (5), agree (4), no idea (3), disagree (2), strongly disagree (1)) was also used to answer the questions in the fourth section.
The internal and external consistency coefficients of the questions were determined by estimating Cronbach's alpha and test-retest coefficients, respectively, for 30 individuals in two stages with a two-week interval to evaluate the reliability of the questionnaire. It should be mentioned that these individuals were not included in the study. Cronbach's alpha coefficients of perceived susceptibility, severity, barriers, benefits and self-efficacy, and cue to action were 0.71, 0.89, 0.84, 0.71, 0.82, and 0.71, respectively.
The Statistical Package for the Social Sciences (SPSS) version 19 was used to analyze the collected data. The quantitative data are described as mean, standard deviation, and frequency. Independent t-test and regression analysis were used to examine the relationship among the variables. In this study, P < 0.05 was set as the significance level.
3.1. Ethical Considerations
This study was approved by the Ethics Committee affiliated with the Dezful University of Medical Sciences (Ethics Code: IR.DUMS.REC.1395.12). In this study, the researchers were committed to the ethical issues of obtaining informed consent from the participants, respecting for voluntary participation, and informing the participants of the research objectives.
4. Results
The participants’ mean age was 46.22 ± 4.56 years (range: 40 - 60 years). Most of the participants (33.7%) had academic education and were married (92.5%).
The participants’ level of knowledge was 28.8%, and there was no statistically significant difference between knowledge and screening behavior (P < 0.19).
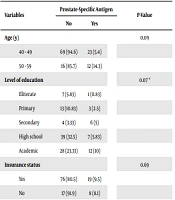
The performance of the PSA test was 20% among the study participants. Moreover, the chi-squares test revealed no significant relationship between education and the PSA test (P < 0.07), indicating that the higher the level of education, the higher the screening performance. Thirteen respondents had a family history of prostate cancer. There was a significant relationship between the participants’ history of cancer and the PSA test (P < 0.59). Individuals with a positive family history of cancer are more likely to engage in screening behaviors (Table 1).
| Variables | Prostate-Specific Antigen | P-Value | |
|---|---|---|---|
| No | Yes | ||
| Age (y) | 0.09 | ||
| 40 - 49 | 69 (94.6) | 23 (5.4) | |
| 50 - 59 | 16 (85.7) | 12 (14.3) | |
| Level of education | 0.07 * | ||
| Illiterate | 7 (5.83) | 1 (0.83) | |
| Primary | 13 (10.83) | 3 (2.5) | |
| Secondary | 4 (3.33) | 6 (5) | |
| High school | 39 (32.5) | 7 (5.83) | |
| Academic | 28 (23.33) | 12 (10) | |
| Insurance status | 0.69 | ||
| Yes | 76 (80.5) | 19 (9.5) | |
| No | 17 (91.9) | 8 (8.1) | |
| Marital status | 0.27 | ||
| Single | 9 (95.5) | 1 (0.5) | |
| Married | 76 (70.1) | 34 (24.9) | |
| History of cancer | 0.59 * | ||
| Yes | 5 (5.6) | 8 (94.4) | |
| No | 77 (90.8) | 30 (9.2) | |
| Awareness | 0.19 | ||
| Acceptable | 19 (22.8) | 8 (9.6) | |
| Average | 48 (57.6) | 18 (21.6) | |
| Weak | 24 (28.8) | 3 (3.6) | |
Relationship Between Prostate Screening Behaviors and Demographic Variables in Men Aged Above 40 Years (n = 120) a
Among the HBM constructs in the present study, the participants had a relatively optimal perceived barriers and susceptibility; however, their perceived severity, benefits, self-efficacy, and cue to action were unacceptable. For those with PSA and those not adopting screening behaviors, the independent t-test showed a statistically significant difference between the two groups regarding the perceived barriers (P = 0.001).
It would seem that men who are aware of preventative behaviors, perceive that their prostate cancer is more pronounced. It is not an indicator of actual poor health.
That is, it is inversely correlated with the adoption of prostate cancer screening behaviors (Table 2).
| Variables | Values | Have Prostate-Specific Antigen | Do Not Have Prostate-Specific Antigen | Minimum | Maximum | P-Value |
|---|---|---|---|---|---|---|
| Perceived sensitivity | 6.8 ± 2.21 | 10.24 ± 2.44 | 9.55 ± 2.26 | 3 | 11 | 0.09 |
| Perceived severity | 7 ± 3.52 | 7.55 ± 2.26 | 7.76 ± 3.55 | 3 | 15 | 0.63 |
| Perceived benefits | 11.42 ± 4.75 | 23.35 ± 2.91 | 23.17 ± 3.21 | 5 | 52 | 0.74 |
| Perceived barriers | 35.42 ± 7.42 | 41.34 ± 9.07 | 34.37 ± 8.11 | 15 | 55 | 0.00* |
| Self-efficacy | 17.68 ± 4.95 | 6.55 ± 3.26 | 6.55 ± 3.26 | 6 | 30 | 0.19 |
| Cues to action | 6.55 ± 3.26 | 12 ± 3.26 | 10.95 ± 4.23 | 4 | 20 | 0.15 |
Descriptive Measures of Health Belief Model Constructs of Prostate Cancer Screening Behaviors in Men at the Dezful University of Medical Sciences (n = 120) a
Table 3 shows the results of the logistic regression analysis of the variables. According to the results, perceived sensitivity and the consequence of prostate cancer were the psychological predictors of prostate cancer screening behaviors among men aged above 40 years (P = 0.001).
| Step /Variables | B | S.E. | OR, Exp (B) | P-Value |
|---|---|---|---|---|
| Awareness | 0.01 | 0.098 | 1.01 | 0.89 |
| Perceived sensitivity | -0.08 | 0.03 | 0.92 | 0.01 |
| Perceived severity | 0.01 | 0.08 | 0.95 | 0.90 |
| Perceived benefits | -0.02 | 0.08 | 0.97 | 0.74 |
| Perceived barriers | -0.04 | 0.09 | 0.92 | 0.53 |
| Cues to action | -0.00 | 0.06 | 0.99 | 0.89 |
| Level of education | 0.48 | 1.89 | 1.61 | 0.80 |
Prediction of Independent Variables to Prostate Cancer Screening Behaviors Using Logistic Regression (n = 120)
5. Discussion
The present study aimed to predict prostate cancer screening behaviors in the male employees at the Dezful University of Medical Sciences according to HBM in 2018. Regarding the status of prostate cancer screening behaviors among the male employees of the Dezful University of Medical Sciences, the findings showed that a highly small percentage of the participants performed DRE and PSA and had low performance in this regard. This finding is consistent with the findings reported by Ebuehi and Otumu (1), Barati et al. (8), Ezenwa et al. (19), and Chiu et al. (26). However, the frequency of prostate cancer screening behaviors was 50% in previous studies conducted by Woolf et al. (27), Gorin and Heck (28), van Leeuwen et al. (29), and Negnevitsky (30). Considering the significance of the PSA test in disease prevention and early detection and the poor performance of Iranian men, there is a need to train and use appropriate training methods to increase their awareness. It is also important to consider the barriers to screening, including financial problems, access to screening services, insurance, and easy access to healthcare centers. These centers play an influential role in screening as such they should be considered in planning and health strategies.
In this study, the participants’ knowledge of prostate cancer and screening behaviors were poor. Consistent with the present study, Barati et al. (8), Zahir et al. (12), and Akbarizadeh et al. (24) showed a low level of awareness among their participants. In this regard, sufficient awareness and knowledge about prostate cancer predict screening behaviors, indicating that with promoting knowledge and awareness, prostate cancer screening behaviors also increase. Knowledge seems to play a crucial role in men's performance in training programs on the benefits of screening behavior.
It also plays a critical role in promoting prostate cancer screening behavior.
This study revealed a positive correlation between the perceived susceptibility and the frequency of the PSA test. This finding is consistent with the findings of similar studies by Abuadas et al. (25), Chiu et al. (26), and Zahir et al. (12). These findings, however, are inconsistent with those reported by Negnevitsky (30) and Barati et al. (8). This difference may be caused by the fact that, given the hidden nature of prostate cancer, individuals may assume that they are at highly low risk of the disease and its complications. However, most men aged above 40 years are at risk.
The present study demonstrated a non-optimal mean score of perceived severity for the prostate cancer. In line with the present study, Barati et al. (8) and Abuadas et al. (25) reported moderate to low scores of perceived severity for the prostate cancer. Perceived severity means that individuals know the serious and potential consequences of the disease, and this should be included in planning, training, and awareness-raising interventions designed for men. The mean score of the perceived benefits suggested that the participants did not believe in the importance and benefits of prostate cancer prevention behaviors.
In a similar vein with the present study, Barati et al. (8) and Aflakseir (31) showed that participants had little trust in the benefits of prostate cancer screening behaviors. However, Shao et al. (32), Sharifirad et al. (33), and Zare et al. (34) showed that the benefits of prostate cancer screening behaviors have been of great importance to men. This was not consistent with the findings of the present study.
This difference may indicate that the training programs implemented at the comprehensive health centers pay not much attention to the benefits of prostate cancer screening behaviors. Moreover, the male target group may have little awareness of the benefits of screening. Accordingly, the importance of such behaviors should be further highlighted.
Furthermore, the mean score of perceived barriers is high in the present study, indicating that there are more barriers to performing health measures such as unawareness of the place, time, and procedure of diagnostic tests, misbeliefs about the unnecessity of referring to a physician due to being asymptomatic, and finding DRE embarrassing. Accordingly, more barriers felt by men make them perform prostate cancer screening behaviors less frequently. The findings of the present study are consistent with those reported by Barati et al. (10), Abhar et al. (11), and Oliver et al. (35). Accordingly, this issue requires and the further attention of health officials and policymakers to adopt preventive measures.
The present study reported undesirable perceived self-efficacy for prostate cancer screening behaviors, indicating individuals’ weak ability to adopt healthy behaviors and remove barriers ahead. This finding is consistent with the findings of similar studies (10, 31). However, Masoudiyekta et al. (22), Shao et al. (32), and Arli and Bakan (36) showed that self-efficacy plays a critical role in promoting cancer prevention behaviors. This difference may be due to the lack of self-confidence, awareness, or health determinants such as cultural or social issues. More efforts should be made to increase men's self-efficacy in Iranian society to manage chronic diseases.
Internal cue to action guides individuals internally to perform cancer screening behaviors and makes them feel responsible for their health. The present study reported a low score for the cue to action, which is consistent with the findings of Massoudi Yekta et al. (23) and Barati et al. (8) and in contrast with the findings reported by Shao et al. (32), Zare et al. (34), and Arli and Bakan (36). This may represent inadequate public knowledge on prostate cancer screening. Moreover, the participants are likely to adopt a cue to action; however, they may believe that that the cue to action is not powerful enough to help them adopt screening behaviors.
Further attention should be paid to prostate cancer screening behaviors among the male employees in Dezful. Among the HBM constructs, perceived susceptibility is the most important predictor of the PSA test. In this regard, the risk of prostate cancer for men should not be ignored. If left untreated, these conditions can endanger the lives of men, resulting in the death of our fathers, spouses, and brothers. Screening and early detection should be performed for men suffering from this disease to make prostate cancer treatment more effective. To improve men's health status, it is recommended to highlight the prevention of prostate cancer while designing and implementing training programs.
