

1. Background
Breast cancer accounts for almost one-third of all cancers in women, and after lung cancer, it has the highest mortality rate; breast cancer has the highest incidence rate among all cancers (1) and is the second most common cancer and the most common cancer in women (2).
Cancer patients suffer intense pain, and patients with more advanced cancers suffer severe pain due to the disease or treatments. Naturally, physical pain can lead to experiencing psychological distress (2).
Although many cancers are curable, cancer patients' psychological, emotional, and social needs are often neglected. Cancer with psychological stressors severely damages patients' quality of life (3). The side effects of treatments and disruptions in career and life goals, economic problems, changes in social relations, the possibility of negative psychological states, and uncertainty about the future are important stressors for these patients. The type of cancer, increase in pain, decrease or inability of body functions, and increase in fatigue related to cancer (CRF) play a key role in lowering the quality of life of cancer patients (4). Only a few studies have examined the effectiveness of acceptance and commitment-based therapy (ACT) techniques in the psychotherapy of cancer patients; among them are the studies by Hulbert-Williams et al., which found ACT to be an effective treatment approach (5). The results of other research in the treatment field based on acceptance and commitment demonstrated that the components of this treatment lead to psychological flexibility in cancer patients, which leads to changes in their quality of life and suffering (6).
Acceptance and commitment therapy is a behavioral therapy that uses mindfulness, acceptance, and cognitive dissonance to increase psychological flexibility (7). In therapy based on acceptance and commitment, psychological flexibility means improving the ability of therapy seekers to relate to their experiences in the present, as well as what is possible for them at this time, to choose to act in a way that is based on be their own chosen values (8). Because cancer requires education to adapt to the disease, psychological skills play an important role in achieving this goal, especially in treatment based on acceptance and commitment that does not see patients as defeated and hopeless. Rather, this treatment is an increasing capability that makes life by values complete and meaningful available to clients. The absolute of success is not defined but can be an increasing choice, which includes the present in the direction of a valuable life, which can be therapeutic (9). For this reason, treatment based on acceptance and commitment can be considered as one of the appropriate and desirable interventions to improve the capabilities of cancer patients in adapting to crises and daily stresses, reducing the amount and intensity of pain, and improving their quality of life.
2. Objectives
The importance and necessity of this research will clarify the effectiveness of acceptance and ACT on pain and quality of life in breast cancer patients.
3. Methods
This research was semi-experimental with a pre-test and post-test design and a control group with random assignment in two experimental and control groups. The statistical population was 235 patients with breast cancer who had been referred to Imam Hassan Mujtaba specialty clinic in Dezful for treatment in 2018 and were undergoing treatment. For the research, 30 willing participants were selected voluntarily and completed the consent form. The conditions for selecting people were to be less than 60 years old, not in the final stages of the disease, and have at least a diploma. Participants were randomly assigned to two experimental and control groups. First, all participants completed the pre-tests of the brief pain questionnaire and the quality-of-life questionnaire. Then, the experimental group received the treatment intervention program based on commitment and acceptance. At the end of the sessions, both groups completed the tests again. The control group was assured that if the intervention were effective, they would receive treatment sessions based on commitment and acceptance.
3.1. Tools
3.1.1. Brief Pain Severity Questionnaire
This questionnaire was created by Cleeland in 1991 to measure the intensity of chronic pain in cancer patients and other patients suffering from chronic pain (10). This questionnaire consists of 2 main parts: measuring pain intensity, the level of interference in daily affairs, and background questions. The sensory section includes 4 questions (2-4, 6) that measure recent pain intensity, minimum pain, worst pain, and average pain during the past week. These substances are scored from zero (absence of pain) to ten (unimaginable). The higher the score, the more severe the pain. The part that measures pain interference with general daily functions (reactive dimension) consists of a 7-part question (10). This questionnaire has been standardized by Mirzamani et al. (11). Also, Vakilzadeh and Nakhaee (12) evaluated the reliability and validity of this questionnaire for cancer patients. Cronbach's alpha for the dimensions of pain intensity and response were 0.87 and 0.89, respectively, and the construct validity of the questionnaire was reported as 0.87. Cronbach's alpha obtained for the dimensions of pain intensity and interference in this study were 0.83 and 0.81, respectively
3.1.2. Quality of Life Questionnaire
This is the third edition of the special questionnaire for measuring the quality of life in cancer patients developed by the "European Organization for Research and Treatment of Cancer" and prepared by Arnson. This questionnaire has 30 questions and three areas: functional area including physical function (questions 5 to 1), role-playing (questions 6 and 7), emotional function (questions 24 to 21), cognitive function (questions 20 and 25) and social (questions 26 and 27) and symptoms area including fatigue (questions 18, 12, 10), pain (questions 9 and 19), nausea and vomiting (questions 14 and 15), shortness of breath (question 8), diarrhea (question 17), constipation (question 16), loss of sleep (question 11), loss of appetite (question 13), economic problems caused by received treatments (question 28), and general area of quality of life (questions 29 and 30). Validation studies have confirmed this questionnaire as a valid and reliable scale for the quality of life of cancer patients in multicultural research situations (13). Safaee et al. reported that the third edition of the Persian version of this questionnaire is reliable and valid for measuring cancer patients' quality of life. Cronbach's alpha of the fatigue scale is 0.65, pain is 0.69, nausea and vomiting is 0.66, and the other scales are estimated above 0.70, indicating this questionnaire's good reliability (13). Also, the calculated Cronbach's alpha value of the questionnaire dimensions in this study fluctuated between 0.68 and 0.79 (14).
3.1.3. Acceptance and Commitment Group Therapy Protocol
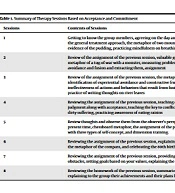
The intervention based on acceptance and commitment was held for eight 90-minute weekly sessions. Designed by the researcher and executed, this treatment is based on eight therapy sessions based on ACT on six central therapeutic processes in ACT: present moment, diffusion, acceptance, self as background, values, and committed action (Table 1).
| Sessions | Contents of Sessions | Homework |
|---|---|---|
| 1 | Getting to know the group members, agreeing on the day and time of the sessions, describing the general treatment approach, the metaphor of two mountains and an ugly plant and evidence of the pudding, practicing mindfulness on breathing and the five senses | Mindfulness practice |
| 2 | Review of the assignment of the previous session, valuable goals and their obstacles, the metaphor of a tug-of-war with a monster, measuring problems and explaining experiential avoidance and fusion and extracting them, assignment | Completing the worksheet of the ways used and the long-term effects |
| 3 | Review of the assignment of the previous session, the metaphor of struggling in the sand, identification of experiential avoidance and constructive frustration towards the ineffectiveness of actions and behaviors that result from fusion and experiential avoidance, the practice of writing thoughts on river leaves | Crochet and Target Loop Worksheet |
| 4 | Reviewing the assignment of the previous session, teaching observation of thoughts without judgment along with acceptance, teaching the key to conflict and explaining clean pain and dirty suffering, practicing awareness of eating raisins | Raisins worksheet and measuring its amount |
| 5 | Review thoughts and observe them from the observer's perspective, connection with the present time, chessboard metaphor, the assignment of the previous session, familiarization with three types of self-concept, and dimension training. | Raisins vs. giving space worksheet |
| 6 | Reviewing the assignment of the previous session, explaining life's values and characteristics, the metaphor of the compass, and celebrating the 80th birthday. | Writing values and meditating on them |
| 7 | Reviewing the assignment of the previous session, providing practical solutions to remove obstacles, setting goals based on your values, explaining the characteristics of smart goals | Recording the worksheet of the intention and action plan |
| 8 | Reviewing the homework of the previous session, summarizing the reviewed concepts, and explaining to the group their achievements and their plans for continuing their lives. |
Summary of Therapy Sessions Based on Acceptance and Commitment
4. Results
This study was conducted on 30 women with breast cancer undergoing treatment in two experimental and control groups. The results of the demographic data showed that the average age of the experimental (44.73) and control groups (45.13) was almost equal. In the demographic variable, the level of education in the experimental and control groups was the highest for diploma degrees and the lowest for Master's degrees.
The descriptive data in Table 2 shows differences between the average of the variables in the 2 experimental and control groups in the pre-test and post-test stages.
| Variables and Groups | Experiment | Control | ||
|---|---|---|---|---|
| Pre-test | Post-test | Pre-test | Post-test | |
| Brief severity of pain | ||||
| Severity component | 25.60 ± 12.65 | 19.60 ± 10.33 | 29.33 ± 13.33 | 29.13 ± 12.16 |
| Interference in everyday components | 37.33 ± 19.48 | 27.66 ± 15.12 | 39.46 ± 14.87 | 38.20 ± 15.16 |
| Quality of life | ||||
| Functional area | 31.66 ± 6.83 | 23.86 ± 3.85 | 32.13 ± 4.95 | 31.46 ± 5.05 |
| Symptom area | 24.40 ± 3.64 | 17.53 ± 3.22 | 23.46 ± 3.27 | 19.06 ± 3.91 |
| Global area | 8.80 ± 2.85 | 10.60 ± 2.66 | 6.93 ± 3.39 | 5.86 ± 1.55 |
Descriptive Finding of the Pain Severity and Quality of Life in Two Experimental and Control Groups
The assumptions for using covariance analysis have been established, which include normality and equality of variance in both experimental and control groups, as well as a linear relationship between the independent and dependent variables in all subscales of pain intensity and quality of life.
The results of covariance analysis showed that the pre-test score in the pain intensity component had a relationship of 0.93 with the post-test scores (P < 0.05). By controlling these significant relationships, it was determined that the difference between the adjusted averages of the pain intensity component of the experimental group was 21.16, and the control group was 27.56, which was statistically significant (P < 0.05). Also, the pre-test score of interference daily had a relationship of 0.89 with the post-test scores (P < 0.05). By controlling these significant relationships, it was determined that the difference between the adjusted averages of the interference in the day area of the experimental group was 28.54 and 37.31, statistically significant (P < 0.05) (Tables 3 and 4).
| Variable and Components | F | Sum of Square | df | P-Value | Effect Size | Power of Test |
|---|---|---|---|---|---|---|
| Brief pain severity | ||||||
| Pain severity | 410.15 | 3347 | 1 | 0.001 | 0.93 | 1 |
| Interference in everyday affairs | 232.95 | 5754.74 | 1 | 0.001 | 0.89 | 1 |
The Results of the Covariance Test in the Components of Pain Severity
| Experiment, Mean ± SD | Control, Mean ± SD | |
|---|---|---|
| Severity of pain | 21.16 ± 0.74 | 27.56 ± 0.74 |
| Interference in everyday life | 28.54 ± 1.28 | 37.31 ± 1.28 |
Adjusted Means of Pain Component in Experiment and Control Groups
According to the adjusted averages of pain intensity and interference in daily life in two groups in the post-test stage, it can be concluded that in the treatment group, intervention based on acceptance and commitment significantly reduced the two components of pain intensity in breast cancer patients. The effect size of the test also shows that this intervention caused a reduction of 0.93 and a reduction of interference in daily affairs by 0.89 in the components of pain intensity in the post-test stage.
The results of covariance analysis showed that the pre-test score in the functional area of quality of life has a relationship of 0.93 with the post-test scores (P < 0.05). By controlling these significant relationships, the difference between the adjusted averages of the functional area of the experimental group was 23.99, and the control group was 31.33, which was statistically significant (P < 0.05) (lower average indicates better performance).
However, in the other component of quality of life, which is the area of symptoms, the results of covariance analysis showed that the pre-test score of the area of symptoms had a relationship of 0.60 with the post-test scores (P < 0.05). By controlling these significant relationships, it was determined that the difference between the adjusted averages of the symptom area in the experimental group was 17.10, and the control group was 19.49, which was statistically significant (P < 0.05) (lower mean indicates a reduction in symptoms shows).
Also, in the general field of quality of life, the covariance analysis results showed that the general field's pre-test score had a relationship of 0.60 with the post-test scores (P < 0.05). Controlling these significant relationships determined that the difference between the adjusted averages of the overall range in the experimental group was 10.09, and in the control group was 6.37, which was statistically significant (P < 0.05) (Tables 5 and 6).
| Variable and Components | Sum of Square | df | Mean of Square | F | P-Value | Effect Size | Power of Test |
|---|---|---|---|---|---|---|---|
| Quality of life | |||||||
| Functional area | 318.35 | 1 | 318.35 | 34.78 | 0.001 | 0.56 | 1 |
| Symptom area | 217.18 | 1 | 217.18 | 40.85 | 0.001 | 0.60 | 1 |
| Global area | 80.27 | 1 | 80.27 | 40.84 | 0.001 | 0.60 | 1 |
The Results of the Covariance Test in the Components of Quality of Life
| Variables | Experimentm, Mean ± SD | Control, Mean ± SD |
|---|---|---|
| Functional area | 23.99 ± 0.78 | 31.33 ± 0.78 |
| Symptom area | 17.10 ± 0.59 | 19.49 ± 0.59 |
| Global area | 10.09 ± 0.37 | 6.36 ± 0.37 |
Adjusted Means of Quality of Life in Experiment and Control Groups
Based on these results, group therapy based on acceptance and commitment significantly increased the quality of life in breast cancer patients. The effect size shows that this intervention increased the quality of life in the post-test.
5. Discussion
The present study was conducted to assess the effectiveness of acceptance and ACT on pain and quality of life in breast cancer patients. In response to the first research hypothesis that treatment based on acceptance and commitment would reduce pain in cancer patients, the results demonstrated a significant difference between the experimental and control groups in the pre-test and post-test. Based on these findings, it can be concluded that the treatment based on acceptance and commitment reduced the severity of pain in breast cancer patients. This finding is in line with the results of research conducted in this field, including the research of Wurtzen et al. (15), Hoffman et al. (16), Lengacher et al. (17), Henderson et al. (18), Kim et al. (19), Dehghani et al. (20), Brown and Ryan (21), and Mousavi et al. (22). The present study showed that the treatment based on acceptance and commitment effectively reduced pain intensity in breast cancer patients and improved their quality of life. According to research evidence, treatment based on acceptance and commitment effectively reduced pain intensity, and this treatment can reduce chronic pain. Pain is a serious problem for patients, spouses, and other family members. Research shows that the wife's reaction to the patient can be effective in her ability to cope with pain (23).
In explaining the second hypothesis of the research, that is, the effectiveness of treatment based on acceptance and commitment to the quality of life in patients with breast cancer, the evidence showed that this treatment was effective in increasing the quality of life of patients. In this regard, the research results of Feros et al. indicated that treatment based on acceptance and commitment increased psychological flexibility and improved distress, mood, and quality of life (6).
From the point of view of therapy based on acceptance and commitment, the primary source of problems in therapy seekers is their psychological flexibility. Limited options for behavior make a person feel trapped and conflicted. Acceptance and commitment therapy emphasizes the benefit of psychological flexibility, that is, having behavioral options available. This occurs when a person consciously accepts their troubling thoughts and feelings, behaves in the same direction, and shows consistency with their values. This happens in the treatment based on acceptance and commitment using different experimental, metaphorical, and second-degree change methods. Psychological inflexibility persists through six main interconnected processes: cognitive fusion, dependence on self-concept, experiential avoidance, lack of connection with the present, uncertain values, and weakness in respect for values. This research showed that the severity of chronic pain was reduced. The quality of life of cancer patients was increased due to psychological flexibility, which is a treatment based on acceptance and commitment using cognitive delusion, separation, and separation of self-concept, experiential acceptance, conscious contact with the present, clear and specific values, and action and commitment based on values create it. The results and achievements of the research showed the effectiveness of psychological and supportive interventions in improving the quality of life of people living with breast cancer (4, 24). Despite the importance of the third wave of cognitive-behavioral therapies, including the approach based on acceptance and commitment, they have been announced as an important area of modern therapy, and research shows their influential role in improving the quality of life (25). Only a few researchers have examined the application of ACT techniques in the psychotherapy of cancer patients, including the research of Hulbert-Williams et al. (5), who found the ACT approach effective in coping with cancer. The results of other research in the field of acceptance and commitment-based treatment demonstrated that the components of this treatment promote psychological flexibility in cancer patients, which can improve the quality of life and alleviate the suffering of patients (6).
Research findings on mindfulness as the core concept of treatment based on acceptance and commitment indicate that cancer stress management based on acceptance and awareness reduced the psychological suffering of breast cancer patients and increased their quality of life and mental health (26).
This therapy teaches people to accept what they cannot change and what is out of their control and commit to action that makes their lives meaningful and complete. This treatment aims to help patients build a rich, complete, and meaningful life based on their values and to see the pain and suffering of life as an integral part of their lives (8).
According to the results of the present study, this treatment method can be used as a selective and complementary psychotherapy to reduce pain intensity and increase cancer patients' quality of life. This can lead to information and enthusiasm of the relevant specialists to the psychological aspects of treatment and stimulate them to attach more importance to this aspect in breast cancer patients. The outcomes can significantly impact the treatment and recovery process. In addition, from a social and economic point of view, this can have additional positive results and benefits.
