

1. Background
Gallstone disease, traditionally stereotyped as affecting primarily 'fair, fat, fertile, 40-year-old females,' is not confined to this demographic (1-7). While gallstone disease often remains asymptomatic until later stages of life (7, 8), Western literature reports that a significant percentage, ranging from 4 - 20%, of cholecystectomies is performed on individuals under the age of 30 (6).
The inherent risk factors associated with gallstones include unchangeable elements such as gender (with females being more susceptible than males), age (prevalent in adults), and familial or ethnic predispositions. In contrast, modifiable factors such as obesity, metabolic syndromes, rapid weight loss, and certain medical conditions like cirrhosis, Crohn’s disease, and gallbladder stasis can be addressed through treatment. Notably, high caloric intake is the only known dietary risk factor. Diets rich in fiber, vegetable proteins, nuts, calcium, vitamin C, coffee, and alcohol, along with regular physical activity, may help prevent gallstone formation (8, 9).
Surgery is rarely necessary for asymptomatic cholelithiasis. However, individuals with large gallstones (> 2.50 cm), congenital hemolytic anemia, non-functioning gallbladders, or those undergoing bariatric surgery or colectomy may require a prophylactic cholecystectomy (8, 10). Our recent observations indicate an increasing trend of laparoscopic cholecystectomy among teenagers and young adults at our facility. This apparent surge prompted a retrospective observational study to investigate the prevalence of gallbladder disease in individuals aged 15 - 40 years. Understanding the evolving landscape of gallstone disease in younger populations is crucial for tailoring preventive strategies and optimizing management approaches.
2. Objectives
This study explores the prevalence and potential risk factors associated with gallstone disease in this younger age group, shedding light on the dynamic nature of this condition in contemporary healthcare.
3. Methods
This observational study was conducted at the Department of General Surgery at Al Wahda Teaching Hospital, Derna, Libya, from January 2021 to January 2022. The study focused on patients with gallbladder disease-related admissions or operations, totaling 182 individuals.
3.1. Data Collection
Data were collected retrospectively from inpatient records and the operating room at the Department of General Surgery. Demographic information, including age, gender, and body mass index (BMI), was recorded. Additionally, modifiable risk factors such as dietary habits, reproductive history, smoking, and associated chronic illnesses were documented.
3.2. Data Analysis
Microsoft Excel (Microsoft, Redmond, WA, USA) was used for data collection and analysis. Categorical data were presented as percentages to provide a comprehensive understanding of the distribution of various factors among the patient population. This approach facilitated the identification of patterns and trends related to gallbladder disease and its risk factors within the study cohort.
4. Results
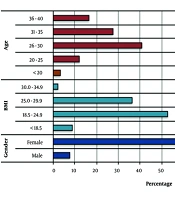
In this study, we examined the demographic characteristics of the study population, focusing on sex, age distribution, and BMI. Figure 1 illustrates the distribution of these demographic variables, providing valuable insights into the composition of the cohort and shedding light on key factors that may influence gallstone formation.
 in the study population. The most common categories within each dataset were highlighted. Females are the predominant gender (92.3%), with the age group of 26 - 30 years being the most commonly affected. The average weight population, as indicated by a BMI range of 18.5 - 24.9, is predominantly affected, accounting for 52.7% of the cases.")
Distribution of demographic characteristics: Sex, age, and body mass index (BMI) in the study population. The most common categories within each dataset were highlighted. Females are the predominant gender (92.3%), with the age group of 26 - 30 years being the most commonly affected. The average weight population, as indicated by a BMI range of 18.5 - 24.9, is predominantly affected, accounting for 52.7% of the cases.
Several modifiable risk factors were explored in this cohort study, including dietary habits, lifestyle choices, and reproductive factors. Additionally, we investigated the prevalence of underlying chronic illnesses in cases of gallstone disease. The results are depicted in Figure 2.
, surprisingly 69.2% adhere to a healthy high-fibre diet, sedentary lifestyle (73.6%) and pregnancy-related factors (76.5%) were prevalent among affected individuals, while a considerable number had a family history of gallstones at the same age (53.8%). Being on a diet (22%) Oral contraceptive pills OCPs (14.6%) and smoking (14.3%) were also observed in a portion of cases; B, underlying chronic illnesses, including haemolytic anaemia (13.2%), diabetes mellitus (5.5%), and liver disease (4.4%), further contribute to the multifaceted nature of gallstone disease.")
Distribution of modifiable risk factors and underlying chronic illnesses in gallstone disease cases. The data reveal a diverse range of modifiable risk factors and underlying chronic illnesses associated with gallstone disease. A, high-fat diet (75.8%), surprisingly 69.2% adhere to a healthy high-fibre diet, sedentary lifestyle (73.6%) and pregnancy-related factors (76.5%) were prevalent among affected individuals, while a considerable number had a family history of gallstones at the same age (53.8%). Being on a diet (22%) Oral contraceptive pills OCPs (14.6%) and smoking (14.3%) were also observed in a portion of cases; B, underlying chronic illnesses, including haemolytic anaemia (13.2%), diabetes mellitus (5.5%), and liver disease (4.4%), further contribute to the multifaceted nature of gallstone disease.
In this study, we investigated the distribution of treatment modalities and observed complications among the cases. As shown in Figure 3, the treatment landscape varied, with a predominant use of laparoscopic cholecystectomy (54.9%), providing a comprehensive view of gallstone management. Although there were instances of complications such as acute pancreatitis, obstructive jaundice, empyema, and intestinal obstruction, a substantial majority of cases (81.3%) did not encounter any complications during or after treatment.
, obstructive jaundice (4.4%), empyema (2.2%), and intestinal obstruction (2.2%), a substantial majority of cases (81.3%) did not encounter any complications during or after treatment.")
Distribution of treatment modalities and complications in the study population. Approximately 54.9% of the cases underwent laparoscopic cholecystectomy however, about 17.6% of cases opted for open cholecystectomy while a significant portion, 27.5%, chose conservative treatment. Although there were instances of complications such as acute pancreatitis (4.4%), obstructive jaundice (4.4%), empyema (2.2%), and intestinal obstruction (2.2%), a substantial majority of cases (81.3%) did not encounter any complications during or after treatment.
5. Discussion
The observed increase in laparoscopic cholecystectomy among teenagers and young adults at our facility prompted an investigation into the prevalence and potential risk factors associated with gallstone disease in individuals aged 15 - 40 years. The results reveal significant patterns, necessitating a discussion on the evolving landscape of gallstone disease in younger individuals and the factors influencing this trend.
Previous research, such as the Sirmione study (6), indicates that women aged 18 - 65 years are more susceptible to cholelithiasis compared to men within the same age group, with an overall prevalence of gallstone disease at 6.9% (8.9% among women and 4.5% among men). Furthermore, the incidence of gallbladder disease increases with age, with Schirmer et al. (7) reporting that approximately 20% of individuals over 40 and 30% of those over 70 develop biliary calculi. Women are about four times more likely than men to develop gallstones during their reproductive years, although this gender disparity diminishes with age.
Earlier studies have shown that the risk of developing gallstone disease increases with factors such as the number of pregnancies, obesity, and hypertriglyceridemia (4, 6, 7, 11).
In our study, the predominance of females among the affected demographic, with 56.1% of cases occurring in individuals under 30 and an overarching majority (83.6%) under 40 years of age, aligns with contemporary research trends. This is consistent with recent studies documenting an increased prevalence of gallstone formation and associated hospital admissions among individuals younger than 30 years, reflecting a shift in age incidence (1, 5, 8, 9). Additionally, Chilimuri et al. found that the prevalence of gallstones among young patients surged to 2.96% by 2010 over a 15-year period, with a notable 30% increase in hospitalizations due to gallstone disease, particularly among females (8).
In contrast to earlier literature, a retrospective cross-sectional study by Mehta et al. in 2012, involving 404 children under 18, found a statistically significant association between obesity and symptomatic gallbladder disease in juveniles (12). However, our study's finding of substantial prevalence (52.7%) among individuals with average weight (BMI 18.5 - 24.9) suggests a need to reconsider the association of gallstones with obesity alone.
In earlier research, Constantinescu et al. analyzed 1,905 cases of cholecystectomy to highlight the significant prevalence of gallstones and their underlying causes in young individuals. Their findings emphasized that age, female gender, pregnancy, and obesity were the most prevalent risk factors associated with gallstone formation (2). These observations were further supported by a study conducted in Korea (3). This study assessed modifiable risk factors and chronic conditions as potential contributors to gallstone formation, finding high-fat diet (75.8%) and sedentary lifestyle (73.6%) to be prevalent among affected individuals. Surprisingly, a notable proportion of individuals (69.2%) maintained a high-fiber diet, which is known for its preventive properties against gallstone formation. Pregnancy-related factors, which accounted for 76.5% of the cases, highlight the importance of considering reproductive history as a contributing factor (13).
Although the prevalence of gallstones varies by country, certain factors such as age, female gender, and genetic predisposition are considered unchangeable, while factors like obesity, rapid weight loss, oral contraceptive use, and physical inactivity are considered modifiable (14). Our study's findings align with existing knowledge about the risk factors associated with gallstones. Notably, only a small proportion of patients in this cohort reported engaging in rapid weight loss diets, using oral contraceptives, or being physically inactive. This suggests that while these factors can contribute to gallstone development, they may not be as prevalent among the study population compared to other risk factors.
Previous literature has proposed a correlation between chronic liver diseases, such as cirrhosis (15), diabetes, and hemolytic anemia (14), and the onset of various types of gallstones. In our study, the presence of modifiable risk factors and chronic conditions, including hemolytic anemia (13.2%), diabetes mellitus (5.5%), and liver disease (4.4%), underscores the complex nature of gallstone etiology within this population cohort.
The predominant use of laparoscopic cholecystectomy (54.9%) in this study reflects a shift in treatment preferences. A significant portion of patients (27.5%) opted for conservative treatment, indicating a nuanced approach to management. Although complications such as acute pancreatitis (4.4%), obstructive jaundice (4.4%), empyema (2.2%), and intestinal obstruction (2.2%) were present in some cases, they were notably absent in the majority (81.3%). This suggests an overall favorable outcome in the management of gallstone disease in this cohort. The findings emphasize the importance of timely management to reduce potential morbidity and improve outcomes for adolescents with gallstones. Previous studies suggest that delayed interventions can lead to increased rates of complications, such as common bile duct stones and severe pancreatitis, particularly in younger patients (10, 12, 13).
This study has several limitations. Firstly, it focused exclusively on individuals aged 20 - 40 years or younger. To improve the study's breadth, including both younger and older populations would be beneficial. Secondly, the study suffered from a limited sample size. More accurate results might have been obtained with a larger and more diverse sample, including additional variables such as liver function tests, lipid profiles, and ultrasound scans. In quantitative studies, sample size significance is generally higher than in qualitative investigations.
5.1. Conclusions
Our study examines the prevalence and risk factors associated with gallstone disease in individuals aged 20 - 40 years, revealing notable patterns and considerations. It confirms the well-established predominance of gallstone disease among females, particularly within this age bracket, consistent with prior research. Additionally, the study highlights a concerning trend of increasing gallstone formation and related hospitalizations among individuals under 30 years old, indicating a shift in age incidence patterns. While traditional risk factors like obesity and pregnancy remain significant, the study challenges the association of gallstones solely with obesity, noting a significant prevalence among individuals of average weight. It also emphasizes the complex interplay of modifiable risk factors and underlying chronic conditions in gallstone formation, underscoring the need for a comprehensive understanding of gallstone etiology in this demographic. Treatment preferences are shifting towards laparoscopic cholecystectomy, with generally favorable outcomes, although conservative management is also chosen by a considerable proportion of cases. Despite limitations such as a narrow age focus and sample size constraints, the study provides valuable insights into gallstone disease among young individuals, informing both research and clinical practice.
