1. Background
Chemical burns are the result of chemical-substance exposure. We can classify these substances into three groups: acid, alkaline and organic compounds (1). The chemical substance group currently includes approximately six million materials; 95000 of these consist of common substances, such as medicines, fertilizers, pesticides, cleaning products, disinfectants, solvents and cements (2). Sodium hypochlorite (NaClO, united nations number: 1791, chemical abstracts service number: 7681-52-9) is a conjugate base that is widely used in bleaching, stain removal, disinfection, deodorization and water treatment. In medical science, diluted NaClO solution has been accepted as a considerably less expensive and easy-to-prepare topical agent for burn therapy (3, 4).
The current literature indicates that chemical burns represent a relatively small proportion of burns, with a reported incidence of up to 10.7% (5), accounting for up to 30% of all burn-related deaths (6). In terms of NaClO, case reports have described endodontic treatment complications as a cause of chemical burns (7, 8). Another type of NaClO-induced chemical burn is epicutaneous exposure to bleach (9). Although there are no definitive data on the epidemiology of NaClO-related burns, epicutaneous exposures in particular, seem to be underestimated and are reported relatively rarely, compared to the real numbers (10). Moreover, management of NaClO burns is mainly based on expert opinions, and there is insufficient scientific information on this subject in the current literature.
The management of NaClO-induced chemical burns in can be evaluated in two consecutive phases: at the emergency department (ED) and during plastic surgery follow-up.
2. Objectives
We report our experience with NaClO-induced upper extremity chemical burns to illustrate the important points regarding its management.
3. Methods
In this retrospective descriptive study, we collected the data of NaClO-induced upper extremity chemical burn admissions to a military hospital over an eight-year period (2007 - 2015). The study was approved by the local ethics committee.
All patients were evaluated according to the hospital’s burn-patient policy; this process included initial treatment at the ED and the plastic surgery follow-up phase. The ED evaluation consisted of an initial examination in accordance with the general principles of trauma management, including airway management, adequate ventilation, and maintenance of hemodynamics. During these procedures, a detailed history of the chemical burn, including the type of agent, exposure sites, exposure duration, and concomitant injuries, were collected from the patients and their retinues. After removal of the clothing, large-volume lavage of the burn site was performed for at least 30 minutes. We obtained blood samples from the patients for complete blood count (CBC) analysis. Regardless of anatomic localization, the width and depth of the chemical burn injury in all cases were reported to a plastic surgeon. All patients were administered parenteral analgesics and tetanus immunizations, if needed.
The plastic surgery follow-up phase began with an initial examination of the irrigated chemical burn site under sterile surgical settings of the ED. Burn wound care was performed with Octanicept® antiseptic solution (Schulke and Mayr, Norderstedt, Germany) and Bactigras® total antiseptic dressing (Smith and Nephew, London, UK). After wound-dressing, the patients were admitted to the plastic surgery department for at least a 24-hour hospitalization. The plastic surgery policlinic follow-up included wound care every other day. We accepted a 21-day follow-up period as a sufficient healing time for further follow-up and treatment decisions (11). Surveyed data included patient age, gender, burn area, burn depth, treatments, and follow-up period. The numerical variables were given as means (min-max).
4. Results
Eight patients were admitted to the ED with complaints of NaClO-induced chemical burns of upper extremity skin, over an eight-year period. All of the patients were male, with a mean age of 21.25 (19 - 23) years. The patients’ demographics and burn injury details from the initial examination are presented in Table 1.
Table 1. Patients’ Demographic, Burn Injury, and Follow-Up Details
| Patient, No. | Age | Burn Area | Gender | Burn Depth | Treatment | Recovery After Three Weeks | Follow-Up Period, m |
|---|---|---|---|---|---|---|---|
| 1 | 19 | Hand | Male | 2° deep dermal | Medical dressing | Yes | 5 |
| 2 | 21 | Hand | Male | 2° deep dermal | Medical dressing | Yes | 5 |
| 3 | 22 | Hand | Male | 2° superficial dermal | Medical dressing | Yes | 3 |
| 4 | 22 | Hand | Male | 2° superficial dermal | Medical dressing | Yes | 3 |
| 5 | 23 | Hand | Male | 2° deep dermal | Debridement, skin graft | No | 9 |
| 6 | 21 | Hand | Male | 2° superficial dermal | Medical dressing | Yes | 3 |
| 7 | 21 | Forearm | Male | 2° superficial dermal | Medical dressing | Yes | 3 |
| 8 | 21 | Hand | Male | 2° deep dermal | Debridement, skin graft | No | 9 |
![This case [Case-6] was healed uneventfully with medical dressing.](https://brieflands.com/journals/jamm/articles/20848/figures/jamm-04-03-40369-g001-preview.webp "22-Year-Old Patient with Right Hand Chemical Burn")
Figure 1.
This case [Case-6] was healed uneventfully with medical dressing.
![This case [Case-2] was healed uneventfully with medical dressing. This patient’s second finger was amputated due to previous traumatic injury.](https://brieflands.com/journals/jamm/articles/20848/figures/jamm-04-03-40369-g002-preview.webp "21-Year-Old Patient With Right Hand Chemical Burn")
Figure 2.
This case [Case-2] was healed uneventfully with medical dressing. This patient’s second finger was amputated due to previous traumatic injury.
During the ED evaluation phase, all patients’ vital signs were in the normal range. There were no signs or symptoms related to the respiratory system, face, or eyes. Our patient group included young males without any chronic illness or medication history. All the incidents occurred as a result of household chemical exposure during occupational accidents. All patients or their retinues reported that household chemicals containing NaClO (a 10% - 25% solution) was the main content of the chemical material. In addition, they reported that the chemical materials were composed of variable amounts of other household chemicals, including bleach (a 3% - 8% solution of NaClO) and cream cleaners (5% - 15% anionic surfactants and < 5% non-ionic surfactants). It was determined that carelessness and negligence were the most common causes of chemical burns. On physical examination, erythematous plaques and surrounding edema were positive findings for all cases. The patients’ CBC results were within the normal range.
After the ED evaluation, all patients were evaluated by a plastic surgeon, and then hospitalized at the plastic surgery clinic for 24 hours. Hospitalization, discharge, and follow-up decisions for the patients were managed by the plastic surgeon. After a three-week follow-up period, six patients’ chemical burns were fully recovered (Table 1). Two patients needed five months of follow-up at weekly intervals, and four needed three months, due to complications (Table 1). During these follow-up periods, the plastic surgeon did not observe any complications or perform any further surgical interventions. After three weeks of follow-up, the plastic surgeon performed debridement and skin grafting on two patients, and followed them for a total of nine months.
5. Discussion
Emergency department management of chemical burns involves unique principles compared to other burn injuries. Identification of the involved chemical substance is the main factor. We observed that even in controlled occupational facilities, full identification of the substance might be impossible. The current literature presents reviews and case series of chemical burns; however, these studies mostly present cases from military (1) or industrial settings (2, 12-14). It was concluded that chemical burns occurring as a result of household chemical exposure have a higher probability of resulting from mixed chemical exposures. The belief that household chemicals provide more effective and fast cleaning, likely contributes to this situation.
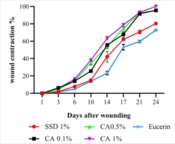
Increased use of NaClO in household products, as a disinfectant or a bleaching agent, makes it a common cause of skin burns. In the ED setting, the physician should evaluate the approximate amount of NaClO exposure and its effects on tissue. The tissue-dissolution capability and toxicity of NaClO depends on its concentration, pH, osmolarity, nature of contact, and duration of exposure (7, 15-17). Cotter et al. reported that 0.1% and 0.5% NaClO solutions, buffered at a physiological pH, are effective antimicrobial solutions and might be tolerated by patients for thermal injury (3). Coetzee et al. reported that an un-buffered solution of NaClO with a concentration of 0.006% would be suitable for topical management (4). Based on the literature, it can be concluded that NaClO compositions in antimicrobial solutions are present in small quantities, and there are no case reports in the literature presenting chemical burns as a result of NaClO-derived antimicrobial agent exposure. In dentistry, NaClO has been accepted and widely used as an effective intracanal irrigant (18) at concentrations ranging from 0.5% to 6.15% (19). Exposure to these concentrations of NaClO results in necrosis, ulceration, ecchymosis of soft tissue and neurological deficits (7, 8). According to current case reports, we can state that epicutaneous exposure to NaClO solutions with concentrations greater than 0.5% may have detrimental effects on soft tissues.
Emergency department management of NaClO-induced chemical burns starts with removal of clothes, then hydrotherapy with the application of large amounts of water or saline solution to the affected skin for a prolonged time (20). This intervention constitutes the fundamental and universal principal of chemical burn management. The toxic effects of epicutaneous NaClO exposure depend on its potential to cause deep tissue damage through liquefactive necrosis (10). Early and prolonged (30 minutes to 2 hours) lavage dilutes the agent and reduces the exposure time. Although sterile solutions are better in terms of preventing secondary infections, tap water can be used as a lavage material to wash the injury site with copious volumes of fluids. Neutralization in chemical burn injuries is controversial, and has been investigated in a small number of alkaline burn injuries (13, 21, 22). We observed that identification of the chemical substance and composition was difficult in NaClO-derived household chemicals, and we recommend against the use of neutralization of these chemicals in order to prevent further unforeseeable catastrophic effects.
In all cases included in this study, the burn injury sites had a total burn surface area (TBSA) of < 9%. Pavelites et al. reported that in most chemical burn cases, exposure is over a relatively small surface area and does not necessitate hospitalization (23). They accepted 15% total body surface area (TBSA) as the criterion for large exposure, and reported that larger exposures or exposures to chemicals with long-term effects may require hospitalization. However, our cases were classified as having small burn areas, and we suggest that upper extremity chemical burns are a special group of injuries with cosmetic aspects and effects on patients’ daily functions. In addition, some patients may need early eschar excision and should be hospitalized for at least the first 24 - 48 hours, according to the plastic surgeon’s decision.
The physical examination should be performed in a detailed manner; and should include vital signs, inspection of the entire body for detection of chemical exposure, and identification of wounds. In chemical burn injuries, early detection of respiratory injury can prevent progression to life-threatening complications, so examination of the respiratory system is more important than in other types of burns. Sodium hypochlorite has the potential to release chlorine gas, a potent irritant that leads to the added risk of inhalation injury (24, 25). Chlorine gas inhalation may result in cough, dyspnea, mucosal irritation, and life-threatening complications, including pulmonary edema and death (26). For this purpose, oxygen saturation and respiratory rate should be monitored, the upper respiratory system mucosa should be inspected, and breathing sounds should be auscultated. The detection of respiratory system-related signs and symptoms requires further evaluation and admission of the patient to the intensive care unit.
The laboratory tests that should be performed is another confusing aspect in the management of chemical burns. The current literature shows that chemical burns commonly have < 10% TBSA, and our survey results are compatible with this (12). We believe that these small proportions of burn surface area decrease the possibility of systemic contagion with chemical substances in cases of upper extremity chemical burn injuries. We conclude that only a CBC should be performed to assess the immunologic and hematologic status of minor upper extremity chemical burn patients. In cases of respiratory system involvement, further analyses, including arterial blood gases and routine biochemistry evaluations, should be performed.
Management of NaClO-induced upper extremity chemical burns should start with hydrotherapy. We recommend the use of tap water for high-volume, long-term lavage. We observed that epicutaneous exposure to NaClO solutions at concentrations of > 0.5% might have detrimental effects on soft tissues. We are against using neutralization chemicals in order to prevent more unforeseeable catastrophic effects, because it is difficult to determine the composition of the NaClO-derived household chemicals involved in the exposure. In addition, the ED management of these patients should include CBC, tetanus immunization, and parenteral analgesics. After ED evaluation, patients should be hospitalized for at least the first 24 - 48 hours, according to the plastic surgeon’s decision.