




1. Background
A chronic underlying disease is one of the most important risk factors for mental disorders, such as anxiety and depression (1). Chronic diseases affect the patient’s daily activities and impose too much stress on the patient and his/her family (2). In general, individuals with chronic diseases are 41% more likely than others to have psychiatric disorders (1). Research studies, meta-analyses, and systematic reviews demonstrate that adults and children with chronic diseases and their families are more at risk for depression and anxiety than others (3).
Cystic fibrosis (CF) is an autosomal recessive disorder resulting from a deviation in a gene encoding the cystic fibrosis transmembrane conductance regulator protein. CF causes abnormal ion transport throughout the body. This disease causes problems with mucus secretion in the lungs, leading to chronic lung infection and inflammation (4). The CF is a chronic incurable genetic disorder threatening individuals’ lives. It is estimated that one in two to three thousand white neonates has CF (5).
Recent advances in CF management and treatment have led to an increase in life expectancy among CF patients. In most countries, the mean age of survival for CF patients is 30 to 40 years, representing a 10-year increase, compared to that reported for the previous decade (6, 7). Furthermore, this has caused CF patients and their families to face many problems by increasing the patient’s age, such as increasing the symptom burden and number of complications, indicating that these individuals need more time-consuming and complex treatment processes (6). Therefore, it is important to pay attention to the mental problems of CF patients because studies showed that depressed patients are more likely to miss physician’s visits, have less life expectancy, and do not pursue their treatment. Therefore, the early diagnosis and treatment of depression and other mental health problems can improve the long-term consequences of CF (6).
Studies proved that the prevalence of depression in CF patients is 8 - 29% for children and adolescents and 13 - 33% for adults (8, 9). The prevalence of anxiety in adults is within the range of 30 - 33% (10). Mortality and complications of the disease pose many cognitive, emotional, and behavioral challenges not only for CF children but also for their families (4). The prevalence of depression among these caregivers is within the range of 20 - 35% (11). Moreover, the International Depression Epidemiological Study (TIDES) holds forth that adolescents with CF whose parents suffer from depression or anxiety are twice as likely to be depressed and anxious (12). Depression, anxiety, and insanity in CF patients not only affect their family members but also, in the short and long term, can affect the severity of the disease and its complications (6).
Previous studies in this regard can be divided into two groups. The first group includes the studies separately examining the patients or patients’ parents. The second group includes the studies considering both patients and parents, investigating the relationship between the mental health of both groups.
The association between anxiety and depression with the quality of life in CF patients has been considered in a study by Yohannes et al. (5). The aforementioned study was performed on 121 CF patients over 18 years of age. A study conducted by Havermans et al. (11) also examined the relationship between anxiety, depression, and clinical symptoms with the quality of life in CF patients. The aforementioned study was conducted on 57 adult CF patients with a mean age of 26.7 years. Another survey (13) in Spain studied the relationship between the quality of life with depression and anxiety. The study population was considered 336 CF patients. Yılmaz et al. (14) investigated sleep disorders, anxiety, and depression among mothers whose children had CF or asthma. The aforementioned study was conducted on a sample, including mothers of 62 children with asthma, 21 children with CF, and 35 healthy children.
As previously reported, the second group of studies considered both patients and parents. The largest and most comprehensive study in this regard (i.e., the TIDES) observed nine countries in terms of depression prevalence among CF patients and their parents. The countries included in the study were Belgium, Germany, Italy, Spain, Sweden, the Netherlands, Turkey, the United Kingdom, and the United States. In the aforementioned study, 6088 CF patients over 12 years of age and 4102 parents of children with CF under 18 years of age were studied from 154 CF centers in Europe and the United States (12). Additionally, Catastini et al. (2) studied the prevalence of depression and anxiety in CF patients and their parents and examined their association with the clinical signs of the disease. The aforementioned study was performed on 614 CF patients and 443 parents in Italy.
To date, in Iran, no studies have specifically studied the psychological problems of CF patients. However, several studies are related to respiratory and non-respiratory diseases, all of which belong to the first group of studies. The end-stage of kidney disease and dialysis severely affect the physical and mental health of patients. Due to the long duration of treatment and lifestyle changes in these patients, a study (15) was conducted to determine the prevalence of depression in patients undergoing hemodialysis in Birjand, Iran. The results of studies indicated a high prevalence of psychological complications in patients with multiple sclerosis (MS). Therefore, a study was designed to investigate the prevalence of personality disorders in MS patients in South Khorasan province, Iran. The aforementioned study was performed on 55 MS patients (16).
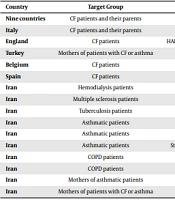
In a study conducted on respiratory patients, Vagharfard (17) focused on tuberculosis because it was particularly prevalent among individuals with mood disorders, such as depression. For this reason, physicians should also be aware of the clinical manifestations of depression when treating tuberculosis patients, as this may lead to treatment discontinuation or disordered treatment. The study by Vagharfard was performed on 76 tuberculosis patients. In various studies, Safa et al. and Fallah Tafti et al. investigated the prevalence of depression and anxiety, quality of life, and sleep quality among asthmatic children (18-20), chronic obstructive pulmonary disease children (21, 22), mothers of asthmatic children (23), and mothers of children with asthma or CF (24). However, as previously mentioned, none of the studies in Iran has considered both groups of patients and parents simultaneously and studies the relationship between the psychological problems of both groups. Table 1 shows the used questionnaires, year of article publication, and country of study.
| Country | Target Group | Questionnaire | Year of Publication | Author (s) |
|---|---|---|---|---|
| Nine countries | CF patients and their parents | HADS, CES-D | 2014 | Quittner et al. (12) |
| Italy | CF patients and their parents | HADS, CES-D | 2016 | Catastini et al. (2) |
| England | CF patients | HADS, Cystic Fibrosis Quality of Life Questionnaire | 2012 | Yohannes et al. (5) |
| Turkey | Mothers of patients with CF or asthma | HADS, PSQI | 2008 | Yılmaz et al. (14) |
| Belgium | CF patients | HADS, CFQ-14+ | 2008 | Havermans et al. (11) |
| Spain | CF patients | HADS, CFQ-14+ | 2016 | Olveira et al. (13) |
| Iran | Hemodialysis patients | Beck Depression Inventory | 2010 | Mogharab et al. (15) |
| Iran | Multiple sclerosis patients | Beck Depression Inventory | 2015 | Javidan (16) |
| Iran | Tuberculosis patients | Beck Depression Inventory | 2014 | Vagharfard (17) |
| Iran | Asthmatic patients | GHQ-28 | 2014 | Safa et al. (18) |
| Iran | Asthmatic patients | HADS | 2013 | Fallah Tafti et al. (19) |
| Iran | Asthmatic patients | St. George’s Respiratory Questionnaire, GHQ-28 | 2011 | Fallah Tafti et al. (20) |
| Iran | COPD patients | PSQI, Patient Health Questionnaire | 2017 | Eslaminejad et al. (21) |
| Iran | COPD patients | Hamilton Anxiety Scale | 2015 | Safa et al. (22) |
| Iran | Mothers of asthmatic patients | Symptom Checklist-90-Revised | 2014 | Safa and Ghasem Boroujerdi (23) |
| Iran | Mothers of patients with CF or asthma | PSQI, HADS | 2012 | Safa et al. (24) |
Abbreviations: CF, cystic fibrosis; HADS, Hospital Anxiety and Depression Scale; CES-D, Center for Epidemiologic Studies-Depression Scale; PSQI, Pittsburgh Sleep Quality Index; CFQ-14+, Cystic Fibrosis Questionnaire for adolescents and adults; GHQ-28, General Health Questionnaire; COPD, chronic obstructive pulmonary disease.
Due to the high prevalence of anxiety and depression in CF patients, it is recommended that these patients should be evaluated for depression and anxiety once a year and referred to a psychologist if necessary (1). There are two main methods for the assessments of depressive symptoms, namely diagnostic interviews and standardized screening measures. The diagnostic interview is a golden standard to diagnose depression; however, it takes time and requires an expert, such as a psychologist or psychiatrist, specifically trained in this field. On the contrary, screening criteria are concise and inexpensive and do not require special training. These criteria have been attentively evaluated by psychometrics and are entirely relevant to diagnostic interviews and appropriate for clinical centers or research protocols (25).
Considering the importance of the issue, the present study investigated the prevalence of depression and anxiety disorders in CF patients and their parents in Iran. In this study, the second method of measuring depression and anxiety symptoms, namely using the screening criteria, was used. Moreover, since the Pediatric Respiratory Diseases Research Center of National Research Institute of Tuberculosis and Lung Diseases (NRITLD) is a referral center for CF patients in Iran, it was selected as the research site.
2. Objectives
This survey answers the following questions: (1) what is the prevalence of depression among CF patients and their parents; (2) what is the prevalence of anxiety among CF patients and their parents; (3) is there any association between depression and anxiety in CF patients and their parents?
3. Methods
This descriptive-analytical cross-sectional study was conducted at the Pediatric Respiratory Diseases Research Center of NRITLD as a referral center for CF patients in Iran in 2020. In this study, 110 questionnaires were distributed among all CF patients who were hospitalized within January to May 2020 and their parents. All the questionnaires were collected anonymously. Furthermore, consent forms were signed by the subjects before participating in the study. The questionnaire consisted of two sections. The first section included demographic data, namely age, gender, educational level, and duration of disease diagnosis. In the second section, the Hospital Anxiety and Depression Scale (HADS) (26) was used as a tool to measure depression and anxiety. The validity and reliability of the Persian version of the questionnaire have been investigated in previous studies (27).
The HADS questionnaire is a 14-item screening scale based on the patient’s self-report, including a 7-item scale for measuring depression (HADS-D) and a 7-item scale for measuring anxiety (HADS-A). For each item, there are four possible answers with a score of 0 to 3. Moreover, the maximum possible score for each of the subscales of depression and anxiety is 21. A higher score on each subscale indicates more severe symptoms of depression or anxiety. A score of 7 was considered a depression and anxiety threshold in each subscale. For both subscales of depression and anxiety, the scores within the ranges of 0 - 7, 8 - 10, and 11 - 15 were considered normal, mild, and moderate, respectively. Furthermore, scores higher than 16 were regarded as severe (12).
Descriptive and inferential statistics were used to analyze the research data. Descriptive statistics were used to describe demographic data and calculate frequencies and scattering indices, such as mean and standard deviation. The Kolmogorov-Smirnov test, independent t-test, Pearson and Spearman correlation coefficients, and Mann-Whitney U test were used for inferential statistics. In addition, SPSS software (version 22) was used to examine and analyze the raw data.
4. Results
Out of the 110 distributed questionnaires, 101 cases were filled out and returned (response rate: 91.8%). After excluding the confounding questionnaires, 96 filled out questionnaires (36 for parents and 60 for patients) were analyzed in this study. Tables 2 and 3 show the demographic data and duration of diagnosis for both groups of patients and parents, respectively.
| Values | No. | % | Mean | SD |
|---|---|---|---|---|
| Age (y) | 18.18 | 6.43 | ||
| < 7 | 1 | 1.7 | ||
| 7 - 18 | 32 | 53.3 | ||
| > 18 | 27 | 45 | ||
| Gender | - | - | ||
| Female | 22 | 36.7 | ||
| Male | 38 | 63.3 | ||
| Educational level | - | - | ||
| Preschool | 1 | 1.7 | ||
| Elementary school | 15 | 25 | ||
| Junior high school | 12 | 20 | ||
| High school | 20 | 33.3 | ||
| Bachelor of science | 11 | 18.3 | ||
| Missing | 1 | 1.7 | ||
| Duration of cystic fibrosis diagnosis (y) | 11.52 | 6.21 | ||
| <10 | 25 | 41.7 | ||
| 10-19 | 26 | 43.3 | ||
| >20 | 8 | 13.3 | ||
| Missing | 1 | 1.7 |
| Values | No | % | Mean | SD |
|---|---|---|---|---|
| Age (y) | 44.21 | 6.10 | ||
| < 20 | 0 | 0 | ||
| 20 - 39 | 8 | 22.2 | ||
| 40 - 59 | 20 | 55.6 | ||
| ≥ 60 | 0 | 0 | ||
| Missing | 8 | 22.2 | ||
| Gender | - | - | ||
| Female | 30 | 83.3 | ||
| Male | 6 | 16.7 | ||
| Educational level | - | - | ||
| Preschool | 2 | 5.6 | ||
| Elementary school | 14 | 38.9 | ||
| Junior high school | 11 | 30.5 | ||
| High school | 8 | 22.2 | ||
| Bachelor of science | 0 | 0 | ||
| Master of science | 0 | 0 | ||
| PhD | 0 | 0 | ||
| Missing | 1 | 2.8 | ||
| Duration of cystic fibrosis diagnosis (y) | 10.56 | 5.53 | ||
| <10 | 17 | 47.2 | ||
| 10-19 | 18 | 50 | ||
| ≥20 | 1 | 2.8 |
Table 2 tabulates that most patients are male, and the highest frequency is observed in the age group of 7 - 18 years and educational level of high school. In addition, the duration of diagnosis for most patients was 10 - 19 years. However, Table 3 shows that mothers participate in the study more than fathers. The age group of 40 - 59 years and educational level of elementary school had the highest frequency among the parents. Moreover, in half of the cases, the duration of diagnosis was 10 - 19 years. In the data preprocessing stage, the missing items were completed with the mean value (for the quantitative data) or mode value (for the qualitative data). The details of the scores for the participants’ depression and anxiety scales are shown in Table 4.
| 0 - 7 Normal | 8 - 10 Mild | 11 - 15 Moderate | 16+ Severe | Mean ± SD | Total | |
|---|---|---|---|---|---|---|
| HADS Anxiety | ||||||
| Patients | ||||||
| Male | 3 (7.9) | 6 (15.8) | 26 (68.4) | 3 (7.9) | 12.34 ± 2.79 | 38 (100) |
| Female | 1 (4.5) | 5 (22.8) | 15 (68.2) | 1 (4.5) | 11.86 ± 2.42 | 22 (100) |
| Total | 4 (6.7) | 11 (18.3) | 41 (68.3) | 4 (6.7) | 12.17 ± 2.65 | 60 (100) |
| Parents | ||||||
| Mothers | 3 (10) | 8 (26.7) | 19 (63.3) | 0 (0) | 11.5 ± 2.65 | 30 (100) |
| Fathers | 0 (0) | 2 (33.3) | 2 (33.3) | 2 (33.3) | 13.33 ± 3.39 | 6 (100) |
| Total | 3 (8.3) | 10 (27.8) | 21 (58.3) | 2 (5.6) | 11.81 ± 2.82 | 36 (100) |
| HADS Depression | ||||||
| Patients | ||||||
| Male | 2 (5.2) | 15 (39.5) | 21 (55.3) | 0 (0) | 10.55 ± 2.08 | 38 (100) |
| Female | 1 (4.5) | 8 (36.3) | 13 (59.1) | 0 (0) | 10.64 ± 2.19 | 22 (100) |
| Total | 3 (5) | 23 (38.3) | 34 (56.7) | 0 (0) | 10.58 ± 2.1 | 60 (100) |
| Parents | ||||||
| Mothers | 3 (10) | 11 (36.7) | 16 (53.3) | 0 (0) | 10.4 ± 2.01 | 30 (100) |
| Fathers | 0 | 2 (33.3) | 4 (66.7) | 0 (0) | 11.5 ± 1.22 | 6 (100) |
| Total | 3 (8.3) | 13 (36.1) | 20 (55.6) | 0 (0) | 10.58 ± 1.93 | 36 (100) |
Abbreviation: HADS, Hospital Anxiety and Depression Scale.
a Values are indicated as No. (%) or mean ± SD.
Table 4 shows that the prevalence of anxiety in patients with a mean of 12.17% is higher than that reported for parents with a mean of 11.81%. Furthermore, 75% of the patients and 63.9% of the parents were in moderate to severe anxiety levels, and the prevalence of depression in patients and parents (10.58%) was almost equal. Severe depression was reported for either parents or patients; nevertheless, 56.7% of the patients and 55.6% of the parents had moderate depression. The results demonstrated that the prevalence of depression and anxiety was higher among fathers than mothers. In addition, the prevalence of anxiety was higher among male patients than female patients; however, the prevalence of depression was higher among female patients than male patients. The use of the Mann-Whitney U test showed that none of these differences was statistically significant (P > 0.05). The Kolmogorov-Smirnov test showed that the significance level for all the variables was higher than 0.05; therefore, the distribution of all the sample variables in both groups of patients and parents was normal. Then, the association between variables was investigated using Pearson and Spearman correlation coefficients. Table 5 tabulates the correlation coefficients and significance levels.
| Variables | Patients | Parents | ||
|---|---|---|---|---|
| Correlation Coefficient | Sig. | Correlation Coefficient | Sig. | |
| Depression | ||||
| Age | -0.053 | 0.687 | -0.253 | 0.037 |
| Educational level | -0.073 | 0.582 | 0.067 | 0.465 |
| Duration of cystic fibrosis diagnosis | 0.224 | 0.047 | -0.007 | 0.967 |
| Anxiety | 0.083 | 0.530 | 0.126 | 0.463 |
| Anxiety | ||||
| Age | -0.392 | 0.000 | 0.008 | 0.964 |
| Educational level | -0.132 | 0.316 | -0.239 | 0.065 |
| Duration of cystic fibrosis diagnosis | 0.281 | 0.001 | -0.282 | 0.003 |
| Depression | 0.083 | 0.530 | 0.126 | 0.463 |
Table 5 shows that in the patients’ group, there is a direct and significant relationship between the duration of diagnosis with depression and anxiety. Moreover, there was an inverse and significant relationship between the patient’s age and anxiety. In the parents’ group, there was a significant inverse association between age and depression, as well as between the duration of diagnosis and anxiety. According to the findings, there was no significant relationship between anxiety and depression in either parents’ or patients’ groups. In addition, the independent t-test revealed that there was no significant difference (P = 0.301 and P = 0.211) between the mean of depression and anxiety in both groups of parents and patients.
5. Discussion
This survey has been the first study to investigate the prevalence of anxiety and depression among CF patients and their parents in Iran. According to the findings, 75% of the patients and 63.9% of the parents had moderate to severe anxiety. Although severe depression was not reported in either parents or patients, 56.7% of the patients and 55.6% of the parents had moderate depression. In the TIDES study (12), depressive symptoms (the HADS score of above 7) were observed in 10% of adolescents, 19% of adults, 37% of mothers, and 31% of fathers. Furthermore, there were anxiety symptoms (the HADS score of above 7) in 22% of adolescents, 32% of adults, 48% of mothers, and 36% of fathers.
Catastini et al. (2) proved that 14% of patients and 19.9% of parent caregivers were anxious, and the prevalence rates of depression in patients, mothers, and fathers were 5.7, 8.7, and 2.8%, respectively. In the aforementioned study, HADS scores of above 10 were considered the measure of depression or anxiety, and patients were over 11 years of age. The prevalence of 33% for anxiety symptoms and 17% for depressive symptoms in another study (5) was reported in patients with a mean age of 30 years. The HADS score of above 8 was considered for having symptoms. In a study performed by Havermans et al. (11), the HADS score was above 7 in 30 and 13% of patients for anxiety and depression, respectively. The mean age of patients in the aforementioned study was 26.79 years.
In a study (13) conducted on patients over 18 years of age, 12.2 and 29.7% of subjects had depressive and anxiety symptoms, respectively, in which the HADS score of above 8 was considered the threshold. The prevalence of depression and anxiety symptoms in another study performed on patients over 18 years of age was reported to be 45% (28). Furthermore, in a study by Cronly et al. performed on patients over 17 years of age, 26.4 and 9% of patients had the HADS score of above 7 for anxiety and depression, respectively (29). In another study conducted by Cronly et al. on the parents of children under 17 years of age, it was shown that 38 and 12% of subjects had the HADS score of above 7 for anxiety and depression, respectively (30).
The present study suggested that gender did not make any significant difference between the prevalence of depression and anxiety. Some studies confirmed the findings of the current study (2, 13), and some studies contradicted the findings of the current study and reported a higher prevalence of depression and anxiety among women than men in both patients and parents (2, 28, 30). The current study also suggested that age was inversely related to anxiety in patients and depression in parents. Some previous studies reported a direct association between the age of patients or parents and prevalence of depression and anxiety (5). Moreover, some studies observed no association in this regard (13, 30). Nonetheless, some studies have confirmed an inverse relationship between patient’s age and their anxiety (2). In this study, the educational level had no effect on depression and anxiety in either group of parents or patients; however, other studies reported an inverse association between educational level with depression and anxiety prevalence (13, 28).
In the present study, the duration of diagnosis was considered an indicator of the patient’s current state of life. The findings suggested a direct and significant relationship between the duration of diagnosis with depression and anxiety in the patients’ group; nonetheless, in the parents’ group, there was a significant inverse relationship between the duration of diagnosis and anxiety. However, some studies did not find any significant relationship between parents’ depression and anxiety with their children’s duration of diagnosis (30). Numerous studies inferred an increase in anxiety and depression among patients and parent caregivers in case of the exacerbation of the patient’s respiratory condition (5, 30); nevertheless, some other studies concluded the opposite (13, 28). The results of the present study indicated that there was no significant relationship between the prevalence of depression and anxiety in either parents’ or patients’ groups; however, a direct relationship was concluded in this regard in some studies (11, 13).
5.1. Conclusion
In the present study, due to the small sample size, it was not possible to separate the age groups; nevertheless, by comparing the findings of this study to the findings of previous studies, it was observed that regardless of demographic characteristics, anxiety and depression in CF patients and parent caregivers had a high prevalence in Iran. Therefore, it is necessary to pay close attention to the mental health status of these individuals. Therefore, it is of paramount importance to plan for regular monitoring of these individuals’ mental health and provide mental health services to reduce the levels of depression and anxiety.
