


1. Background
Obesity is increasingly known as a serious public health concern (1). Evidence suggests that its worldwide prevalence has increased dramatically in recent decades (2-6).
According to the World Health Organization (WHO), overweight and obesity in children and adolescents are defined as a body mass index (BMI) of 2 and 3 standard deviations above the WHO’s growth standard median, respectively (7).
Overweight and obesity are frequently observed among adolescents and children worldwide, a problem that is faced by all countries. However, they are more pronounced in low- and middle-income countries. At the current rate, it is predicted that the prevalence of overweight and obesity will be higher than that of the underweight by 2022 (8).
According to a systematic review by Bibiloni Mdel et al., the prevalence of overweight and obesity varies greatly across the world. Estimates show that about 30% of American adolescents and 22% - 25% of Europeans are either overweight or obese. So, this report shows that obesity is not merely a problem in third-world countries but also poses a health threat to developed countries and the whole world (9).
Based on a study by Kelishadi et al., the prevalence of obesity and overweight among Iranian children were 3.22% and 9.27%, respectively. Also, obesity prevalence in elementary school students and overweight prevalence in intermediate school students were higher than in high school students (10).
Childhood and adolescence obesity can contribute to the development of many diseases in adulthood. Evidence confirmed that premature obesity was associated with an increased risk of life-threatening diseases in the future, such as type 2 diabetes, hypertension, and coronary heart disease (11). Furthermore, obesity and overweight can increase the risk of disease-related death (12). Furthermore, childhood obesity also results in anxiety & depression, low self-esteem, and lower self-reported quality of life, as well as being bullied and stigmatized and developing diseases such as asthma, sleep apnea, cancer, fatty liver disease, and gastroesophageal reflux disease (13).
An important issue in obese boys is concealed penis, which can exaggerate anxiety and decrease self–steam and sexual function in the future (14, 15).
Overweight and obesity are caused by various factors, including genetic and environmental-lifestyle contributors that play important roles in the development of overweight and obesity. Hence, the promotion of a healthy lifestyle and adaptation of appropriate lifestyle modifications from early childhood can reduce the prevalence of overweight and obesity (16, 17). Assessment of the burden of overweight and obesity among children is an essential first step toward addressing this problem. Also, socioeconomic status affects the development of obesity in different age groups (18).
2. Objectives
Despite the high priority of the problem, there are few studies on the prevalence of obesity among Iranian children. Given the importance of being informed about obesity prevalence and related factors in implementing preventive programs, the present study’s main objective was to determine the prevalence of overweight and obesity among 8 - 12-year-old children in primary schools in Tehran, Iran. There are two types of educational systems in schools in Iran, private and public, generally covering children with different socioeconomic levels, which was addressed in this study as a primary goal. Also, the samples were selected by cluster sampling to augment data validity. 3. Methods
This cross-sectional study was conducted on 829 primary school students aged 8 - 12 years recruited from several schools in Tehran, Iran, after checking for inclusion criteria. Children with the confirmed diagnosis of chronic diseases, including malignancy, diabetes, kidney disease, and heart disease, were excluded.
For selecting the subjects, we used multi-stage cluster sampling. We divided Tehran into five areas of the Northern, Eastern, Western, Southern, and Central divisions. After that, we obtained permission from the Education Department of each zone and observed the names and addresses of for-profit and not-for-profit schools.
Using simple random sampling, two elementary schools were chosen from each zone. Thus, the data were gathered from a total of 10 elementary schools.
In Iran, the duration of the primary school period is six years, so six classes were selected from each school.
The sample size was calculated by G*Power software and using the sample size formula below:
The expected power (1 - β) for this study was 0.8.
For deciding about the body weight status of students, we used the MedCalc 3000 system. Height (cm) was measured by a standing meter with an accuracy of 0.5 cm, while children wore no shoes. The Beurer scale (Germany) was used to measure weight (kg) while children wore light clothing and no shoes. Body mass index (BMI) was calculated as follows:
According to the WHO’s child growth standards, the BMI was categorized into four groups, including underweight (< 5 percentile), normal weight (≥ 5 percentile to < 85 percentile), overweight (≥ 85 percentile to < 95), and obese (≥ 95 percentile).
Our protocol was approved by the Medical Research Ethics Committee of the Iran University of Medical Science under the code: IR.IUMS.REC.1394.04.140.26839. In addition, the Ministry of Education in Tehran granted us permission to conduct this study in selected schools. Consent forms were signed by children’s parents, and verbal explanations were given to children. A total of 920 children with their parents were invited to participate in this study; 53 students were excluded from the study because of having chronic diseases (two with anemia, one with migraine, one with chronic kidney disease (CKD), one with kidney stones, five with heart disease, two with glucose-6-phosphate dehydrogenase deficiency, two with recurrent urinary tract infections (UTI), one with nocturia, two with chronic sinusitis, two with gastroesophageal reflux disease, three with diabetes, two with hypothyroidism, two with epilepsy, one with thalassemia, 11 with asthma, and 15 with allergies). In addition, 13 other students were excluded because of providing incomplete information. Finally, a total of 829 children and their parents participated in this study.
Questionnaires were provided to the participants to fill out anonymously. The data gathered included the date of birth, weight, height, school type, sex, and history of chronic diseases.
Statistical analysis was performed in SPSS software (Statistical Package for Social Sciences, V 11.5). Mean and standard deviation were calculated for quantitative variables, and the frequency (percent) was used to describe qualitative variables. The chi-square test was used for the statistical analysis of categorical variables. A P value of < 0.05 was accepted as the statistical significance threshold.
4. Results
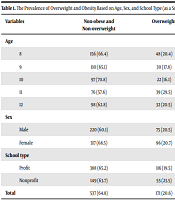
Of the students studied, 366 (44.1%) were boys, and 463 (55.9%) were girls. The mean age of the participants was 9.76 years, with a standard deviation of 1.48. The prevalence of overweight and obesity among the students was 20.6% and 14.6%, respectively (Table 1).
| Variables | Non-obese and Non-overweight | Overweight | Obese | P |
|---|---|---|---|---|
| Age | 0.19 | |||
| 8 | 156 (66.4) | 48 (20.4) | 31 (13.2) | |
| 9 | 110 (65.1) | 30 (17.8) | 29 (17.2) | |
| 10 | 97 (70.8) | 22 (16.1) | 18 (13.1) | |
| 11 | 76 (57.6) | 39 (29.5) | 17 (12.9) | |
| 12 | 98 (62.8) | 32 (20.5) | 26 (16.7) | |
| Sex | 0.002 | |||
| Male | 220 (60.1) | 75 (20.5) | 71 (19.4) | |
| Female | 317 (68.5) | 96 (20.7) | 50 (10.8) | |
| School type | 0.33 | |||
| Profit | 388 (65.2) | 116 (19.5) | 91 (15.3) | |
| Nonprofit | 149 (63.7) | 55 (23.5) | 30 (12.8) | |
| Total | 537 (64.8) | 171 (20.6) | 121 (14.6) |
The Prevalence of Overweight and Obesity Based on Age, Sex, and School Type (as a Socioeconomic Variable) a
The prevalence of obesity (19.4% vs. 10.8%) and overweight (26.5% vs. 20.7%) were higher among boys than girls. The chi-square test demonstrated that the prevalence of obesity and overweight varied by gender greatly (P = 0.002). The result demonstrated that 9-year-old children had the highest prevalence of obesity, but there was no significant relationship between age and the prevalence of obesity (P = 0.19, Table 1).
The prevalence of obesity was higher in children from public schools than in those studying in private schools, but the chi-square test demonstrated that there was no significant association between the prevalence of overweight and obesity and the type of the school as a socioeconomic indicator (P = 0.33).
5. Discussion
In this study, the highest prevalence of obesity was noted in 9-year-old children, but there was no significant relationship between age and prevalence of obesity.
The prevalence of obesity was higher in children from public schools than in those studying in private schools; however, the chi-square test showed that the prevalence of overweight and obesity did not significantly differ by the type of the school as a socioeconomic indicator. Public schools in Iran are run by the government, while private schools are run by independent individuals or organizations. The type of the school is generally considered a socioeconomic indicator, and children studying in private schools are assumed to have a higher socioeconomic status than their peers coming from public schools. Therefore, socioeconomic status may be associated with an increased prevalence of obesity in children studying in public schools (19). The economic status has been noted to be positively associated with obesity in developing countries.
This study investigated the prevalence of overweight and obesity among Iranian children aged 8-12 years in Tehran. According to our findings, the prevalence of overweight and obesity were 20.6% and 14.6%, respectively. The prevalence of obesity among Iranian children who are at the age of elementary school has recently increased (20, 21). Other studies have demonstrated that the prevalence of overweight and obesity in children varies greatly based on the region and country (9, 20). Generally, the prevalence of obesity has been reported to be higher in developed countries than in undeveloped countries (9).
The prevalence of childhood overweight and obesity in a study in Greece was 27.2% and 8.5%, respectively (22). Based on a study in the United States, the prevalence of obesity in 2011 - 2014 was 17.0% (95% CI: 15.5% - 18.6%), and the prevalence of extreme obesity was 5.8% (95% CI: 4.9% - 6.8%) (23).
In the United States, as a developed country, the prevalence of overweight and obesity in children was higher compared to developing countries (24). In India, a systematic review showed the prevalence of childhood overweight, and obesity was 19.3% in 2010, which was significantly higher than a previously reported prevalence (i.e., 16.3%) from 2001 - 2005 (25). In Nigeria, a study showed that the prevalence of overweight and obesity in children and adolescents was 7.5% and 2.1%, respectively. In another study by de Onis et al., the estimated prevalence of childhood overweight and obesity in Africa in 2010 was 8.5%, which was expected to reach 12.7% in 2020 (26). So, it can be concluded the prevalence of overweight and obesity has an increasing trend in the world. Differences in the prevalence of obesity and overweight between countries may be due to disparities in socioeconomic status and educational levels (20, 27).
In parallel with economic developments in countries, the prevalence of obesity seems to have risen (28). Industrialization and changes in lifestyle are among other reasons for the obesity epidemic (29). So, obesity and overweight are major public health concerns across the world (1).
In our study, obesity prevalence was relatively high, which is consistent with the reported increasing trend of obesity in Iran (27). Evidence shows that an epidemic of obesity is expected in Tehran, highlighting its importance as a public health concern (30). Inappropriate diets, overeating, food insecurity, and sedentary lifestyle seem to have contributed to this situation in Iran (31).
Therefore, preventive planning and policies are necessary to reduce epidemic waves of obesity (1, 26). It has been shown that appropriate interventions can reduce the prevalence of overweight and obesity (32).
In this study, the prevalence of obesity was higher in boys than in girls (19.4% vs. 10.8%). Also, the prevalence of overweight among girls and boys was 20.7% and 26.5%, respectively. A systematic review in Iran demonstrated that the prevalence of obesity was higher in boys than in girls (6.85% vs. 5.13%) (20). In studies in other regions of Iran, obesity prevalence was reported to be higher in girls than in boys (20, 33, 34). Physical activity level, behavioral, hormonal, physiological, social, and cultural elements, as well as the mental image of the body, can contribute to different BMIs between boys and girls (33, 35).
In this study, the highest prevalence of obesity was noted in 9-year-old children, but there was no significant relationship between age and the prevalence of obesity.
Obesity was more prevalent in children from public schools than those studying in private schools, but the chi-square test showed that the school type, as a socioeconomic indicator, was not significantly associated with the prevalence of overweight and obesity. Public schools in Iran are run by the government, while private schools are non-governmental organizations. The type of school is generally considered a socioeconomic indicator, and children studying in private schools are supposed to have a higher socioeconomic status than those studying in public schools. Therefore, there may be a link between socioeconomic status and the increased prevalence of obesity in public schools (19). The economic status has been noted to be positively associated with obesity in developing countries (36).
As a limitation of our study, the socioeconomic status of the children could not be cited due to the lack of accurate responses to questions such as monthly income, parents’ education, etc. So, the socioeconomic status was evaluated only based on the type of schools (private vs. public). Due to the importance of controlling childhood obesity, more community-based studies are recommended to analyze the current trend of obesity and implement more effective protocols in schools and society.
5.1. Conclusions
According to our results, childhood obesity and overweight are important health problems in Tehran. According to the findings of this study, the prevalence of overweight and obesity in Iranian children aged 8 - 12 years was directly related to gender, showing a higher prevalence in boys than in girls. On the other hand, no relationship was found between age and the prevalence of obesity and overweight. Considering the importance of the obesity epidemic in children and its probable complications, imposing medical expenses on families and the health system, it is essential to investigate obesity-related risk factors and to implement preventive planning to control obesity at the school level.
