






1. Background
Benign esophageal strictures (congenital and acquired) are not rare diseases. The congenital include: esophageal atresia, achalasia, web, and Schatzki’s ring. The acquired types comprehend: stenosis secondary to reflux esophagitis, eosinophilic esophagitis, drugs or caustic ingestion and surgical complications (1). Dysphagia is one of the hallmark symptoms of esophageal strictures. It is characterized by nausea, vomiting, cough, hoarseness and failure to thrive (FTT) (2). These patients have dysphagia to solid foods, and this kind of stenosis can be resolved by esophageal dilatation. The primary goal of the procedure is to improve dysphagia. The best therapeutic response is seen in short-length stenosis (less than 2 cm) (3) and the EBD has a high clinical success rate (3). Previously, peptic stenosis secondary to gastroesophageal reflux (GER) accounted for approximately 80% of the causes of benign esophageal stenosis (ES). Nowadays the prevalence of this stenosis has decreased; due to the extensive use of proton pump inhibitors (PPIs) (4). The prevalence of stenosis due to ingestion of caustic agents was reported to be 2% - 38% (5). During the past two decades, EBD has been used to treat ES (5). In general, there are limited pediatric studies about the evaluation of EBD in treatment of ES (6). These studies have determined that this technique is more effective in the treatment of congenital ES. Pediatric EBD is performed by an over the wire (OTW) or achalasia special catheter. This method has high success rates and fewer side effects (7). Some studies in children show the effectiveness of this therapeutic approach (6). In many of the world’s prestigious medical centers, this method is used as the first line of treatment for pediatric ES (8). In each standard session, dilatation can be performed up to three times using proper catheters. Finally, the need for further dilations is determined based on the symptoms (7). If symptoms do not improve after five sessions, the esophageal diameter remains smaller than 14 mm, or the stenosis has recurred within a month after the procedure, this is considered as “treatment-resistant esophageal stricture” (9, 10). The EBD method has fewer complications than other procedures (11) The advantages of EBD compared to surgical procedures include: lack of long-term anesthesia, low cost, short-term hospital admission and fewer side effects. Also and if necessary, it can be repeated several times. Hamza et al. (12) observed that EBD has a high success rate (70% - 90%) in treating achalasia. In some studies, failure to balloon therapy has not been reported (13, 14) while in other studies, the incidence of failure of balloon therapy has been reported to be from 5.8 to 33% (15, 16). According to the review of the articles published in PubMed and Medline, there is no study on the success rate of EBD for benign esophageal strictures in children in Iran.
2. Objectives
Therefore, the purpose of this study was to identify the most common causes of benign esophageal stricture in children and determine the success rate of endoscopic balloon dilatation.
3. Methods
This is a prospective cross-sectional study performed during one year (2016 - 2017), at the Children’s Medical Center Hospital in Tehran (Iran). Children under 16 years with benign esophageal stricture were enrolled. They were previously studied with barium due to dysphagia and persistent vomiting, and it was determined the presence of ES, its location, and its length.
The sample size included all children less than 16 years with benign ES during one year. The number of samples in previous studies was around 30 cases.
3.1. The Exclusion Criteria
Children who did not have sustained vital signs, respiratory problems, so that their anesthesia was not possible and those with a febrile infectious disease. Also were excluded from the study the patients with signs of gastrointestinal (GI) perforation. Individuals with long segment stenosis (length of the stenosis more than 20 mm) also did not enter the study.
3.2. Intervention
At first, written consent was obtained from all patients or their parents. Children were examined by a pediatric gastroenterologist and their demographic characteristics including age, sex, cause of stenosis, length of stenosis and number of previous balloon dilatations were recorded. Afterward, endoscopy was performed by a pediatric gastroenterologist with video endoscope (Olympus CV-180 HD Evis Exera II, made in Japan). The procedure was conducted under general anesthesia. Different catheters (manufacture ENDO-FLEX Company of Germany) were used, including esophageal dilation balloon type OTW (size 8, 10, 12, and 14 mm) and achalasia balloon dilator (size 20, 25, and 30 mm). Each stage of dilation longed one minute, and the pressure required was 30 - 60 mmHg (17). The balloon diameter was based on the experience of the endoscopist, the age of patients and the cause and severity of the stenosis (17). After dilatation, patients were hospitalized for 24 hours and then discharged with prescription of proton pump inhibitors (PPIs). Chest X-rays were performed only in case of clinical suspicion of perforation. The duration of the follow-up was one year. A good response to treatment in children younger than 4 years was determined according to the following criteria: resolution of vomiting and difficulty in swallowing, easy passage of the endoscope and lack of visible mucosal lesions in the esophagus. This response was scored in children over 4 years of age according to clinical symptoms and categorized by the Vantrappen table (18). Table 1 depicts the score of these symptoms and their frequency per day. This scoring system was less useful in children younger than 4 years-old due to lack of proper collaboration. When the score after dilatation dropped more than 50%, it was considered as a good response to treatment. If this reduction was less than 50%, it was considered as a recurrence. In these cases, dilatation was performed again with a larger-size balloon. If the score did not drop higher than 50%, they would be considered recurrent or dilatation-resistant. The study was approved by the Ethics Committee of Tehran University of Medical Sciences. (approval number: IR.TUMS.MEDICINE.REC.1395.1936).
| Clinical Symptoms | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Dysphagia to solids | Never | Weekly | Daily | Every meal |
| Dysphagia to liquids | Never | Weekly | Daily | Every meal |
| Passive regurgitation | Never | Weekly | Daily | Every meal |
| Active regurgitation | Never | Monthly | Weekly | Daily |
| Chest pain | Never | Monthly | Weekly | Daily |
Vantrappen Table for Scoring of the Recovery
3.3. Statistical Analysis
The data were analyzed with Statistical Package for Social Sciences (SPSS) version 20 (IBM Corp.; Armonk, NY. USA). For the explanation of the descriptive and quantitative data were used a frequency and percentage, mean and standard deviation respectively. For more accurate statistical analysis was a used chi-square and Fisher test. The values of less than 0.05 were considered statistically significant.
4. Results
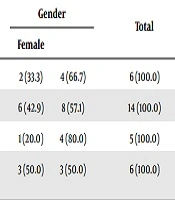
Between May 2016 and June 2017, thirty-one children with ES were referred for endoscopy. Sixty one percent (n = 19) of them were male. The mean age was 5.1 ± 3.9 years (range: 1 - 15 years). The most common causes of esophageal stricture were achalasia (45%), esophageal atresia (19%), caustic ingestion (19%) and congenital stenosis (16%) respectively. Table 2 depicts the most common cause of benign ES in children by gender. Congenital stenosis, esophageal atresia, and achalasia were more common in boys. (Table 2) The frequency of stenosis due to caustic ingestion was the same in both genders. Two types of catheters were used for dilatation: OTW catheter in 24 (44.4%) cases, achalasia catheter in 4 (12.9%), and in 3 (9.7%) cases both types of catheters were used. The OTW catheter was used in stenosis secondary to esophageal atresia, congenital stenosis, and caustic ingestion. In patients with achalasia, the OTW catheter was preferred in 7 (50%) cases; the achalasia catheter in 4 (28.6%) cases, and both catheters in 3 (21.4%) cases. In the younger patient with achalasia, OTW catheter was best, because it is thinner than the achalasia catheter. There were no complications following the EBD. A total of 64 dilatation procedures were performed. Some patients needed more than one procedure. The frequency of balloon dilatation was as follows for each patient: 1, 2, 3, 4, and 5 times dilatation were performed in 15 (48.4%), 8 (25.8%), 1 (3.2%), 5 (16.1%) and 2 (6.5%) patients, respectively. According to this data, only one session was effective in 48.4% of children. Overall, in 23 (74.2%) patients, clinical problems were resolved with 1 - 2 times dilatation. Table 3 summarizes the frequency of the type of strictures with the number of dilatations. The response and failure to treatment is shown in Table 4. In cases when the score after dilatation dropped less than 50%, endoscopy and dilatation were again performed. The balloon dilatation failure and referral to surgery was considered when the endoscope could not pass through the stenosis or in case of risk of perforation. A total of 87.1% children (n = 27) had a good response to treatment. Resistance to treatment or recurrence of the stricture was more common in patients with stenosis due to caustic ingestion. (33.3%) There were no cases of treatment failure in this group. A total of 4 patients (12.9%) had a treatment failure and were referred for surgery.
| Type of Stenosis | Gender | Total | |
|---|---|---|---|
| Female | Male | ||
| Esophageal atresia | 2 (33.3) | 4 (66.7) | 6 (100.0) |
| Achalasia | 6 (42.9) | 8 (57.1) | 14 (100.0) |
| Congenital stenosis | 1 (20.0) | 4 (80.0) | 5 (100.0) |
| Stenosis after caustic ingestion | 3 (50.0) | 3 (50.0) | 6 (100.0) |
The Most Common Cause of Benign Esophageal Stenosis in Children by Gendera
| Number of Dilatations | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Esophageal atresia | 3 (50.0) | 3 (50.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Achalasia | 7 (50.0) | 3 (21.4) | 0 (0.0) | 3 (21.4) | 1 (7.1) |
| Congenital stenosis | 4 (80.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (20.0) |
| Stenosis after caustic ingestion | 1 (16.7) | 2 (33.3) | 1 (16.7) | 2 (33.3) | 0 (0.0) |
| Total | 15 (48.4) | 8 (25.8) | 1 (3.2) | 5 (16.1) | 2 (6.5) |
The Frequency of Stenosis Type, with the Number of Dilatations in Patients with Benign Esophageal Stenosisa
| Type of Stenosis | Response to Treatment | Failure to Treatment |
|---|---|---|
| Esophageal atresia | 5 (83.3) | 1 (16.7) |
| Achalasia | 12 (85.7) | 2 (14.3) |
| Congenital stenosis | 4 (80.0) | 1 (20.0) |
| Stenosis after caustic ingestion | 6 (100.0) | 0 (00.0) |
| Total | 27 (87.1) | 4 (12.9) |
Response and Failure to Treatment After Endoscopic Balloon Dilatation in Children with Benign Esophageal Stenosisa
5. Discussion
The main causes of esophageal stricture in the adult are the gastroesophageal reflux disease (GERD) and malignancy (1). In children, these include: caustic ingestion, esophagitis (secondary to the GERD or eosinophilic), infections, achalasia, and postoperative stricture (19). In our study, among the 31 patients with ES, achalasia was the most common cause (45%). We did not observe stenosis due to reflux (GERD), which seems due to the increasing use of acid inhibitors in children. Lan et al. (6) in England and Hong Kong studied 77 patients with esophageal stricture. The mean age of patients was 1.8 years, while in our study it was 5.1 years. Unlike our study, the most common cause of esophageal stricture was esophageal atresia (n = 63), and cases with achalasia were rare (n = 2). The reason for this difference is the mean age of the patients. In our study, the mean age was higher and therefore, the risk of achalasia was higher as well. Pieczarkowski et al. (20) in Poland and Bittencourt et al. (21) in Brazil reported the most common causes of esophageal stricture to be postoperative stenosis, and stenosis due to caustic ingestion. Pieczarkowski et al. (20) showed that one session of balloon dilatation was successful in only 10% of children, and the vast majority of patients (90%) needed more than two sessions, which this is also reported by others (22-24). This is in contradiction to our study, where one procedure of dilatation was successful in 48% (n = 15). In the study by Yeming et al. (15), treatment failure was reported in 42.8% of children with stenosis due to caustic ingestion. However we did not found any failure from patients with this type of stenosis. On the other hand, 73% (n = 5) of these children in our study needed repeated balloon dilatations. The success rate of balloon dilation was reported to be as high as 96%, by Khodadad et al. (25) Of the 39 patients with achalasia in the Khodadad et al.’s study (25), only one patient (4%) suffered from recurrent stenosis after two sessions of dilatation and was referred for surgery due to his/her parents’ dissatisfaction with doing re-dilatation. In our study, half of the patients with achalasia required multiple dilations, and eventually, two of them (14.3%) required surgery. Therefore our success rate of balloon dilation was 85.7% (n = 12). This difference could be due to the low number of achalasia, rather than the study of Khodadad et al. (25) (14 vs. 39 cases). Babu et al. (16) reported a success rate of 80% in the treatment of achalasia with balloon dilation. In our study, this rate was 85.7%. Total success rate of balloon therapy in Lan’s study was 97% (6), and in our study was 87.1%. This difference can be explained as the number of achalasia cases in the Lan’s study was lower (2 vs. 14 cases), and the mean age of patients was lower as well (1.8 vs 5.1 years). In 2002, Mikaeli et al. (26) evaluated the results of balloon dilatation therapy in 99 achalasia patients. In this study, one-time dilatation was associated with 65% improvement and more than one-time dilatation with 94%. The mean recovery time was 44.7 months and the mean age of patients 35.6 years. In our study, 48.4% of patients fully recovered after one dilatation, and 87.1% after several sessions. The most common complication of balloon dilatation is esophageal bleeding, and the most serious complication is esophageal perforation. In various studies, the incidence of perforation has been reported differently from 3-5% and rarely up to 21% (27, 28). In the study of Pieczarkowski et al. (20), only one case of esophageal perforation (0.28%) was reported. In our study, there were no perforations following the procedure.
5.1. Conclusions
Achalasia, esophageal atresia, and caustic ingestion are the most common cause of benign esophageal stricture in the children. Therefore EBD is an effective and safe therapeutic approach in children with benign stenosis. This technique is recommended, even in cases where there is a history of previous surgery, such as restoration of esophageal atresia, or recurrence of stenosis after initial dilatation. This therapeutic procedure can be successful without any side effects if done by a skilled and experienced operator with the appropriate size of catheters.
The most important of our limitations was the short duration of the follow-up period and the small size of the samples.
